



Basal cell carcinoma typically presents as a superficial, slowly growing papule or nodule that derives from certain epidermal cells. Basal cell carcinomas arise from keratinocytes near the basal layer, which are sometimes called basaloid keratinocytes. Metastasis is rare, but local growth can be highly destructive. Diagnosis is suspected on clinical appearance and confirmed by biopsy. Treatment depends on the tumor’s characteristics and may involve curettage and electrodesiccation, surgical excision, cryosurgery, topical chemotherapy, or, occasionally, radiation therapy or medications.
(See also Overview of Skin Cancer.)
Basal cell carcinoma, a keratinocyte skin cancer, is the most common type of skin cancer, with approximately 2 million new cases yearly in the United States (1). There is a particularly high burden among people with light skin with a history of sun exposure. Basal cell carcinoma is very rare in people with darkly pigmented skin. Men are affected more frequently than women, and prevalence rises with increasing age (2). In resource-rich regions, the prevalence of basal cell carcinoma has increased over time.

This photo shows a nevus sebaceus (a type of birthmark that usually appears on the scalp). This benign congenital skin discoloration is due to pigmentation and is composed of sebaceous gland tissue.
DR P. MARAZZI / SCIENCE PHOTO LIBRARY
General references
1. Asgari MM, Moffet HH, Ray GT, Quesenberry CP. Trends in Basal Cell Carcinoma Incidence and Identification of High-Risk Subgroups, 1998-2012. JAMA Dermatol 151(9):976-981, 2015. doi: 10.1001/jamadermatol.2015.1188
2. Verkouteren JAC, Ramdas KHR, Wakkee M, et al. Epidemiology of basal cell carcinoma: scholarly review. Br J Dermatol. 2017 Aug;177(2):359-372. doi: 10.1111/bjd.15321. Epub 2017 Feb 20. PMID: 28220485.
Pathophysiology of Basal Cell Carcinoma
Basal cell carcinoma arises primarily from an interplay between environmental and genetic factors. Basal cell carcinomas are also associated with genetic syndromes and may arise in a nevus sebaceus. Xeroderma pigmentosum represents an inherited defect in DNA repair that can result in nonmelanoma skin cancer and in melanoma. Basal cell nevus syndrome (Gorlin syndrome) is an autosomal dominant disorder that results in multiple basal cell carcinomas as well as in medulloblastomas, meningiomas, breast cancers, non-Hodgkin lymphomas, and ovarian cancers. Bazex-Dupré-Christol syndrome is a rare X-linked genodermatosis characterized by a triad of early onset of multiple basal cell carcinomas, follicular atrophoderma, and hypotrichosis.
Most basal cell carcinomas are caused by aberrant activation of the Hedgehog signaling (most commonly due to loss-of-function mutations in the PTCH1 gene). The most significant environmental risk factor is UV (both UVA and UVB) radiation, in particular, intermittent and intense sun exposure during childhood and adolescence. Less frequently implicated environmental factors include exposure to arsenic and profound immunosuppression (especially organ transplantation).
Symptoms and Signs of Basal Cell Carcinoma
The clinical manifestations of basal cell carcinomas are highly variable.
Most commonly, the carcinoma begins as a shiny papule, enlarges slowly, and, after a few months or years, shows a shiny, pearly border with prominent engorged vessels (telangiectases) on the surface and a central dell (ie, central depression) or ulcer. The carcinomas often alternately crust and heal, which may unjustifiably decrease patient and physician concerns about the seriousness of the lesion. Recurrent itching, crusting, or bleeding is not unusual. Most lesions are painless and nontender to palpation. Chronic nonhealing lesions, particularly in sun-exposed skin, should prompt consideration of basal cell carcinoma.
Basal-cell carcinoma lesions typically occur in sun-exposed areas (1). Lesions occur most commonly on the head and neck (80% of cases), followed by the trunk (15%), and less commonly on the arms and legs. The palms and soles are typically spared, and involvement of the axillary, mammary, or genital regions is rare.
There are several types of basal cell carcinomas. The most common types are (2):
Nodular (approximately 51% of basal cell carcinomas): These types are small, shiny, firm, almost translucent to pink nodules with telangiectases, usually on the face or other sun-exposed areas. Ulceration and crusting are common.
Superficial (approximately 34%): These types are red or pink, marginated, thin papules or plaques, commonly on the trunk, that can be mistaken for psoriasis or other localized dermatitis.
Morpheaform and infiltrative (5 to 10%): These types are flat, scarlike, indurated plaques that can be flesh-colored or light red and have vague borders. They are considered high-risk because of their tendency for deeper invasion and higher recurrence risk.
Mixed: This type includes histopathologic features of more than one subtype.
Other: Other types are possible (eg, micronodular, basosquamous). Nodular and superficial basal cell carcinomas can produce pigment (sometimes called pigmented basal cell carcinomas).

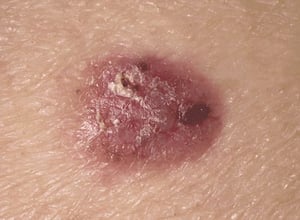
This photo shows a superficial, slowly growing, ulcerated nodule.
This photo shows a superficial, slowly growing, ulcerated nodule.
Photo provided by Thomas Habif, MD.


This lesion usually appears as a firm, pearly, dome-shaped nodule often displaying multiple telangiectatic vessels coursing over its borders.
This lesion usually appears as a firm, pearly, dome-shaped nodule often displaying multiple telangiectatic vessels cour
© Springer Science+Business Media


This photo shows a superficial basal cell carcinoma on the forehead of a patient. This lesion involves only the epidermis.
This photo shows a superficial basal cell carcinoma on the forehead of a patient. This lesion involves only the epiderm
RICHARD USATINE MD / SCIENCE PHOTO LIBRARY

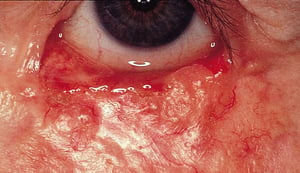
This basal cell carcinoma appears as a flat, waxy, poorly demarcated plaque with prominent telangiectasia.
This basal cell carcinoma appears as a flat, waxy, poorly demarcated plaque with prominent telangiectasia.
© Springer Science+Business Media

Pigmented basal cell carcinoma is a less common variant. These lesions are sometimes misdiagnosed as pigmented nevi or malignant melanomas.
Pigmented basal cell carcinoma is a less common variant. These lesions are sometimes misdiagnosed as pigmented nevi or
© Springer Science+Business Media


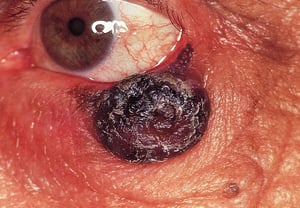
This photo shows an advanced pigmented basal cell carcinoma with ulceration on the cheek of a patient.
This photo shows an advanced pigmented basal cell carcinoma with ulceration on the cheek of a patient.
BSIP, GIRAND / SCIENCE PHOTO LIBRARY
This photo shows a superficial, slowly growing, ulcerated nodule.
This photo shows a superficial, slowly growing, ulcerated nodule.
Photo provided by Thomas Habif, MD.
This lesion usually appears as a firm, pearly, dome-shaped nodule often displaying multiple telangiectatic vessels coursing over its borders.
This lesion usually appears as a firm, pearly, dome-shaped nodule often displaying multiple telangiectatic vessels cour
© Springer Science+Business Media
This photo shows a superficial basal cell carcinoma on the forehead of a patient. This lesion involves only the epidermis.
This photo shows a superficial basal cell carcinoma on the forehead of a patient. This lesion involves only the epiderm
RICHARD USATINE MD / SCIENCE PHOTO LIBRARY
This basal cell carcinoma appears as a flat, waxy, poorly demarcated plaque with prominent telangiectasia.
This basal cell carcinoma appears as a flat, waxy, poorly demarcated plaque with prominent telangiectasia.
© Springer Science+Business Media
Pigmented basal cell carcinoma is a less common variant. These lesions are sometimes misdiagnosed as pigmented nevi or malignant melanomas.
Pigmented basal cell carcinoma is a less common variant. These lesions are sometimes misdiagnosed as pigmented nevi or
© Springer Science+Business Media
This photo shows an advanced pigmented basal cell carcinoma with ulceration on the cheek of a patient.
This photo shows an advanced pigmented basal cell carcinoma with ulceration on the cheek of a patient.
BSIP, GIRAND / SCIENCE PHOTO LIBRARY
Symptoms and signs references
1. Rubin AI, Chen EH, Ratner D. Basal-cell carcinoma. N Engl J Med. 2005 Nov 24;353(21):2262-9. doi: 10.1056/NEJMra044151. PMID: 16306523.
2. Pampena R, Parisi G, Benati M, et al. Clinical and Dermoscopic Factors for the Identification of Aggressive Histologic Subtypes of Basal Cell Carcinoma. Front Oncol. 2021;10:630458. Published 2021 Feb 19. doi:10.3389/fonc.2020.630458
Diagnosis of Basal Cell Carcinoma
Biopsy and histopathological examination
The diagnosis of basal cell carcinoma consists of clinical evaluation of a suspicious skin lesion followed by confirmation with biopsy and histologic examination. Histopathological examination confirms the subtype of basal cell carcinoma, which is important for guiding treatment.
Treatment of Basal Cell Carcinoma
Usually with local therapies
Treatment of basal cell carcinoma should be performed by a specialist.
The clinical appearance, size, site, and histologic subtype determine choice of treatment. Treatment selection depends on risk stratification (1).
Low-risk tumors are managed with:
Primarily surgical excision, curettage, or electrodesiccation
Nonsurgical modalities (eg, topical chemotherapy [imiquimod or 5-fluorouracil], cryotherapy, photodynamic therapy)
Occasionally radiation therapy
Low-risk features include:
Location on the trunk or extremities with a diameter < 2 cm
Well-defined clinical borders
Primary (not recurrent) tumors
Nodular or superficial subtypes
Absence of perineural involvement
Recurrence rates are generally higher when nonsurgical approaches are used (with the exception of radiation therapy) (2), but cosmetic outcomes may be superior (3).
High-risk tumors usually require one of the following:
Mohs micrographic surgery
Surgical excision with peripheral and deep en face margin assessment techniques, for which tissue borders are progressively excised until specimens are tumor-free,as determined by microscopic examination during surgery
High-risk features include:
Tumors of any size on the head, neck, hands, feet, pretibial, or anogenital areas
Diameter ≥ 2 cm on trunk and extremities
Poorly-defined borders
Recurrent tumors
Aggressive growth patterns (basosquamous, infiltrative, morpheaform)
Perineural involvement
Immunosuppression
Prior radiation therapy site
If patients have metastatic or locally advanced disease and are not candidates for surgery or radiation therapy (eg, because lesions are large, recurrent, or metastatic), vismodegib or sonidegib may be given (4, 5). Both medications inhibit the Hedgehog pathway. Cemiplimab, a programmed death-receptor 1 (PD-1) inhibitor, is an option for patients who cannot tolerate Hedgehog pathway inhibitors (6).
Treatment references
1. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines). Basal Cell Skin Cancer, version 1.2026. https://www.nccn.org/professionals/physician_gls/pdf/nmsc.pdf. Accessed November 13, 2025.
2. Drucker AM, Adam GP, Rofeberg V, et al. Treatments of Primary Basal Cell Carcinoma of the Skin: A Systematic Review and Network Meta-analysis. Ann Intern Med. 2018 Oct 2;169(7):456-466. doi: 10.7326/M18-0678. Epub 2018 Sep 18. PMID: 30242379.
3. Thomson J, Hogan S, Leonardi-Bee J, et al. Interventions for basal cell carcinoma of the skin. Cochrane Database Syst Rev. 2020;11(11):CD003412. Published 2020 Nov 17. doi:10.1002/14651858.CD003412.pub3
4. Basset-Séguin N, Hauschild A, Kunstfeld R, et al. Vismodegib in patients with advanced basal cell carcinoma: Primary analysis of STEVIE, an international, open-label trial. Eur J Cancer 86:334-348, 2017. doi: 10.1016/j.ejca.2017.08.022
5. Lear JT, Migden MR, Lewis KD, et al. Long-term efficacy and safety of sonidegib in patients with locally advanced and metastatic basal cell carcinoma: 30-month analysis of the randomized phase 2 BOLT study. J Eur Acad Dermatol Venereol 32(3):372-381, 2018. doi: 10.1111/jdv.14542
6. Stratigos AJ, Sekulic A, Peris K, et al. Cemiplimab in locally advanced basal cell carcinoma after hedgehog inhibitor therapy: An open-label, multi-centre, single-arm, phase 2 trial. Lancet Oncol 22(6):848–857, 2021. doi: 10.1016/S1470-2045(21)00126-1
Prognosis for Basal Cell Carcinoma
Basal cell carcinoma generally has an excellent prognosis because of the extremely low metastatic potential and high cure rates following appropriate treatment (1). While basal cell carcinomas rarely metastasize, they may invade healthy tissues (ie, local spread). Rarely, patients die because the carcinoma invades or impinges on underlying vital structures or orifices (eg, eyes, ears, mouth, bone, dura mater).
Approximately 40% of patients with a history of keratinocyte cancer will develop another keratinocyte cancer within 5 years of the original carcinoma (2). Risks of recurrence are progressively higher for each recurrence (ie, for third compared to second, and fourth compared to third). Consequently, long-term surveillance is recommended; patients with a history of basal cell carcinoma should be seen annually for a skin examination.
Prognosis references
1. Correia de Sá TR, Silva R, Lopes JM. Basal cell carcinoma of the skin (part 2): diagnosis, prognosis and management. Future Oncol. 2015 Nov;11(22):3023-38. doi: 10.2217/fon.15.245. Epub 2015 Oct 9. PMID: 26449265.
2. Wehner MR, Linos E, Parvataneni R, et al. Timing of subsequent new tumors in patients who present with basal cell carcinoma or cutaneous squamous cell carcinoma. JAMA Dermatol. 2015 Apr;151(4):382-8. doi: 10.1001/jamadermatol.2014.3307. PMID: 25588079.
Prevention of Basal Cell Carcinoma
Because basal cell carcinoma is associated with ultraviolet (UV) radiation exposure, a number of measures (eg, sun avoidance measures, use of protective clothing, use of sunscreen) are recommended to limit exposure. For more detailed information, see Prevention of Effects of Sun Exposure.
Key Points
Basal cell carcinomas, the most common skin cancers, are particularly common on sun-exposed skin among people with light skin.
The diagnosis should be considered with typical lesions (eg, shiny, slowly enlarging papule, often with a shiny, pearly border) and lesions that bleed easily or alternately crust and heal.
Patients should be referred to specialists for treatment, which is usually performed by locally destructive methods.
Drug Information for the Topic





