





Secretory otitis media is an accumulation of fluid in the middle ear.
Secretory otitis media occurs when acute otitis media has not completely resolved or allergies cause blockage of the eustachian tube.
People may have fullness and some temporary hearing loss in the affected ear.
Doctors examine the ear and use tympanometry to diagnose this disorder.
Doctors may need to make an opening in the eardrum to let fluid drain.

Serous otitis media can develop from acute otitis media that has not completely cleared or from a blocked eustachian tube (which connects the middle ear and the back of the nose). Allergies and enlarged adenoids are common causes of eustachian tube blockage. Tumors are rare causes of blockage. Serous otitis media can occur at any age, but it commonly develops after acute otitis media in children (see Secretory Otitis Media in Children) and may persist for weeks to months.
Normally, pressure in the middle ear is equalized 3 or 4 times a minute as the eustachian tube opens during swallowing. If the eustachian tube is blocked, pressure in the middle ear tends to decrease as oxygen is absorbed into the bloodstream from the middle ear. As the pressure decreases, fluid may accumulate in the middle ear, reducing the eardrum’s ability to move.
Symptoms of Serous Otitis Media

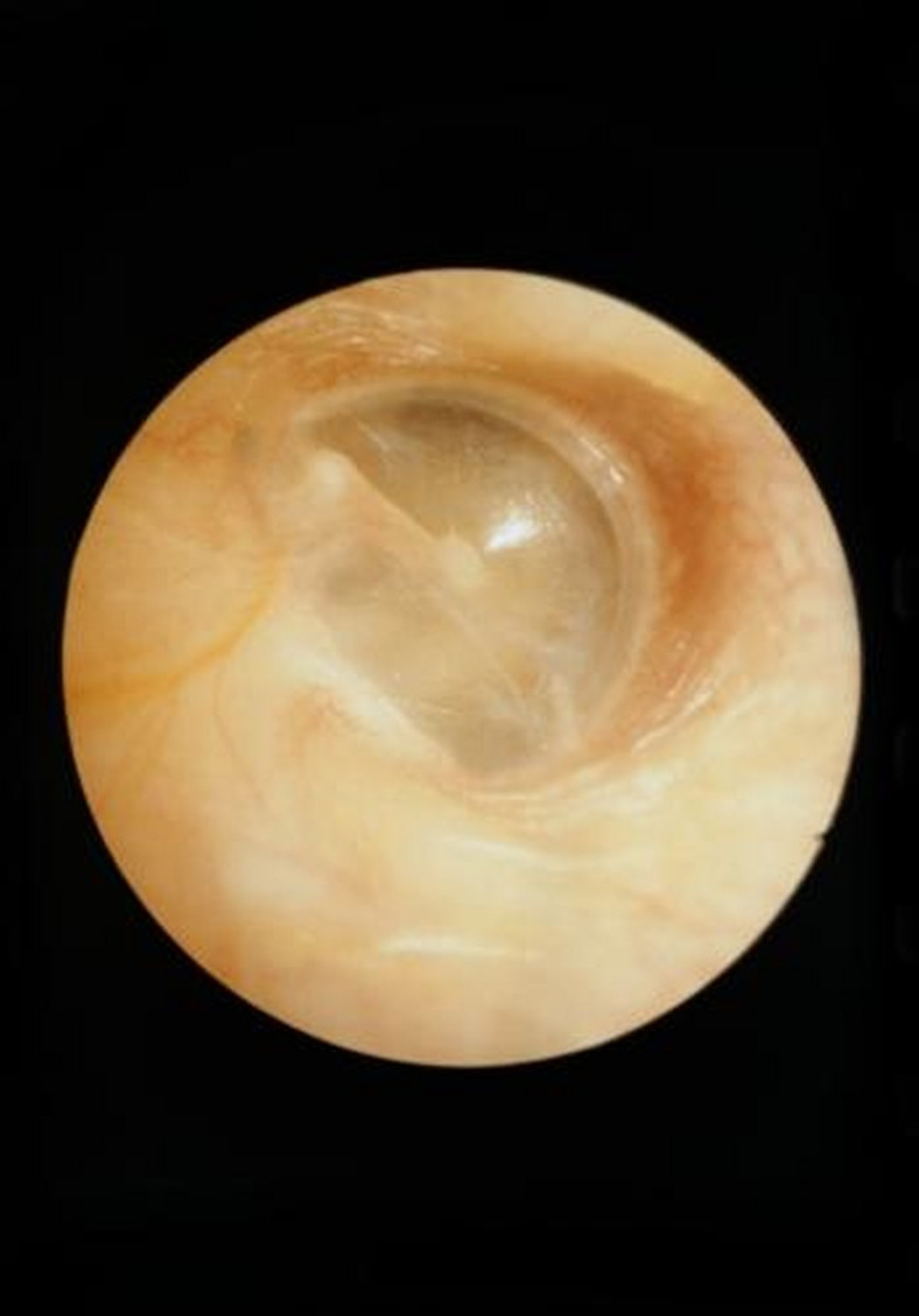
This image shows a normal eardrum (tympanic membrane).
CLINICA CLAROS/SCIENCE PHOTO LIBRARY


Some people with secretory otitis media have bubbles and white, chalky areas on the tympanic membrane.
TONY WRIGHT, INSTITUTE OF LARYNGOLOGY AND OTOLOGY/SCIENCE PHOTO LIBRARY
Usually, the fluid in the middle ear contains some bacteria, but symptoms of an active infection (such as redness, pain, and pus) are rare. Earache is rare. People usually notice a fullness in the affected ear and may hear a popping or crackling sound when they swallow. Some hearing loss commonly develops.
Diagnosis of Serous Otitis Media
A doctor's evaluation
A doctor examines the ear to make the diagnosis. Doctors use an otoscope (a handheld light) with a device uses air to move the eardrum. If there is fluid in the middle ear or a hole in the eardrum, the eardrum does not move normally.


This photo shows an adolescent undergoing tympanometry. This examination is done to help determine whether there is fluid in the middle ear.
ANNABELLA BLUESKY/SCIENCE PHOTO LIBRARY
Tympanometry helps determine whether fluid is in the middle ear. Doctors examine the nasal passages and upper throat in adults and adolescents to check for tumors.
Treatment of Serous Otitis Media
Watchful waiting
Maneuvers to increase pressure in the ear
Sometimes drainage tubes in the ear
Most people with secretory otitis media get better without treatment. Decongestants and antibiotics are not helpful.
People with congestion caused by allergies may be given antihistamines by mouth and/or a steroid (sometimes also called a glucocorticoid or corticosteroid) nasal spray.
Low pressure in the middle ear can be temporarily increased by forcing air past the blockage in the eustachian tube. The following methods may used:
People are instructed to try to breathe out and keep their mouth closed and their nostrils pinched shut (called the Valsalva maneuver).
People are instructed to gently pinch their nose and swallow. This maneuver can be repeated several times throughout the day to get air into the middle ear.
The doctor can use a special syringe (middle ear inflator) to blow air into one of the person’s nostrils, then blocks the other nostril while the person swallows. This technique (called politzerization) forces the air into the eustachian tube and middle ear.
If symptoms become chronic (lasting more than 1 to 3 months), a doctor may perform a myringotomy. For this procedure, an opening is made through the eardrum to allow fluid to drain from the middle ear. A tiny drainage tube (tympanostomy tube—see figure ) can be inserted into the opening in the eardrum to help fluid drain and allow air to enter the middle ear. Children may also need to have their adenoids removed (adenoidectomy). Young children with prolonged hearing loss from long-standing secretory otitis media may require appropriate treatment to make sure their language skills develop normally.
Myringotomy: Treating Secretory Otitis Media
During a myringotomy, doctors make a small opening in the eardrum to allow fluid to drain from the middle ear. Then they place a tiny, hollow plastic or metal tube (tympanostomy tube, or ventilating tube) in the eardrum through the opening. These tubes balance the pressure in the environment with that in the middle ear. Doctors recommend ventilating tubes for some children who have had recurring ear infections or recurring or persistent collections of fluid in their middle ears (chronic serous otitis media). Placement of ventilating tubes is a common surgical procedure that is done in a hospital or doctor’s office. General anesthesia or sedation is usually required. After the procedure, children usually go home within a few hours. Antibiotic ear drops are sometimes given after the procedure for about a week. The tubes usually come out on their own after about 6 to 12 months, but some types stay in longer. Tubes that do not come out on their own are removed by the doctor, sometimes under general anesthesia or sedation. If the opening does not close on its own, it may need to be closed surgically. Children with ventilating tubes may wash their hair and go swimming, but some doctors recommend children do not submerge their head in deep water without using earplugs. Drainage of fluid from the ears indicates an infection, and the doctor should be notified. |

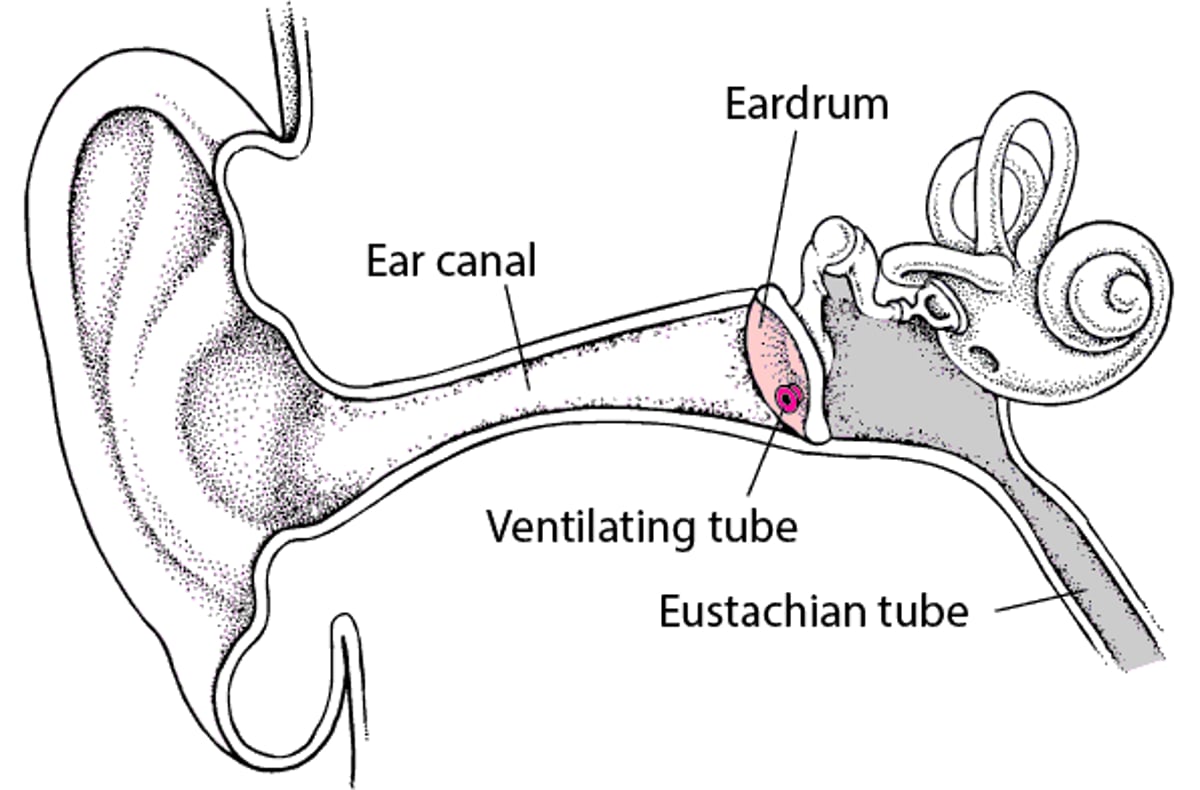


This illustration shows a tympanostomy tube, also called a ventilating tube, inserted in the eardrum (tympanic membrane) during a myringotomy. The eardrum is a grayish color, and the tympanostomy tube is green for visual emphasis.
Image Copyright © Nucleus Medical Media. All rights reserved.
People with allergies should try to eliminate known allergens from their environment. Doctors may recommend allergen immunotherapy, which tries to teach the person's immune system not to react to an allergen.
People with secretory otitis media should avoid or delay scuba diving and air travel because changes in environmental pressure can cause ear pain and injury (barotrauma). If air travel cannot be avoided, chewing food or drinking (for example, from a bottle) may help young children with this disorder. In older children and adults, often the pressure in the middle ear can be equalized and the discomfort can be relieved by several maneuvers. If outside pressure is decreasing, as in a plane ascending, the person should try breathing with the mouth open, yawning, chewing gum, or swallowing. If outside pressure is increasing, as in a plane descending or a diver going deeper underwater, the person should pinch the nose shut, hold the mouth closed, and try to blow gently out through the nose (called the Valsalva maneuver). This maneuver forces air through the blocked eustachian tube.





