


Flail chest is multiple fractures in 3 adjacent ribs that result in a segment of the chest wall separating from the rest of the thoracic cage; it is a marker for injury to the underlying lung.
(See also Overview of Thoracic Trauma.)
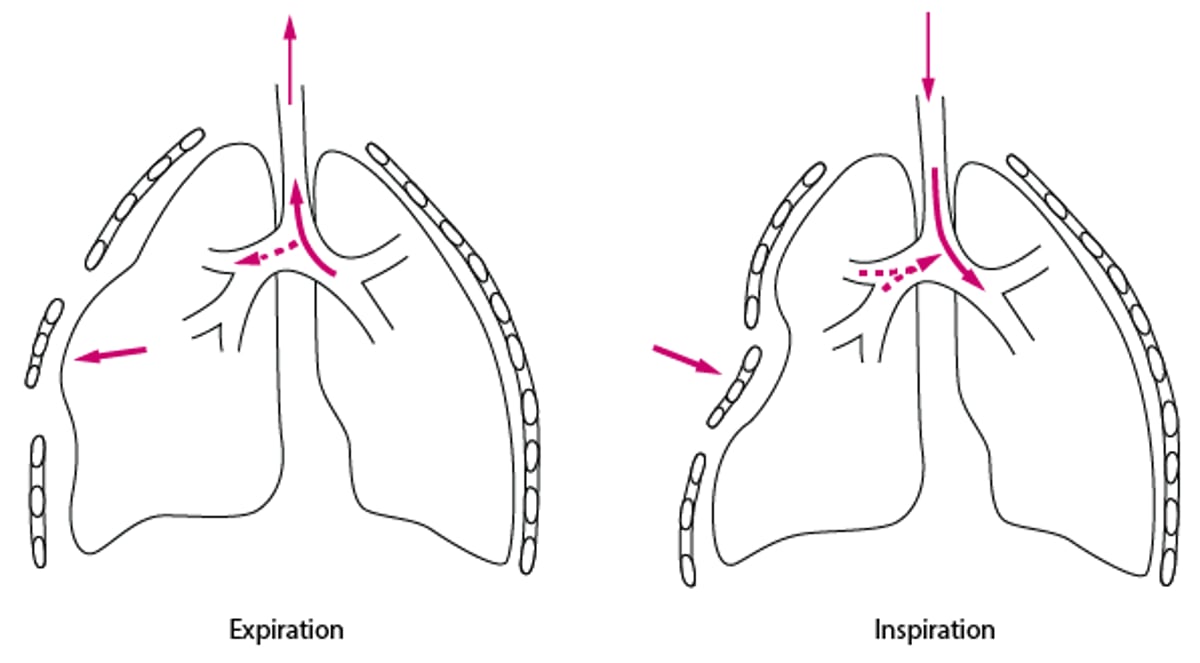
A single rib may fracture in more than one place. If multiple (3 or more) adjacent ribs fracture in ≥ 2 places, the breaks in each rib result in a segment of chest wall that is not mechanically connected to the rest of the thoracic cage (flail segment). This flail segment moves paradoxically (ie, outward during expiration and inward during inspiration—see figure Flail Chest).
Patients are at high risk for respiratory complications, mainly because the large amount of force required to cause a flail chest typically causes a significant underlying pulmonary contusion. In addition, the paradoxical motion of flail chest increases the work of breathing, and chest wall pain tends to limit deep inspiration and thus maximal ventilation.
Flail Chest

Diagnosis of Flail Chest
History and physical examination
Diagnosis of flail chest is clinical, ideally by observing the paradoxical motion of the flail segment during breathing. However, this motion may be difficult to see if inspiratory depth is limited by pain or obtundation due to other injuries. The paradoxical motion does not occur if the patient is mechanically ventilated, but the flail segment may be identified by its more extreme outward movement during lung inflation. Palpation can often detect crepitus of the flail segment and confirm abnormal chest wall motion.
Chest x-ray can help confirm bone fractures and usually shows underlying pulmonary contusion; x-ray does not show cartilaginous disruption.
Treatment of Flail Chest
Supportive care
Sometimes mechanical ventilation
Sometimes rib fracture repair
Humidified oxygen is given to patients with flail chest. Analgesics may help improve ventilation by decreasing pain during breathing, but ventilation may need to be supported mechanically. Volume status should be closely monitored because harm can result from either hypovolemia (due to lung hypoperfusion) or hypervolemia (due to pulmonary edema). In select patients with flail chest (those who cannot be weaned from the ventilator, those with significant chest wall deformity, those who have impending respiratory failure despite pain control, or those who require thoracotomy for other reasons), operative fixation of ribs appears to reduce the risk of pneumonia, length of hospital stay, duration of mechanical ventilation, and death (1– 4 ).
Treatment references
1. Simon B, Ebert J, Bokhari F, et al: Management of pulmonary contusion and flail chest: An Eastern Association for the Surgery of Trauma practice management guideline. J Trauma and Acute Care Surgery 73(5 Suppl 4):S351-S361, 2012. doi: 10.1097/TA.0b013e31827019fd
2. Kasotakis G , Hasenboehler EA, Streib EW, et al: Operative fixation of rib fractures after blunt trauma: A practice management guideline from the Eastern Association for the Surgery of Trauma. J Trauma Acute Care Surg 82(3):618-626, 2017. doi: 10.1097/TA.0000000000001350
3. Dehghan N, Nauth A, Schemitsch E, et al: Operative vs nonoperative treatment of acute unstable chest wall injuries: A randomized clinical trial. JAMA Surg 157(11):983, 2022. doi: 10.1001/jamasurg.2022.4299
4. Coughlin TA, Ng JWG, Rollins KE, et al: Management of rib fractures in traumatic flail chest: A meta-analysis of randomised controlled trials. Bone Joint J 8-B(8):1119-1125, 2016. doi: 10.1302/0301-620X.98B8.37282






