



Etiology of stomach cancer is multifactorial, but Helicobacter pylori plays a significant role. Symptoms include early satiety, obstruction, and bleeding but tend to occur late in the disease. Diagnosis is by endoscopy, followed by CT and endoscopic ultrasound for staging. Treatment is surgery sometimes in combination with chemotherapy or chemoradiation. Long-term survival is poor except for patients with local disease.
Gastric adenocarcinoma accounts for 95% of malignant tumors of the stomach; less common are localized gastric lymphomas, gastrointestinal stromal tumors, and leiomyosarcomas.
Stomach cancer is the fifth most common cancer worldwide, but the incidence varies widely. Incidence is extremely high in Eastern Asia (with Mongolia having the highest incidence rate) and Eastern Europe, and lowest in Africa (1). In the United States, incidence has declined in recent decades.
Stomach cancer accounted for an estimated 26,890 cases and 10,880 deaths in the United States in 2024, making gastric cancer the 16th most commonly diagnosed cancer and the 17th leading cause of cancer-related death in the United States (2).
In the United States, stomach cancer is most common among Black, Hispanic, and American Indian people. Its incidence increases with age.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229-263. doi:10.3322/caac.21834
2. Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024 [published correction appears in CA Cancer J Clin. 2024 Mar-Apr;74(2):203. doi: 10.3322/caac.21830]. CA Cancer J Clin. 2024;74(1):12-49. doi:10.3322/caac.21820
Etiology of Stomach Cancer
Risk factors for stomach cancer include the following:
Helicobacter pylori infection (when it is associated with extensive gastric intestinal metaplasia)
Smoking (and people who smoke may have an impaired response to treatment)
Gastric polyps
Genetic factors
Dietary factors are not proven causes; however, the World Health Organization (WHO) International Agency for Research on Cancer (IARC) has reported a positive association between consumption of processed meat and stomach cancer (1).
Gastric polyps can be precursors of cancer. Inflammatory polyps may develop in patients taking nonsteroidal anti-inflammatory drugs (NSAIDs), and fundic foveolar polyps are common among patients taking proton pump inhibitors. Adenomatous polyps, particularly multiple ones, although rare, are the most likely to develop cancer. Cancer is particularly likely if an adenomatous polyp is > 2 cm in diameter or has a villous histology.
Various genetic factors are also risk factors. Hereditary diffuse gastric cancer is associated with a mutation in the cadherin 1 gene (CDH1) and has no precursor lesion. This mutation is an autosomal dominant trait with high penetrance. Affected patients usually develop gastric cancer at an early age (average age 38) and have approximately an 80% lifetime risk of developing gastric cancer (2). Affected women are also at high risk of developing lobular breast cancer. Patients with personal or family history of diffuse gastric cancer and/or lobular breast cancer in multiple family members, especially if they were diagnosed before age 50, should be referred for genetic counseling and testing. Prophylactic gastrectomy should be offered to asymptomatic carriers of the CDH1 mutation between the ages of 18 and 40 (3). Breast cancer surveillance with annual breast MRI beginning at age 30 is also recommended for women with the CDH1 mutation (4). There are case reports of colorectal cancer in CDH1 mutation carriers. Data are insufficient to recommend colon cancer screening of all carriers or their families; however, if colon cancer has been diagnosed in a carrier, their family members should have colon cancer screening beginning at age 40 or at an age 10 years younger than when the youngest family member was diagnosed (4). Other genetic syndromes that predispose to stomach cancer include familial adenomatous polyposis, Lynch syndrome, juvenile polyposis syndrome, and Peutz-Jeghers syndrome.
Risk factor references
1. Bouvard V, Loomis D, Guyton KZ, et al. Carcinogenicity of consumption of red and processed meat. Lancet Oncol. 16(16):1599–1600, 2015. doi: 10.1016/S1470-2045(15)00444-1
2. Pharoah PD, Guilford P, Caldas C; International Gastric Cancer Linkage Consortium. Incidence of gastric cancer and breast cancer in CDH1 (E-cadherin) mutation carriers from hereditary diffuse gastric cancer families. Gastroenterology.121(6):1348-1353, 2001. doi: 10.1053/gast.2001.29611
3. Shepard B, Yoder L, Holmes C. Prophylactic total gastrectomy for hereditary diffuse gastric cancer. ACG Case Rep J. 3(4):e179, 2016. doi: 10.14309/crj.2016.152
4. van der Post RS, Vogelaar IP, Carneiro F, et al. Hereditary diffuse gastric cancer: Updated clinical guidelines with an emphasis on germline CDH1 mutation carriers. J Med Genet. 52(6):361–374, 2015. doi: 10.1136/jmedgenet-2015-103094
Pathophysiology of Stomach Cancer
Gastric adenocarcinomas can be classified by gross appearance:
Protruding: The tumor is polypoid or fungating.
Penetrating: The tumor is ulcerated.
Superficial spreading: The tumor spreads along the mucosa or infiltrates superficially within the wall of the stomach.
Linitis plastica: The tumor infiltrates the stomach wall with an associated fibrous reaction that causes a rigid “leather bottle” stomach.
Miscellaneous: The tumor shows characteristics of ≥ 2 of the other types; this classification is the largest.
Prognosis is better with protruding tumors than with spreading tumors because protruding tumors become symptomatic earlier.

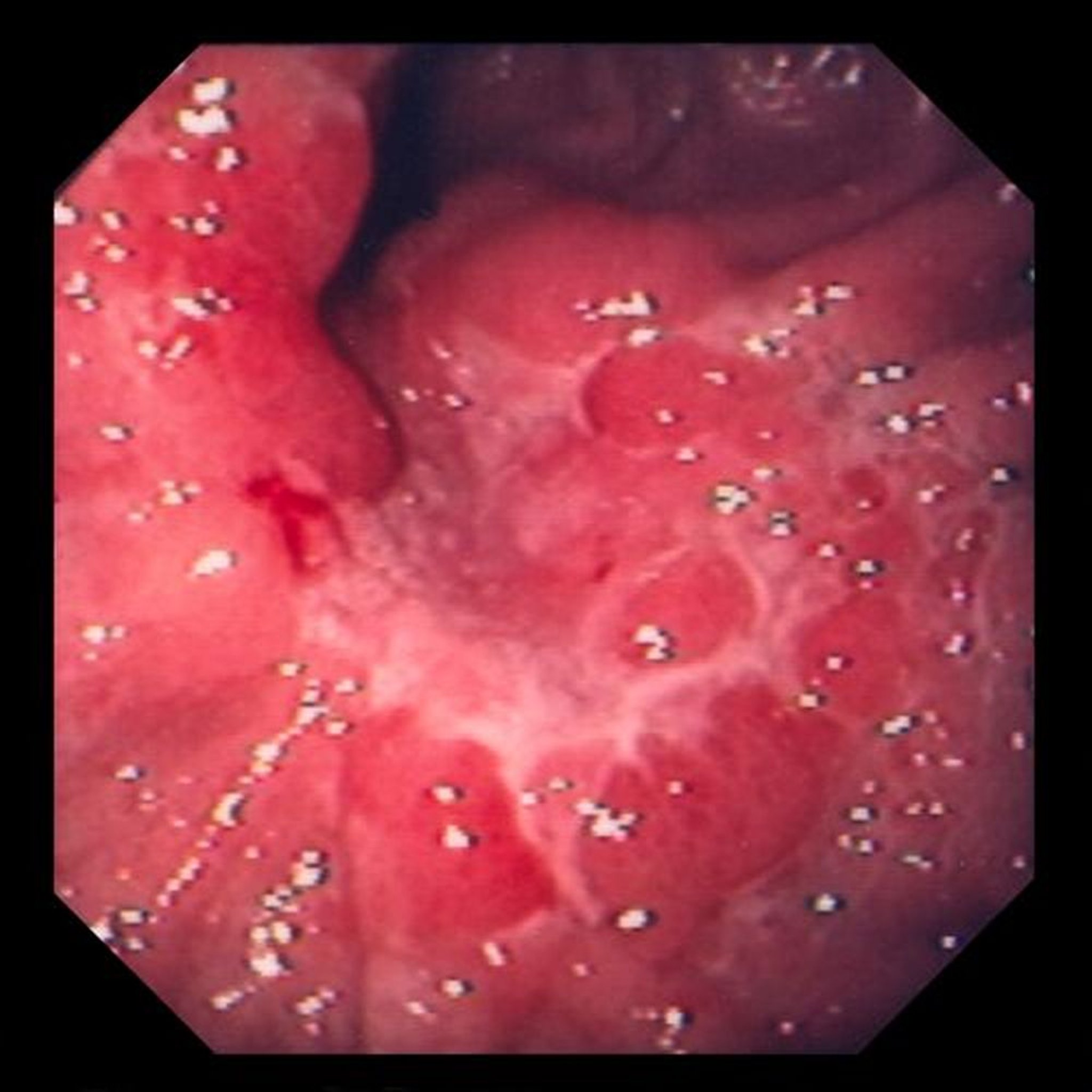
This image shows an ulcer within edematous mucosal folds, which, on biopsy, turned out to be poorly differentiated adenocarcinoma (signet ring cell type).
Image provided by David M. Martin, MD.
Symptoms and Signs of Stomach Cancer
Initial symptoms of stomach cancer are nonspecific, often consisting of dyspepsia suggestive of peptic ulcer. Patients and physicians alike tend to dismiss symptoms or treat the patient for acid disease.
Later, early satiety (fullness after ingesting a small amount of food) may occur if the cancer obstructs the pyloric region or if the stomach becomes nondistensible secondary to linitis plastica. Dysphagia may result if cancer in the cardiac region of the stomach obstructs the esophageal outlet. Loss of weight or strength, usually resulting from dietary restriction, is common. Massive hematemesis or melena is uncommon, but secondary anemia may follow occult blood loss. Occasionally, the first symptoms are caused by metastasis (eg, jaundice, ascites, fractures).
Physical findings may be unremarkable or limited to heme-positive stools. Late in the course, abnormalities include an epigastric mass; umbilical, left supraclavicular, or left axillary lymph nodes; hepatomegaly; and an ovarian or rectal mass. Pulmonary, central nervous system, and bone lesions may occur.
Diagnosis of Stomach Cancer
Endoscopy with biopsy
Then CT and endoscopic ultrasound
Differential diagnosis of stomach cancer commonly includes peptic ulcer and its complications.
Patients suspected of having stomach cancer should have endoscopy with multiple biopsies and brush cytology. Occasionally, a biopsy limited to the mucosa misses tumor tissue in the submucosa. Radiographs, particularly double-contrast barium studies, may show lesions but rarely obviate the need for subsequent endoscopy.
Patients in whom cancer is identified require CT of the chest and abdomen to determine extent of tumor spread. If CT is negative for metastasis, endoscopic ultrasound should be done to determine the depth of the tumor and regional lymph node involvement. Findings guide therapy and help determine prognosis.
Basic blood tests, including complete blood count, electrolytes, and liver tests, should be done to assess anemia, hydration, general condition, and possible liver metastases. The carcinoembryonic antigen (CEA) level should be measured before and after surgery.
Screening
Screening with endoscopy is used in high-risk populations (eg, Japanese) but is not recommended in the United States.
Follow-up screening for recurrence in treated patients consists of endoscopy and CT of the chest, abdomen, and pelvis.
Treatment of Stomach Cancer
Surgical resection, sometimes combined with chemotherapy, radiation, or both (chemoradiation)
Stomach cancer treatment decisions depend on tumor staging and the patient’s wishes (some may choose to forgo aggressive treatment—see Advance Directives).
Curative surgery involves removal of most (subtotal gastrectomy) or all (total gastrectomy) of the stomach and adjacent lymph nodes and is reasonable in patients with disease limited to the stomach and perhaps the regional lymph nodes (< 50% of patients) (1). Patients often receive perioperative chemotherapy (ie, before surgery and after surgery) typically with the FLOT regimen (5-fluorouracil, leucovorin, oxaliplatin, docetaxel) (2).
For patients with inadequate lymphadenectomy or with node-positive or incompletely resected disease, adjuvant chemotherapy or chemoradiation is sometimes used.
Metastasis or extensive nodal involvement precludes curative surgery, and, at most, palliative procedures should be undertaken. However, the true extent of tumor spread often is not recognized until curative surgery is attempted. Palliative surgery typically consists of a gastroenterostomy to bypass a pyloric obstruction and should be done only if the patient’s quality of life can be improved. In patients not undergoing surgery, various combination chemotherapy regimens (5-fluorouracil, capecitabine, doxorubicin, mitomycin, cisplatin, oxaliplatin, irinotecan, paclitaxel, docetaxel, or leucovorin) may produce a temporary response and only a minor improvement in survival.
For advanced disease with tumors that express human epidermal growth factor receptor 2 (HER2+), trastuzumab (a monoclonal antibody that targets HER2) or ramucirumab (a vascular endothelial growth factor [VEGF] inhibitor) in conjunction with chemotherapy may be used. Immunotherapy such as with pembrolizumab is available for use in patients with programmed cell death ligand 1 (PD-L1)–positive advanced or metastatic gastric cancer. Programmed cell death receptor 1 inhibitors (eg, nivolumab) are available for use outside the United States for patients with advanced gastric cancer. Radiation therapy is of limited benefit for patients with metastases.
Treatment references
1. Ajani JA, D'Amico TA, Bentrem DJ, et al. Gastric Cancer, Version 2.2022, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2022 Feb;20(2):167-192. doi: 10.6004/jnccn.2022.0008
2. Al-Batran SE, Homann N, Pauligk C, et al. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): A randomised, phase 2/3 trial. Lancet. 393(10184):1948-1957, 2019. doi: 10.1016/S0140-6736(18)32557-1
Prognosis for Stomach Cancer
Prognosis depends greatly on stage but overall is poor (5-year survival: < 5 to 15%) because most patients present with advanced disease. Median overall survival in well-selected patients after perioperative chemotherapy and surgery can be as high as 50 months based on modern randomized trials (1, 2). If the tumor is limited to the mucosa or submucosa, 5-year survival may be as high as 95% (3). For tumors involving local lymph nodes, survival is correlated with the number of involved nodes. More widespread disease is almost always fatal within 6 to 12 months.
Gastric lymphomas have a better prognosis (see Mucosa-Associated Lymphoid Tissue (MALT) Lymphoma and Non-Hodgkin Lymphomas).
Prognosis references
1. Cunningham D, Allum WH, Stenning SP, et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med. 355(1):11-20, 2006. doi: 10.1056/NEJMoa055531
2. Al-Batran SE, Homann N, Pauligk C, et al. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): A randomised, phase 2/3 trial. Lancet. 393(10184):1948-1957, 2019. doi: 10.1016/S0140-6736(18)32557-1
3. Zhang J, Zhou Y, Jiang K, et al. Evaluation of the seventh AJCC TNM staging system for gastric cancer: a meta-analysis of cohort studies. Tumour Biol. 35(9):8525-8532, 2014. doi: 10.1007/s13277-014-1848-6
Key Points
Helicobacter pylori infection is a risk factor for some stomach cancers.
Initial symptoms are nonspecific and often resemble those of peptic ulcer disease.
Screening with endoscopy is used in high-risk populations (eg, Japanese) but is not recommended in the United States.
Curative surgery, perhaps with combined chemotherapy and radiation therapy, is reasonable in patients with disease limited to the stomach and perhaps the regional lymph nodes.
Overall, survival is poor (5-year survival: 5 to 15%) because many patients present with advanced disease.
Drug Information for the Topic





