

Nerve root disorders result in segmental radicular deficits (eg, pain or paresthesias in a dermatomal distribution, weakness of muscles innervated by the root). Diagnosis may require neuroimaging, electrodiagnostic testing, and systemic testing for underlying disorders. Treatment depends on the cause but may include symptomatic relief with nonsteroidal anti-inflammatory drugs, other analgesics, and corticosteroids.
(See also Overview of Peripheral Nervous System Disorders.)
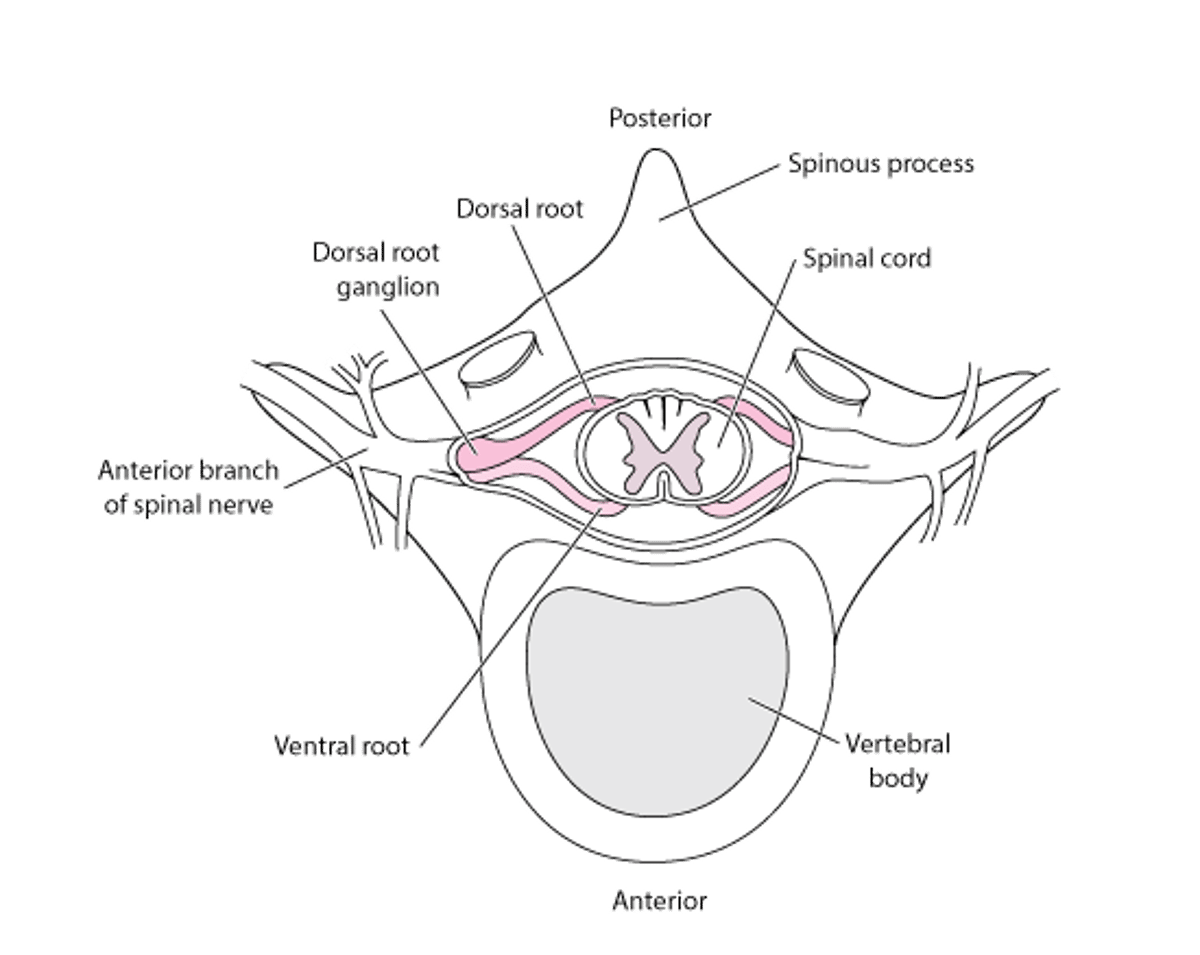
Nerve root disorders (radiculopathies) are precipitated by acute or chronic pressure on a nerve root in adjacent to the spinal column (see figure ).
Spinal Nerve Roots

Etiology of Nerve Root Disorders
The most common cause of radiculopathies is
Bone changes due to rheumatoid arthritis (RA) or osteoarthritis, especially in the cervical and lumbar areas, may also compress isolated nerve roots.
Less commonly, carcinomatous meningitis causes patchy multiple root dysfunction. Rarely, spinal mass lesions (eg, epidural abscesses and tumors, spinal meningiomas, neurofibromas) may manifest with radicular symptoms instead of the usual symptoms of spinal cord dysfunction.
Diabetes can cause a painful thoracic or extremity radiculopathy by causing ischemia of the nerve root.
Infectious disorders, such as those due to mycobacteria (eg, tuberculosis [TB]), fungi (eg, histoplasmosis), or spirochetes (eg, Lyme disease, syphilis), sometimes affect nerve roots. Herpes zoster infection usually causes a painful radiculopathy with dermatomal sensory loss and characteristic rash, but it may cause a motor radiculopathy with segmental weakness and reflex loss. Cytomegalovirus-induced polyradiculitis is a complication of AIDS.
Symptoms and Signs of Nerve Root Disorders
Radiculopathies tend to cause characteristic radicular syndromes of pain and segmental neurologic deficits based on the cord level of the affected root (see table ). Muscles innervated by the affected motor root become weak and atrophy; they also may be flaccid with fasciculations. Sensory root involvement causes sensory impairment in a dermatomal distribution. Corresponding segmental deep tendon reflexes may be diminished or absent. Electric shock–like pains may radiate along the affected nerve root’s distribution.
Symptoms of Common Radiculopathies by Cord Level
Level | Symptoms |
|---|---|
C4 | Pain in the lower neck and trapezius area with paresthesias involving the lower neck and upper shoulder girdle |
C5 | Pain in the neck, shoulder, and dorsal forearm with paresthesias and numbness involving the dorsal arm Weakness of the deltoid, biceps, and rotator cuff Decrease in the biceps brachii reflex |
C6 | Pain in the trapezius ridge and tip of the shoulder, often radiating to the thumb, with paresthesias and sensory impairment in the same areas Weakness of biceps Decreased biceps brachii and brachioradialis reflexes |
C7 | Pain, paresthesias, and numbness in the shoulder blade and axilla, radiating to the middle finger Weakness of triceps Decreased triceps brachii reflex |
T (any) | Bandlike dysesthesias around the thorax (eg, T4 nipple, T10 umbilicus) |
L3 | Pain, numbness, and paresthesias in the anterior and medial thigh and knee with quadriceps weakness and diminished patellar reflex |
L4 | Pain, numbness, and paresthesias in the medial lower leg and ankle Weakness of the quadriceps, ankle dorsiflexion, and diminished patellar reflex |
L5 | Pain in the buttock, posterior lateral thigh, calf, and foot Footdrop with weakness of the anterior tibial, posterior tibial, and peroneal muscles Sensory loss over the anterolateral lower leg and dorsum of the foot |
S1 | Pain along the posterior aspect of the leg and buttock Weakness of the medial gastrocnemius muscle with impaired ankle plantar flexion Loss of ankle jerk Sensory loss over the lateral calf and foot |
Pain may be exacerbated by movements that transmit pressure to the nerve root through the subarachnoid space (eg, moving the spine, coughing, sneezing, doing the Valsalva maneuver).


Copyright © 2025 Merck & Co., Inc., Rahway, NJ, USA and its affiliates. All rights reserved.
Lesions of the cauda equina, which affect multiple lumbar and sacral roots (cauda equina syndrome), cause radicular symptoms in both legs and may impair sphincter and sexual function.
Findings indicating spinal cord compression include the following:
A sensory level (an abrupt change in sensation below a horizontal line across the spine)
Flaccid paraparesis or quadriparesis
Reflex abnormalities below the site of compression
Early-onset hyporeflexia followed later by hyperreflexia
Sphincter dysfunction
Diagnosis of Nerve Root Disorders
Neuroimaging
Sometimes electrodiagnostic tests
Radicular symptoms require MRI or CT of the affected area. Myelography is needed only if MRI is contraindicated (eg, because of an implanted pacemaker or presence of other metal) and CT is inconclusive. The area imaged depends on symptoms and signs; if the level is unclear, electrodiagnostic tests should be done to localize the affected root, but they cannot identify the cause.
If imaging does not detect an anatomic abnormality, cerebrospinal fluid analysis is done to check for infectious or inflammatory causes, and fasting plasma glucose is measured to check for diabetes.
Treatment of Nerve Root Disorders
Treatment of the cause and of pain
Surgery (as a last resort)
Specific causes of nerve root disorders are treated.
Acute pain requires appropriate analgesics (eg, acetaminophen, nonsteroidal anti-inflammatory drugs [NSAIDs], sometimes opioids). NSAIDs are particularly useful for disorders that involve inflammation. Muscle relaxants, sedatives, and topical treatments rarely provide additional benefit. If symptoms are not relieved with nonopioid analgesics, corticosteroids can be given systemically or as an epidural injection; however, analgesia tends to be modest and temporary. Methylprednisolone may be given, tapered over 6 days, starting with 24 mg orally once a day and decreased by 4 mg a day.requires appropriate analgesics (eg, acetaminophen, nonsteroidal anti-inflammatory drugs [NSAIDs], sometimes opioids). NSAIDs are particularly useful for disorders that involve inflammation. Muscle relaxants, sedatives, and topical treatments rarely provide additional benefit. If symptoms are not relieved with nonopioid analgesics, corticosteroids can be given systemically or as an epidural injection; however, analgesia tends to be modest and temporary. Methylprednisolone may be given, tapered over 6 days, starting with 24 mg orally once a day and decreased by 4 mg a day.
Management of chronic pain can be difficult; acetaminophen and NSAIDs are often only partly effective, and long-term use of NSAIDs has substantial risks. Opioids have a risk of addiction. Tricyclic antidepressants and antiseizure medications may be effective, as may physical therapy and consultation with a mental health professional. For a few patients, alternative medical treatments (eg, can be difficult; acetaminophen and NSAIDs are often only partly effective, and long-term use of NSAIDs has substantial risks. Opioids have a risk of addiction. Tricyclic antidepressants and antiseizure medications may be effective, as may physical therapy and consultation with a mental health professional. For a few patients, alternative medical treatments (eg,transdermal electrical nerve stimulation, spinal manipulation, acupuncture, medicinal herbs) may be tried if all other treatments are ineffective.
If the pain is intractable or if progressive weakness or sphincteric dysfunction suggest spinal compression, surgical decompression may be necessary.
Key Points
Suspect a nerve root disorder in patients who have segmental deficits such as sensory abnormalities in a dermatomal distribution (eg, pain, paresthesias) and/or motor abnormalities (eg, weakness, atrophy, fasciculations, hyporeflexia) at a nerve root level.
If patients have a sensory level, bilateral flaccid weakness, and/or sphincter dysfunction, suspect spinal cord compression.
If clinical findings suggest radiculopathy, do MRI or CT.
Use analgesics and sometimes corticosteroids for acute pain, and consider other medications and other treatments, as well as analgesics, for chronic pain.
In patients with progressive weakness and sphincteric dysfunction, consider surgical decompression.





