

Chalazia and hordeola (styes) are sudden-onset localized swellings of the eyelid. A chalazion is caused by noninfectious meibomian gland occlusion, whereas a hordeolum usually is caused by infection. Both conditions initially cause eyelid hyperemia and edema, swelling, and pain. With time, a chalazion becomes a small nontender nodule in the eyelid center, whereas a hordeolum remains painful and localizes to an eyelid margin. Diagnosis is clinical. Treatment is primarily with warm compresses. Both conditions improve spontaneously, but incision or, for chalazia, intralesional glucocorticoids may be used to hasten resolution.
Chalazion


In its initial stages, a chalazion is clinically indistinguishable from a hordeolum.
SCIENCE PHOTO LIBRARY
A chalazion is noninfectious obstruction of a meibomian gland causing extravasation of irritating lipid material in the eyelid soft tissues with focal secondary granulomatous inflammation (1). Disorders that cause abnormally thick meibomian gland secretions (eg, meibomian gland dysfunction, acne rosacea) increase the risk of meibomian gland obstruction.
Hordeolum
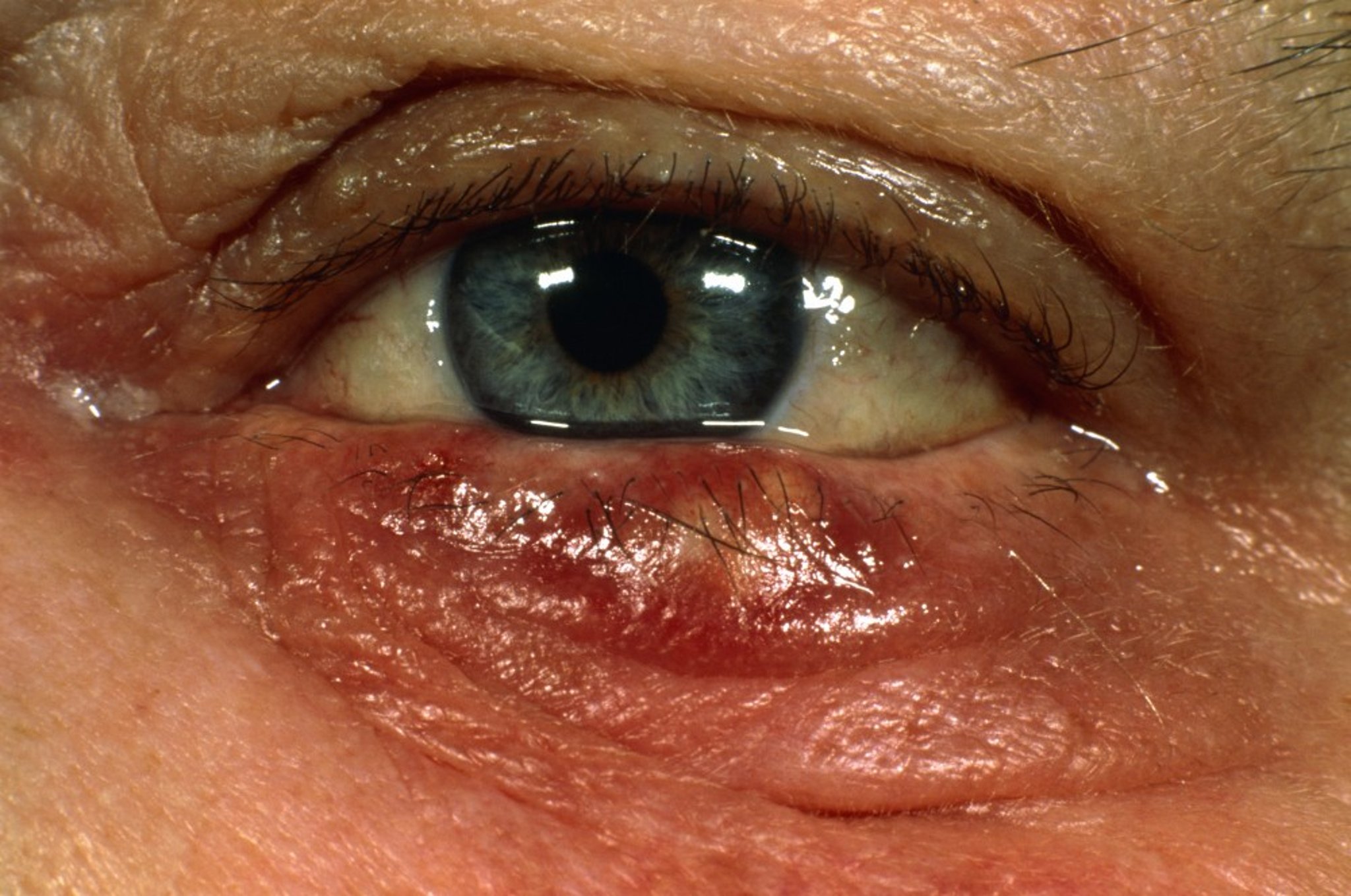
This hordeolum (stye) is swollen, red, and inflamed and is slightly yellow in the center.
DR. CHRIS HALE/SCIENCE PHOTO LIBRARY
A hordeolum (stye) is an acute, localized swelling of the eyelid that may be external or internal and usually is a pyogenic (typically staphylococcal) infection or abscess. Most hordeola are external and result from obstruction and infection of an eyelash follicle and adjacent glands of Zeis or Moll glands. Follicle obstruction may be associated with blepharitis. An internal hordeolum results from infection of a meibomian gland. Sometimes cellulitis accompanies hordeola.
General reference
1. Kim ES, Afshin EE, Elahi E. The lowly chalazion. Surv Ophthalmol. 2023 Jul-Aug;68(4):784-793. doi: 10.1016/j.survophthal.2022.11.002.
Symptoms and Signs of Chalazion and Hordeolum
Chalazia and hordeola each cause eyelid redness, swelling, and pain.
Chalazion
Initially the eyelid is diffusely swollen. Occasionally the eyelid can be massively swollen, shutting the eye completely. After 1 or 2 days, a chalazion localizes to the body of the eyelid. Typically, a small nontender nodule or lump develops. A chalazion usually drains through the inner surface of the eyelid or is absorbed spontaneously over 2 to 8 weeks; rarely, it persists longer. Depending on its size and location, a chalazion may indent the cornea, resulting in slightly blurred vision from induced astigmatism.
Hordeolum
After 1 to 2 days, an external hordeolum localizes to the eyelid margin. There may be tearing, photophobia, and a foreign body sensation. Typically, a small yellowish pustule develops at the base of an eyelash, surrounded by hyperemia, induration, and diffuse edema. Within 2 to 4 days, the lesion ruptures and discharges material (often pus), thereby relieving pain and resolving the lesion.
Symptoms of an internal hordeolum are the same as those of a chalazion, with pain, erythema, and edema localized to the posterior tarsal conjunctival surface. Inflammation may be severe, sometimes with fever or chills. Inspection of the tarsal conjunctiva shows a small elevation or yellow area at the site of the affected gland. Later, an abscess forms. Spontaneous rupture is rare; however, when it does occur, it usually occurs on the conjunctival side of the eyelid and sometimes erupts through the skin side. Recurrence is common.
Diagnosis of Chalazion and Hordeolum
History and physical examination alone
Diagnosis of chalazion and both kinds of hordeola is clinical; however, during the first 2 days, they may be clinically indistinguishable. Because internal hordeola are rarer, they are not usually suspected unless inflammation is severe or fever or chills are present. If the chalazion or hordeolum lies near the inner canthus of the lower eyelid, it must be differentiated from dacryocystitis and canaliculitis, which can usually be excluded by noting the location of maximum induration and tenderness (eg, eyelid for a chalazion, under the medial canthus near the side of the nose for dacryocystitis, and medial to the punctum for canaliculitis).
Chronic chalazia that do not respond to treatment require biopsy to exclude tumor of the eyelid.
Treatment of Chalazion and Hordeolum
Warm compresses
Sometimes incision and drainage or medications such as glucocorticoid injection (for chalazia) or oral antibiotics (for hordeola)
Warm compresses for 5 to 10 minutes 2 or 3 times a day can be used to hasten resolution of chalazia and external hordeola.
Chalazion
Incision and curettage or intralesional glucocorticoid therapy (eg, triamcinolone) may be indicated if chalazia are large, unsightly, and persist for more than several weeks despite conservative therapy (Incision and curettage or intralesional glucocorticoid therapy (eg, triamcinolone) may be indicated if chalazia are large, unsightly, and persist for more than several weeks despite conservative therapy (1).
Hordeolum
An external hordeolum that does not respond to warm compresses can be incised with a sharp, fine-tipped blade (2). Systemic antibiotics (eg, doxycycline or erythromycin) are indicated when ). Systemic antibiotics (eg, doxycycline or erythromycin) are indicated whenpreseptal cellulitis accompanies a hordeolum.
Treatment of an internal hordeolum is with oral antibiotics and incision and drainage if needed. Topical antibiotics are usually ineffective.
Treatment references
1. Tashbayev B, Chen X, Utheim TP: Chalazion treatment: A concise review of clinical trials. Curr Eye Res 9(2):109-118, 2024. doi:10.1080/02713683.2023.2279014
2. Lindsley K, Nichols JJ, Dickersin K. Non-surgical interventions for acute internal hordeolum. Cochrane Database Syst Rev. 2017;1(1):CD007742. Published 2017 Jan 9. doi:10.1002/14651858.CD007742.pub4
Key Points
Chalazia and hordeola initially cause eyelid hyperemia and edema, swelling, and pain and may be clinically indistinguishable for a few days.
A hordeolum remains painful and localizes to an eyelid margin.
Warm compresses can hasten resolution of either lesion.
Other treatments that may be needed include intralesional glucocorticoids (for chalazia) and incision and/or antibiotics (for hordeola).
Consider biopsy to exclude eyelid tumor for chronic chalazia that do not respond to usual treatments.





