



Diverticulitis is inflammation of 1 or more balloon-like sacs (diverticula). Infection may or may not develop.
Diverticulitis usually affects the large intestine (colon).
Left lower abdominal pain, tenderness, and fever are the typical symptoms.
The diagnosis is based on the results of a computed tomography (CT) scan, and colonoscopy is done after the episode of diverticulitis is over.
People with mild diverticulitis symptoms may be treated with rest, whereas those with severe symptoms are hospitalized for treatment with antibiotics given by vein and sometimes surgery.
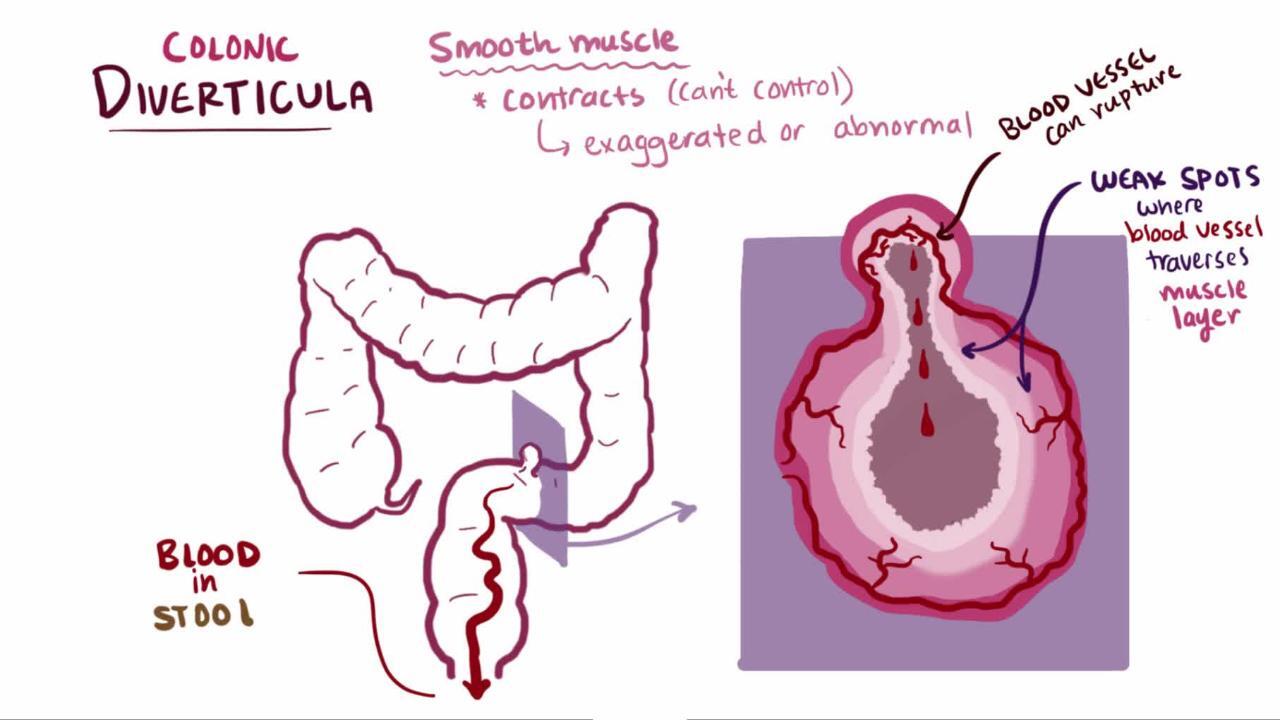
Diverticula in the large intestine occur when a defect develops in the thick, muscular middle layer of the bowel. The thin inner layers of the bowel bulge out through the defect and create a small sac. One sac is a diverticulum.
(See also Definition of Diverticular Disease.)


Diverticulitis is more common among people over 40 years old. In people over 50 years old, diverticulitis is most common among women. In people under 50 years old, diverticulitis is most common among men. Diverticulitis is more common among White people.
Diverticulitis can be severe in people of any age, although it is most serious in older adults, especially those taking corticosteroids or other medications that suppress the immune system and thus increase the risk of infection, including colon infection. People who have HIV infection and those undergoing chemotherapy are at increased risk of developing diverticulitis.

Causes of Diverticulitis
Diverticulitis occurs in people with diverticulosis when a diverticulum develops a small (sometimes microscopic) hole that allows bacteria from the intestines to be released. Some doctors think that a diverticulum can become inflamed even if a hole has not developed. Diverticulitis most commonly affects the sigmoid colon, which is the last part of the large intestine just before the rectum.
Doctors think there may be a connection between diverticulitis and the amount of red meat people eat per week, whether they smoke, and whether they have obesity. The use of nonsteroidal anti-inflammatory drugs (including aspirin), corticosteroids, and opioids also increases the risk of diverticulosis and diverticulitis.
Diverticulitis is not caused by eating nuts, seeds, corn, or popcorn.
Symptoms of Diverticulitis
Symptoms of diverticulitis typically include pain and/or tenderness (usually in the left lower part of the abdomen), fever, and sometimes nausea and vomiting. Diverticulitis typically does not cause gastrointestinal bleeding.
Complications of diverticulitis
Complications of diverticulitis include
Fistulas
Abscess
Peritonitis
Narrowing (stricture)
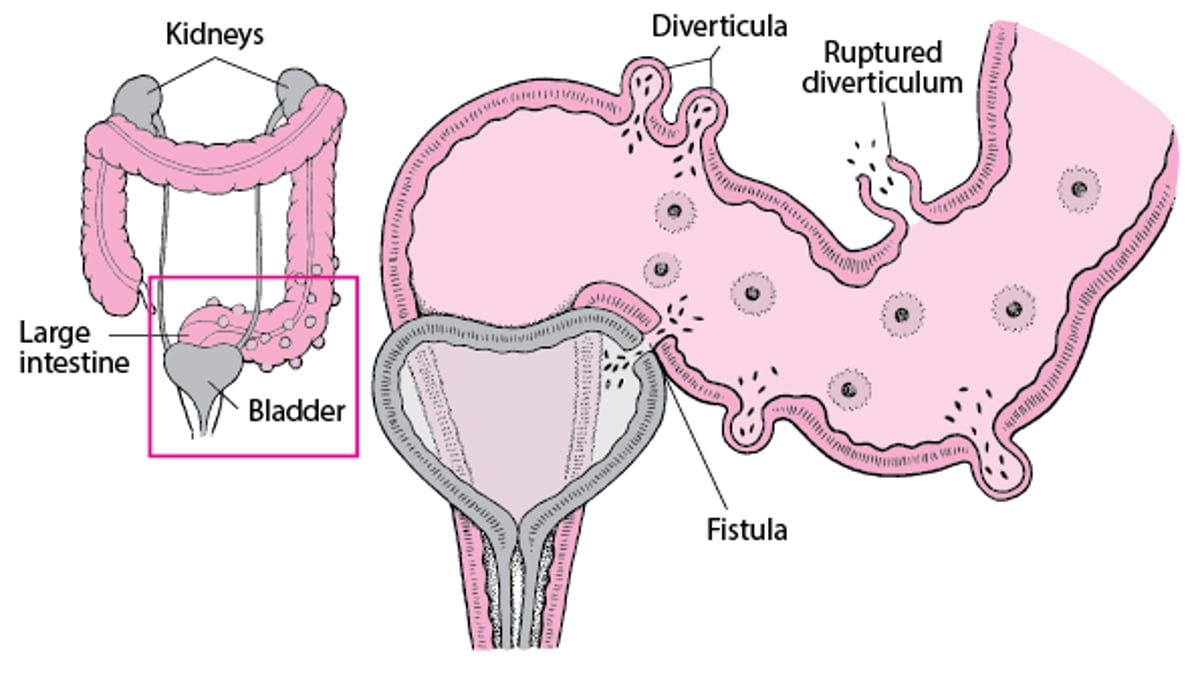
A fistula is an abnormal channel connecting 1 organ with another or with the skin. Intestinal inflammation from diverticulitis can lead to the development of fistulas that connect the large intestine with other organs.
Fistulas usually form when an inflamed diverticulum in the large intestine is touching another organ (such as the bladder). The resulting inflammation along with the bacterial contents of the large intestine slowly penetrate the nearby organ, resulting in a fistula.
Most fistulas form between the sigmoid colon and the bladder. These fistulas are more common among men than women, although women who have had a hysterectomy (removal of the uterus) are at increased risk because the large intestine and bladder are no longer separated by the uterus. When fistulas form between the large intestine and bladder, intestinal contents, including normal bacteria, enter the bladder and cause urinary tract infections.
Less commonly, a fistula can develop between the large intestine and the small intestine, uterus, vagina, abdominal wall, or even the thigh.
Complications of Diverticulitis
In diverticular disease, a diverticulum may bleed into the intestine. If a diverticulum ruptures, the contents of the intestine, including bacteria and blood, spill into the abdominal cavity, often causing infection. An abnormal channel (fistula) may form between the large intestine and another organ such as the bladder, usually when a diverticulum that touches another organ ruptures. |

An abscess is a pocket of pus. An abdominal abscess can form around an inflamed diverticulum, causing worsened pain and fever.
Peritonitis is infection of the abdominal cavity, which can develop if the wall of a diverticulum ruptures.
Other possible complications of diverticulitis include inflammation of nearby organs (such as the uterus, bladder, or other areas of the digestive tract). Repeated bouts of diverticulitis can lead to narrowing (stricture) of the colon because the resulting scarring and muscle thickening can narrow the inside of the large intestine and prevent solid stool from passing through.
Diagnosis of Diverticulitis
Computed tomography (CT) of the abdomen and pelvis
Colonoscopy after episode has ended
If a doctor knows that the person already has diverticulosis, a diverticulitis diagnosis may be based almost entirely on the symptoms. However, many other conditions involving the large intestine and other organs in the abdomen and pelvis can cause symptoms similar to diverticulitis, including appendicitis, colon cancer or ovarian cancer, an abscess not related to diverticulitis, and noncancerous (benign) growths on the wall of the uterus (uterine fibroids).
A CT scan of the abdomen and pelvis may be helpful in determining that the problem is diverticulitis and not appendicitis or another diagnosis. Magnetic resonance imaging (MRI) is an alternative test for pregnant women or young people. Sometimes an ultrasound study is done in an emergency department or urgent care facility.
Once inflammation has subsided or the infection has been treated, a doctor may do a colonoscopy (an examination of the large intestine using a flexible viewing tube) to rule out colon cancer. The colonoscopy may be done if people have complications (such as a perforation or abscess) or if they have risk factors for cancer (such as narrowed stool, bleeding, anemia, weight loss, or a family history of colon cancer). Colonoscopy usually needs to be delayed for 1 to 3 months after treatment because it can damage or rupture an inflamed intestine. Exploratory surgery is rarely needed to confirm the diagnosis.


This photo shows a diverticulum with a clotted blood vessel (left) that caused lower gastrointestinal bleeding. Placement of an endoclip (right) during colonoscopy stopped the bleeding.
Photos courtesy of Drs. Joel A. Baum and Rafael A. Ching Companioni.
Treatment of Diverticulitis
For mild diverticulitis, rest
For severe diverticulitis, no food or fluids by mouth and antibiotics
Sometimes surgery
Mild diverticulitis can be treated at home with rest. Diverticulitis symptoms usually lessen rapidly. People who do not have complications may consume clear liquids for 2 to 3 days and then may eat low-fiber foods once their pain lessens.
Severe diverticulitis requires different treatment. People who have severe symptoms, such as abdominal pain, body temperature above 101° F (38.3° C), and other evidence of serious infection or complications, are hospitalized. In the hospital, people are given fluids and antibiotics by vein (intravenously), kept on bed rest, and given nothing by mouth until the symptoms subside. People stay in the hospital until their symptoms go away. They can then eat soft foods. Once the episode has ended, people can eat high-fiber foods. To decrease the risk of recurrence, people should avoid using nonsteroidal anti-inflammatory drugs (NSAIDs).
After 1 to 3 months, people have a colonoscopy to evaluate the colon.
For some people, including those who have small abscesses, rest and sometimes antibiotics are all that are needed to treat severe diverticulitis.
Drainage for abscesses
Larger abscesses and abscesses that do not go away with only antibiotics or are getting worse are drained with a needle inserted through the skin and guided by a CT scan or an endoscopic ultrasound.
If drainage helps, people remain in the hospital until symptoms have been relieved and they have resumed a soft diet. If drainage does not help, people need surgery.
Surgery for diverticulitis
Emergency surgery is necessary for people whose intestine has ruptured or who have peritonitis. Other people who need surgery include those who have severe diverticulitis symptoms that are not relieved by nonsurgical treatment (such as antibiotics) within 3 to 5 days. People who have increasing pain, tenderness, and fever also need surgery.
The surgeon removes the involved section of the intestine. The ends are rejoined immediately in healthy people who do not have a perforation, abscess, or severe intestinal inflammation. Other people need a temporary colostomy.
A colostomy is an opening between the large intestine and the skin surface. About 10 to 12 weeks later (or sometimes longer), after the inflammation has gone away and the person's condition has improved, the cut ends of the intestine are rejoined during a follow-up operation, and the colostomy is closed.
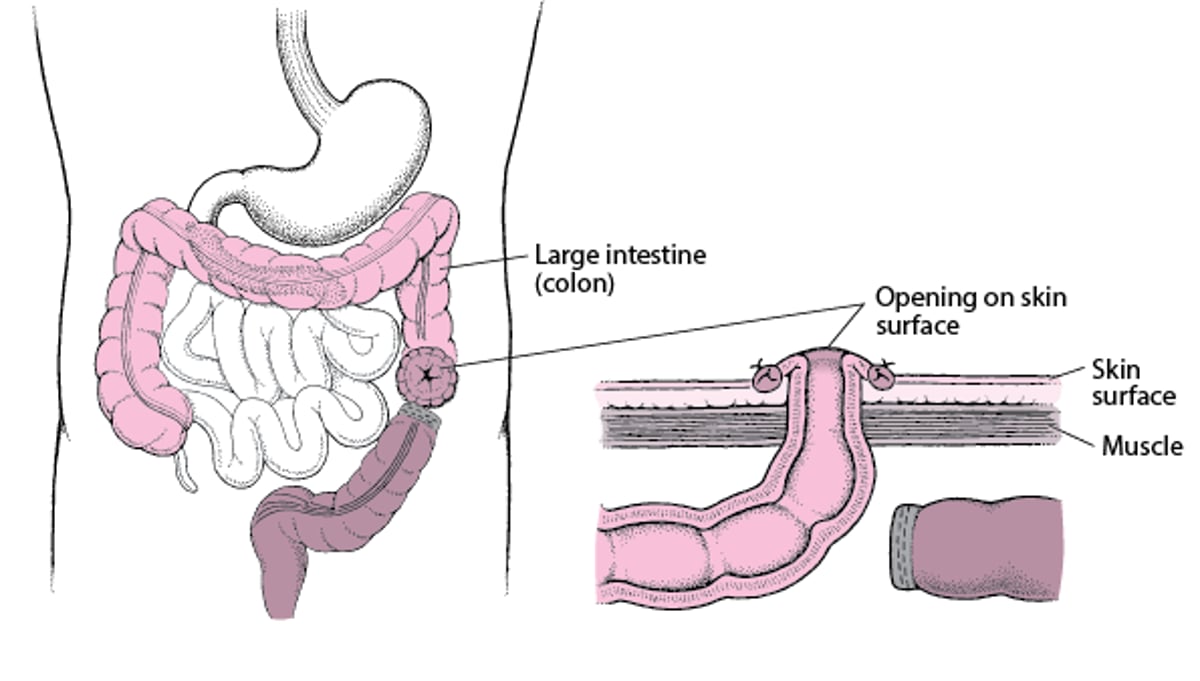
Understanding Colostomy
In a colostomy, the large intestine (colon) is cut. The healthy end of the large intestine, which is before the blockage, is brought to the skin surface through a surgically created opening in the abdominal wall. It is then stitched to the skin of the opening. Stool passes through the opening and into a disposable bag. The colostomy allows the remaining part of the large intestine to rest while the person recovers. After the person recovers from the surgery and the colon heals, the 2 ends can be reattached so that stool can pass normally. |

Fistula treatment involves removing the section of large intestine where the fistula begins, rejoining the cut ends of the large intestine, and repairing the other affected area (for example, the bladder or small intestine).
Sometimes, after talking with their doctor, people choose to have elective surgery (surgery that is not needed immediately and can be put off for some time) to manage their diverticular disease. Elective surgery is typically considered for people who have had multiple attacks of diverticulitis or for those who have a complication such as narrowing of the colon due to scarring.





