



Pleural fibrosis and calcification are usually benign sequelae of pleural inflammation or asbestos exposure.
Pleural fibrosis and calcification can be either:
Postinflammatory
These disorders are suspected and diagnosed based on imaging studies. Treatment of fibrosis and calcification themselves is generally unnecessary. Rarely, very large, symptomatic areas of fibrosis require surgical removal.
Postinflammatory
Pleural inflammation commonly causes acute pleural thickening due to fibrosis. Common causes of pleural inflammation include untreated infection, drug adverse effects (eg, methylsergide), autoimmune conditions (eg, rheumatoid pleuritis or IgG4 disease), and exposures including asbestos (benign asbestos pleural disease). In some cases, the thickening and fibrosis will largely resolve, especially if the underlying disease is treated (eg, adequate drainage and antibiotics in pleural infection). Some patients are left with minor degrees of pleural thickening, which usually causes no symptoms or impairment of lung function. In other cases, there may be long-term, progressive and increasingly symptomatic pleural fibrosis and thickening. Occasionally, the lung becomes encased with a thick, fibrous pleural peel that limits expansion ("trapped lung"), pulls the mediastinum toward the side of disease, and impairs pulmonary function.
Chest radiograph shows asymmetry of the lungs with thickened pleura (trapped lung). Differentiating localized pleural thickening from loculated pleural fluid may be difficult on radiograph, but this differentiation is easily made with CT.

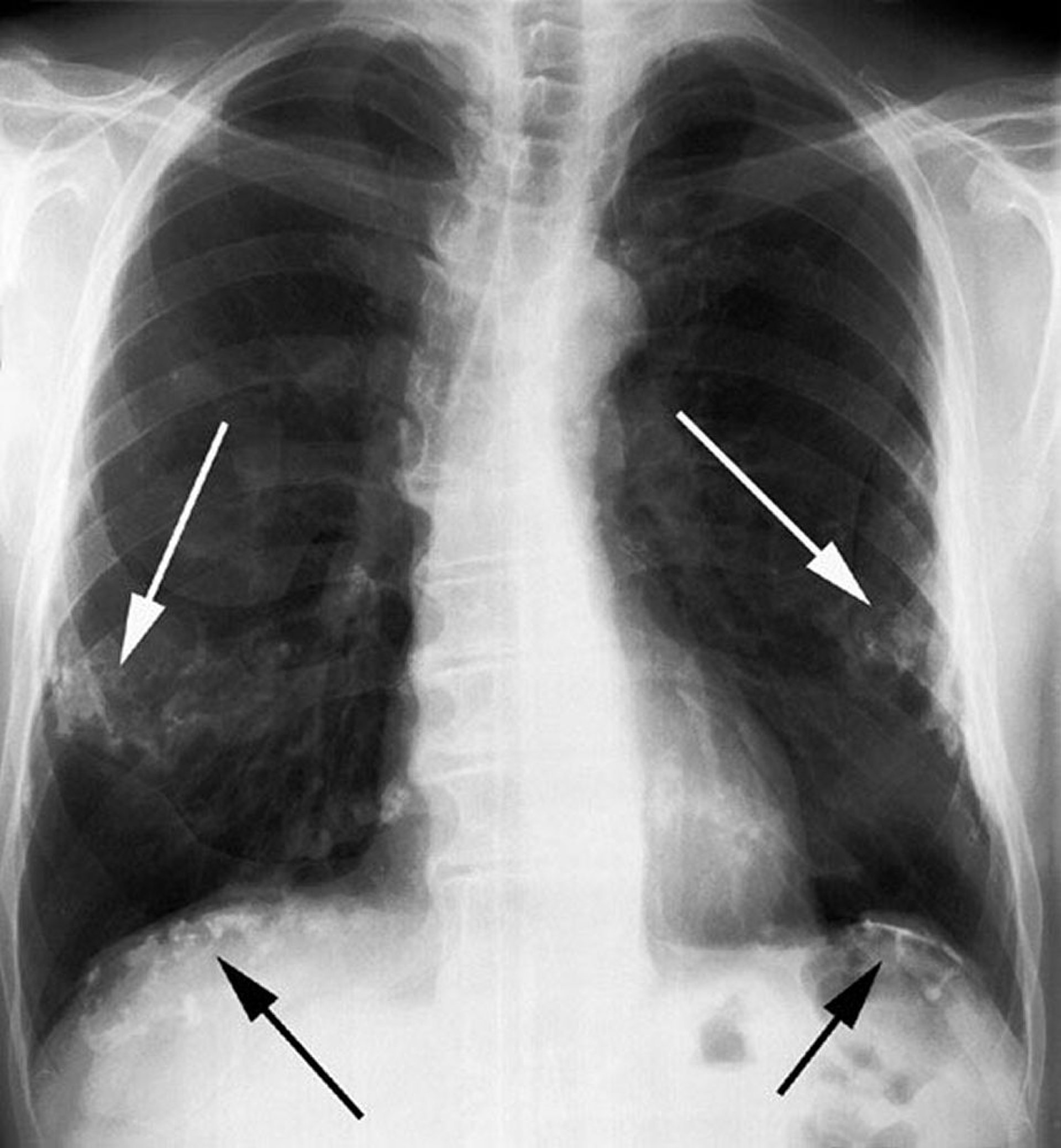
Calcified pleural plaques on chest wall and diaphragm.
Image courtesy of David W. Cugell, MD.
Pleural fibrosis after inflammation can, on occasion, calcify. Calcification produces a dense image on the chest radiograph and almost always involves the visceral pleura. Postinflammatory calcifications are invariably unilateral.
Asbestos-related
Exposure to asbestos can lead to focal, plaquelike pleural fibrosis, at times with calcification, occurring up to ≥ 20 years after the initial exposure.


Pleural thickening is seen on the right in this CT scan.
Image courtesy of Najib M. Rahman, BMBCh MA (oxon) DPhil.
Diagnosis is usually by chest radiograph. The diameter of the plaques can vary from several millimeters to 10 cm. Any pleural or pericardial surface can be affected, but asbestos-related pleural plaques are usually in the lower two-thirds of the thorax and are bilateral. Calcification most often affects the parietal and diaphragmatic pleura and spares the costophrenic sulci and apices. Calcification may be the only evidence of exposure. Dense pleural fibrosis surrounding the entire lung and > 1 cm in thickness can also follow asbestos exposure.





