

Calcium pyrophosphate deposition (CPPD) disease involves intra-articular and/or extra-articular deposition of calcium pyrophosphate (CPP) crystals. Manifestations are protean and may be minimal or include intermittent flares of acute arthritis, termed pseudogout or acute CPP crystal arthritis, and a degenerative arthropathy that is often severe. Diagnosis requires identification of CPP crystals in synovial fluid. Treatment of pseudogout flares is with intra-articular or oral glucocorticoids, nonsteroidal anti-inflammatory drugs (NSAIDs), or colchicine.Calcium pyrophosphate deposition (CPPD) disease involves intra-articular and/or extra-articular deposition of calcium pyrophosphate (CPP) crystals. Manifestations are protean and may be minimal or include intermittent flares of acute arthritis, termed pseudogout or acute CPP crystal arthritis, and a degenerative arthropathy that is often severe. Diagnosis requires identification of CPP crystals in synovial fluid. Treatment of pseudogout flares is with intra-articular or oral glucocorticoids, nonsteroidal anti-inflammatory drugs (NSAIDs), or colchicine.
CPP crystal deposition (chondrocalcinosis, pyrophosphate arthropathy), whether symptomatic or asymptomatic, becomes more common with age.
Asymptomatic chondrocalcinosis is common in the knee, metacarpophalangeal joints, hip, wrist, annulus fibrosus of the intervertebral disks, symphysis pubis, and spine. Men and women are affected approximately equally. The incidental detection of chondrocalcinosis on radiographs or other imaging in a patient who is asymptomatic is not an indication for treatment of CPP arthritis. CPP deposition may accelerate the progression of osteoarthritis (1).
Reference
1. Conway R, McCarthy GM. Calcium-Containing Crystals and Osteoarthritis: an Unhealthy Alliance. Curr Rheumatol Rep. 2018;20(3):13. Published 2018 Mar 8. doi:10.1007/s11926-018-0721-9
Etiology of Calcium Pyrophosphate Deposition Disease
The cause of most CPP crystal arthritis is unknown. CPP crystal arthritis is associated with other conditions, such as trauma (including surgery), hypomagnesemia, hyperparathyroidism, gout, hemochromatosis, hypophosphatasia, Gitelman syndrome, X-linked hypophosphatemic rickets, familial hypocalciuric hypercalcemia, and old age. These associations suggest that calcium pyrophosphate (CPP) crystal deposits may be caused by degenerative or metabolic changes in the affected tissues.
Some cases are familial, usually transmitted in an autosomal dominant pattern, with complete penetration by age 40.
The ankyrin (ANK) protein is a central factor in producing excess extracellular pyrophosphate, which promotes CPP crystal formation (1). ANK protein is a transporter of intracellular and microvesicle pyrophosphate to the extracellular location where CPP crystals form.
Etiology reference
1. Abhishek A, Doherty M. Pathophysiology of articular chondrocalcinosis--role of ANKH. Nat Rev Rheumatol. 2011;7(2):96-104. doi:10.1038/nrrheum.2010.182
Symptoms and Signs of Calcium Pyrophosphate Deposition Disease
Acute, subacute, or chronic arthritis can occur, usually in the knee, wrist, or other large peripheral joints; thus, CPP crystal arthritis can mimic many other forms of arthritis (1). Acute flares are similar to gout but vary more in intensity, tend to be more protracted, and are often more difficult to treat. There may be no symptoms of CPP crystal arthritis between flares or continuous low-grade symptoms in multiple joints, similar to rheumatoid arthritis or osteoarthritis. These patterns tend to persist for life.
Crowned dens syndrome (with a radiographically "crowned" appearance of the odontoid process of the second cervical vertebra) is a presentation of acute CPP axial arthritis in which there can be profound inflammatory neck pain and stiffness. It can be mistaken for polymyalgia rheumatica, giant cell arteritis, seronegative spondyloarthritis, cervical osteomyelitis, or meningitis.
Symptoms and signs reference
1. Pascart T, Filippou G, Lioté F, Sirotti S, Jauffret C, Abhishek A. Calcium pyrophosphate deposition disease. Lancet Rheumatol. 2024;6(11):e791-e804. doi:10.1016/S2665-9913(24)00122-X
Diagnosis of Calcium Pyrophosphate Deposition Disease
Synovial fluid analysis
Identification of crystals microscopically
CPP crystal arthritis should be suspected in older patients with arthritis, particularly those with a history of recurrent inflammatory arthritis.
Radiopaque deposits may sometimes be present in fibrocartilage, hyaline articular cartilage (particularly the knee), or both, but calcinosis can be seen in the absence of acute flares.

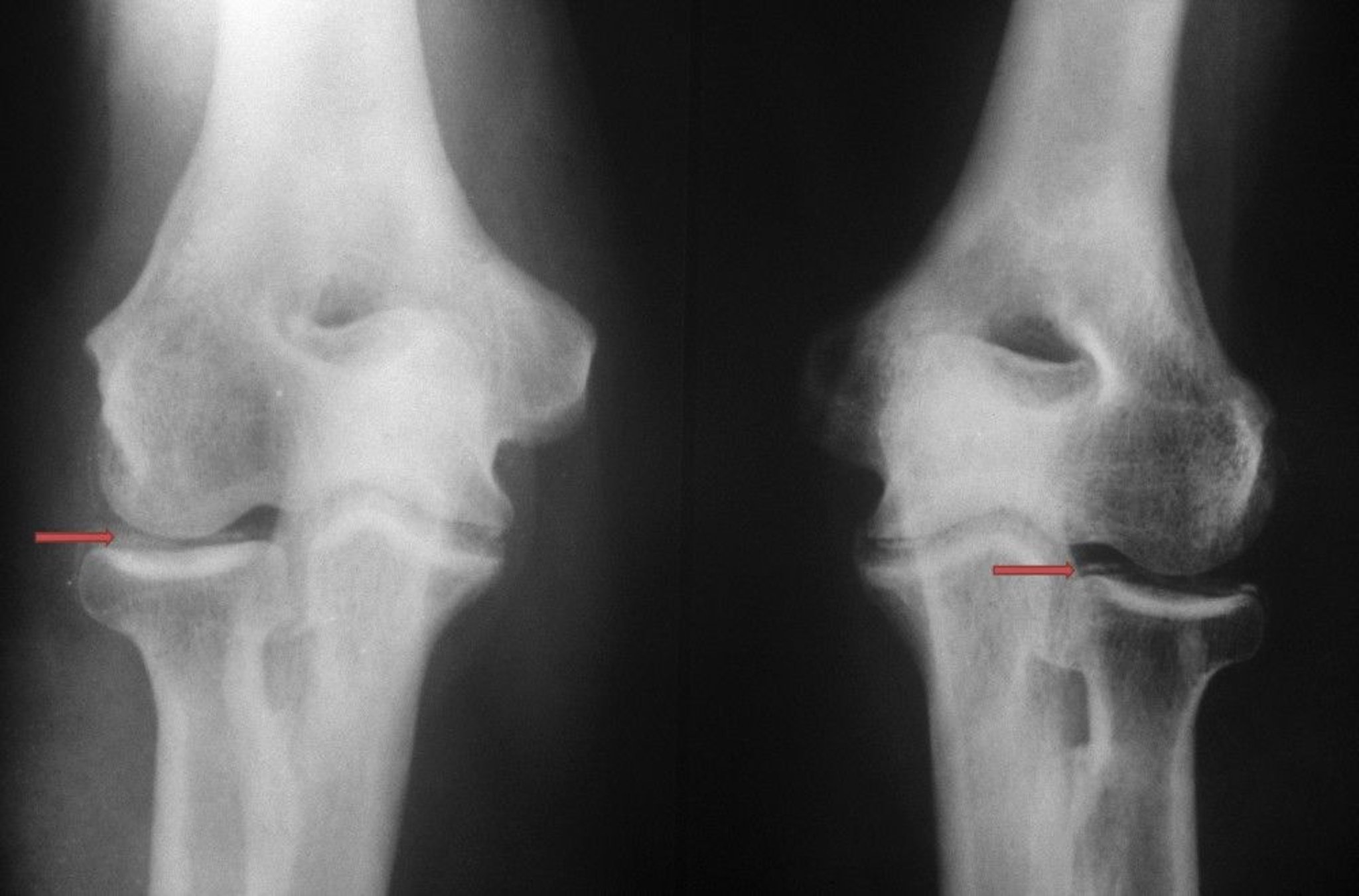
Calcium pyrophosphate crystal deposition is visible as poorly defined and variably dense radiopacities (red arrows) inside the elbow joint.
BIOPHOTO ASSOCIATES/SCIENCE PHOTO LIBRARY

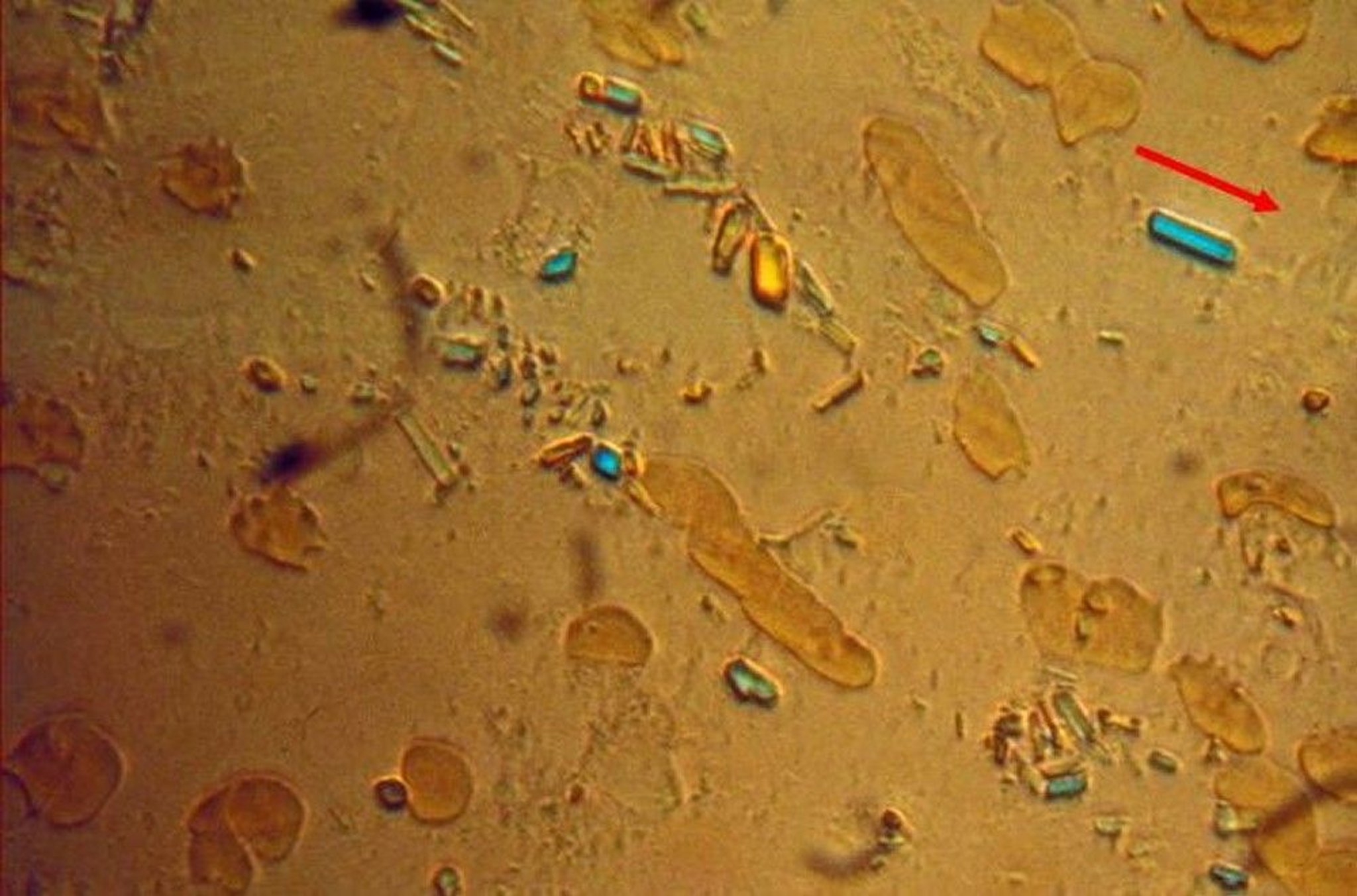
This image shows calcium pyrophosphate (CPP) crystals extracted from synovial fluid viewed under polarized light microscopy. (The red arrow in the upper right indicates the axis of a red compensator, a device used to determine the alignment of the crystals. The positively birefringent CPP crystals appear blue when parallel to the optical axis of the compensator and yellow when perpendicular to it.)
Image courtesy of Brian Mandell, MD.
Diagnosis of CPP crystal arthritis is established by identifying rhomboid- or rod-shaped crystals in synovial fluid that are not birefringent, or are weakly positively birefringent on polarized light microscopy. Joint fluid in acute flares has findings typical of inflammation; thus, coincident infectious arthritis and gout (other common causes of inflammatory joint fluid) must also be excluded. Infectious arthritis is excluded based on Gram stain and culture findings. Gout is best excluded by the absence of urate crystals in fluid from the inflamed joint. Notably a patient may have both gout and CPP arthritis. Radiographs or ultrasonography are indicated if synovial fluid cannot be obtained for analysis; findings of multiple linear or punctate calcification in articular cartilage, especially fibrocartilage, support the diagnosis, but do not exclude gout or infection.
Patients, especially younger ones, who have frequent CPP crystal flares should be evaluated for underlying triggers and diseases. Post-diagnostic laboratory testing that should be considered includes serum calcium, parathyroid hormone (PTH), serum magnesium, alkaline phosphatase, and iron studies (. Post-diagnostic laboratory testing that should be considered includes serum calcium, parathyroid hormone (PTH), serum magnesium, alkaline phosphatase, and iron studies (1).
Diagnosis reference
1. Parperis K, Constantinou A. Calcium Pyrophosphate Crystal Deposition: Insights to Risks Factors and Associated Conditions. Curr Rheumatol Rep. 2024;26(11):375-382. doi:10.1007/s11926-024-01158-5
Treatment of Calcium Pyrophosphate Deposition Disease
Intra-articular glucocorticoids
Oral glucocorticoids (eg, prednisone, methylprednisolone)Oral glucocorticoids (eg, prednisone, methylprednisolone)
Nonsteroidal anti-inflammatory drugs (NSAIDs)
Colchicine Colchicine
Interleukin-1 (IL-1) antagonists (eg, anakinra)Interleukin-1 (IL-1) antagonists (eg, anakinra)
Treatment of acute CPPD disease is similar to that for acute gout (1). Symptoms of acute synovial effusion abate with synovial fluid drainage and intra-articular glucocorticoid injection (eg, 40 mg prednisolone acetate or prednisolone tertiary butylacetate into a knee).). Symptoms of acute synovial effusion abate with synovial fluid drainage and intra-articular glucocorticoid injection (eg, 40 mg prednisolone acetate or prednisolone tertiary butylacetate into a knee).
Indomethacin, naproxen, or another Indomethacin, naproxen, or anotherNSAID given at anti-inflammatory doses often stops acute flares. Colchicine use for treatment of acute flares is identical to that of gout. Colchicine 0.6 mg orally once a day or 2 times a day may decrease the frequency of recurrent acute flares. Oral glucocorticoids are effective at treating acute CPP arthritis flares and are particularly useful for patients in whom oral NSAIDs and colchicine are contraindicated. However, failure to resolve an acute flare may require a higher dose for a longer period of time. Interleukin-1 antagonists such as anakinra can also be effective. is identical to that of gout. Colchicine 0.6 mg orally once a day or 2 times a day may decrease the frequency of recurrent acute flares. Oral glucocorticoids are effective at treating acute CPP arthritis flares and are particularly useful for patients in whom oral NSAIDs and colchicine are contraindicated. However, failure to resolve an acute flare may require a higher dose for a longer period of time. Interleukin-1 antagonists such as anakinra can also be effective.
Treatment reference
1. Stack J, McCarthy G. Calcium pyrophosphate deposition (CPPD) disease - Treatment options. Best Pract Res Clin Rheumatol. 2021;35(4):101720. doi:10.1016/j.berh.2021.101720
Prognosis for Calcium Pyrophosphate Deposition Disease
The prognosis for individual flares of acute CPPD disease is usually excellent. However, chronic arthritis can occur, and severe destructive arthropathy resembling neurogenic arthropathy (Charcot joints) occasionally occurs. Unlike gout, chronic CPP crystal arthritis is challenging to manage because there is no therapy that effectively eliminates or reduces the burden of CPP crystals.
Key Points
Asymptomatic chondrocalcinosis becomes more common with age, particularly in the knee, hip, wrist, annulus fibrosus of the intervertebral disks, and symphysis pubis but does not require treatment.
CPPD disease can affect the knee and large peripheral joints and mimic other forms of arthritis (eg, gout, rheumatoid arthritis, osteoarthritis).
Examine joint fluid for characteristic rhomboid- or rod-shaped crystals in synovial fluid that are not birefringent or are weakly positively birefringent, and exclude joint infection.
For acute symptoms, treat with an intra-articular glucocorticoid, an oral NSAID, colchicine, or oral glucocorticoids; anakinra can also be effective.For acute symptoms, treat with an intra-articular glucocorticoid, an oral NSAID, colchicine, or oral glucocorticoids; anakinra can also be effective.





