



The tonsils and adenoids may enlarge (become bigger) because of an infection or other cause or may be large at birth. Enlargement of the tonsils and adenoids is common among children and typically does not need any treatment.
Enlarged tonsils and adenoids in children may result from infections but may be normal.
Enlargement usually causes no symptoms but can occasionally cause difficulty breathing or swallowing and sometimes recurring ear or sinus infections or obstructive sleep apnea.
The diagnosis is based on a physical examination to see the tonsils, nasopharyngoscopy to see the adenoids, and sometimes on the results of a sleep study to see whether enlarged tonsils and adenoids may be causing obstructive sleep apnea.
Antibiotics may be used if a bacterial infection is present, and sometimes, if infections are recurring, the tonsils and adenoids are removed.
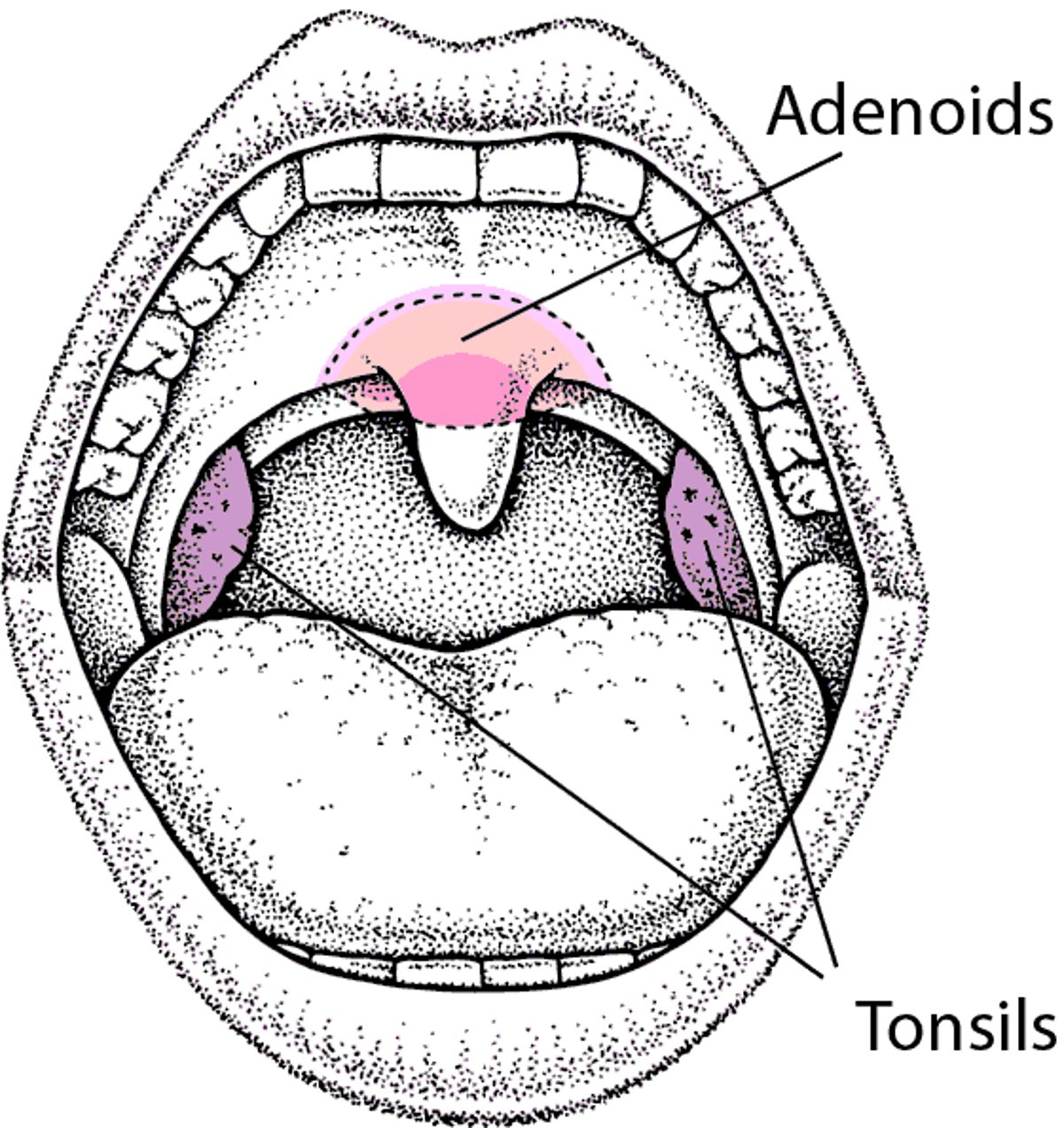
Locating the Tonsils and Adenoids
The tonsils are 2 areas of lymphoid tissue located on either side of the throat. The adenoids, also lymphoid tissue, are located higher and further back, behind the palate, where the nasal passages connect with the throat. The adenoids are not visible through the mouth. |

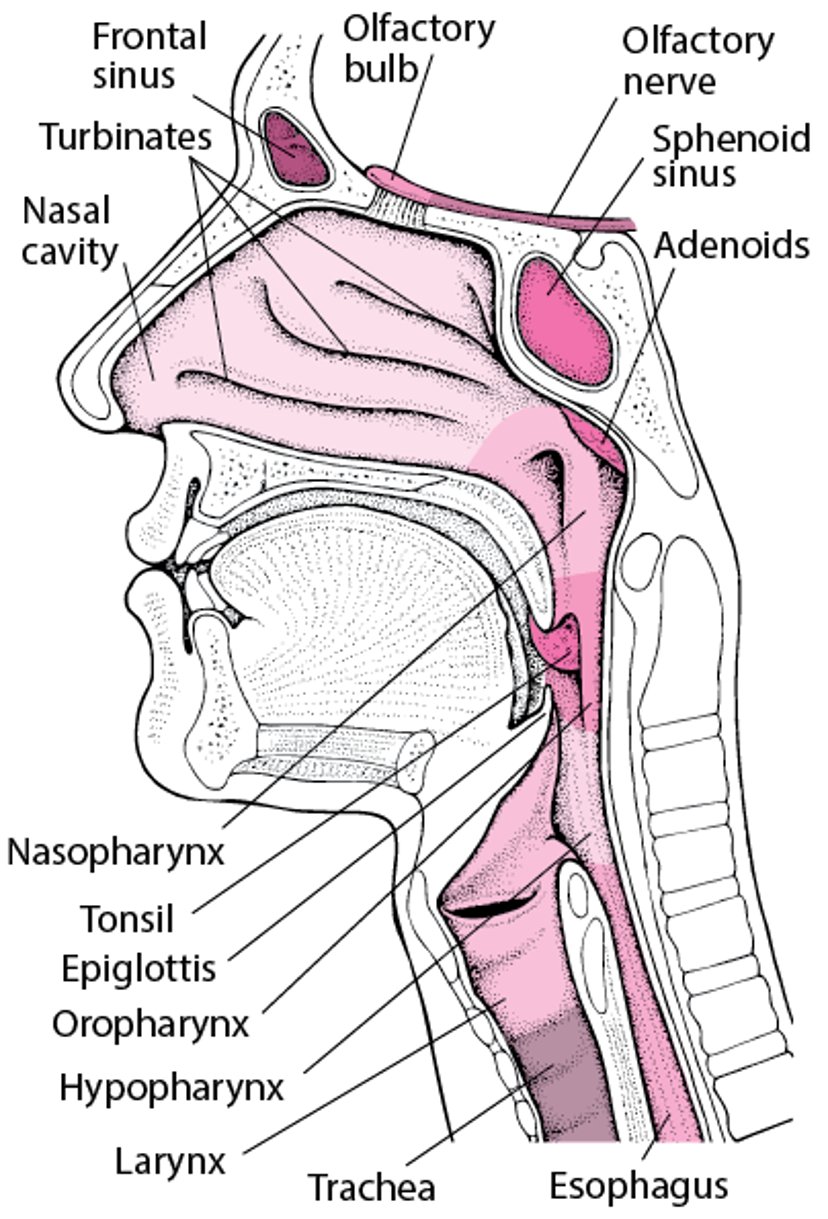
A Look Inside the Throat

Tonsils and adenoids are collections of lymphoid tissue that may have a role in helping the body fight infection. They trap bacteria and viruses entering through the throat and produce antibodies. The tonsils and adenoids are largest in children who are 2 to 6 years of age.
The tonsils are located on both sides of the back of the throat. The adenoids are located higher and further back, where the nasal passages connect with the throat. The tonsils are visible through the mouth, but the adenoids are not.
Causes of Enlarged Tonsils and Adenoids
Some preschool and adolescent children have relatively large tonsils and adenoids that are not due to any problem. However, tonsils and adenoids can become enlarged because they become infected with a virus or bacteria that cause throat infections (sore throat). In addition, allergies (such as seasonal allergies or year-round allergies), irritants, and, possibly, gastroesophageal reflux also can cause the tonsils and adenoids to enlarge. Ongoing exposure to children who have bacterial or viral infections, such as children at child care centers, increases the risk of infection.
When enlarged, tonsils sometimes interfere with breathing or swallowing, and adenoids may block the nose or the eustachian tubes that connect the back of the throat to the ears. Usually, tonsils and adenoids return to normal size once the infection is over. Sometimes they remain enlarged, particularly in children who have had frequent or chronic infections.
Symptoms of Enlarged Tonsils and Adenoids
Most enlarged tonsils and adenoids cause no symptoms. However, enlarged tonsils or adenoids can give the voice a stuffy-nose quality (children sound as though they have a cold). Children with enlarged tonsils or adenoids may have an abnormally shaped palate and position of the teeth. Children may also tend to breathe through their mouth. Enlarged tonsils can also cause nosebleeds, bad breath, and cough.
Complications
Enlarged tonsils and adenoids are considered a problem when they cause more serious problems such as the following:
Chronic ear infections and hearing loss: These problems result from blockage of the eustachian tube and fluid accumulation in the middle ear.
Recurring sinus infections: See Sinusitis.
Obstructive sleep apnea: Some children with enlarged tonsils and adenoids snore and stop breathing for brief periods during sleep. As a result, oxygen levels in the blood may be low, and children may wake up frequently and be sleepy during the day. Rarely, obstructive sleep apnea caused by enlarged tonsils and adenoids has serious complications, such as high blood pressure in the lungs (pulmonary hypertension) and changes in the heart due to pulmonary hypertension (cor pulmonale).
Weight loss or lack of weight gain: Children may not eat sufficiently because of pain resulting from infections or because breathing takes constant physical effort.
Diagnosis of Enlarged Tonsils and Adenoids
Nasopharyngoscopy
Sometimes a sleep study
Very large tonsils may be normal, and chronically infected tonsils may be normal-sized. To help determine whether infections are the cause of enlarged tonsils, doctors ask how many episodes of strep throat children have had during the past 1 to 3 years.
Usually, to view the back of the nose and throat, doctors insert a flexible viewing tube through the nose (called a nasopharyngoscope). Doctors also look for redness of the tonsils, enlargement of lymph nodes at the jaw and in the neck, and the effect of the tonsils on breathing. They may also take x-rays of the neck to determine the size of the adenoids.
Obstructive sleep apnea is suspected when parents report that the child stops breathing during sleep. In such cases, doctors may recommend the child undergo a sleep study (polysomnography). For this test, the child is monitored while sleeping overnight in a sleep laboratory. Doctors also may take a chest x-ray and measure oxygen levels in the blood.
Treatment of Enlarged Tonsils and Adenoids
Treatment of other causes (allergies and infections)
Sometimes adenoidectomy, tonsillectomy, or both
If doctors think the cause is allergies, they may give a nasal corticosteroid spray or other medications, such as antihistamines, by mouth. If the cause appears to be a bacterial infection, doctors may give antibiotics.
If these medications are not effective or if doctors think they will not be useful, doctors may recommend surgical removal of the adenoids (called adenoidectomy) and possibly removal of the tonsils (called tonsillectomy) during the same operation.
Tonsillectomy and adenoidectomy are very common operations for children in the United States. Children who benefit from these operations include those who have the following:
Obstructive sleep apnea
Extreme discomfort when talking and breathing
Multiple throat infections (defined by some doctors as more than six infections in 1 year, more than four infections a year for 2 years, or more than two infections a year for 3 years)
Doctors may recommend only adenoidectomy for children who have the following:
Frequent ear infections and persistent collections of fluid in the middle ears
Recurring nosebleeds or nasal blockages causing voice changes or disturbed sleep
Frequent sinus infections
Obstructive sleep apnea that is caused by large adenoids in a child who does not also need a tonsillectomy
Did You Know...
|
Tonsillectomy and adenoidectomy do not seem to decrease the frequency or severity of colds or cough.
Tonsillectomy and adenoidectomy are often done on an outpatient basis. These operations should be done at least 2 weeks after any infection has cleared.
The surgical complication rate is low, but postoperative pain and difficulty swallowing caused by tonsillectomy may last up to 2 weeks. Children typically recover from adenoidectomy in 2 to 3 days.
Bleeding resulting from tonsillectomy is a less common complication but may occur at 2 peak times: within 24 hours after surgery or at about 7 days after surgery. Bleeding after surgery very rarely may be serious or even life-threatening in children. Children who have bleeding after surgery should receive emergency care.





