

Lice can infect the scalp, body, pubis, and eyelashes. Head lice are transmitted by close contact; body lice are transmitted in cramped, crowded conditions; and pubic lice are transmitted by sexual contact. Symptoms, signs, diagnosis, and treatment differ by location of infestation.
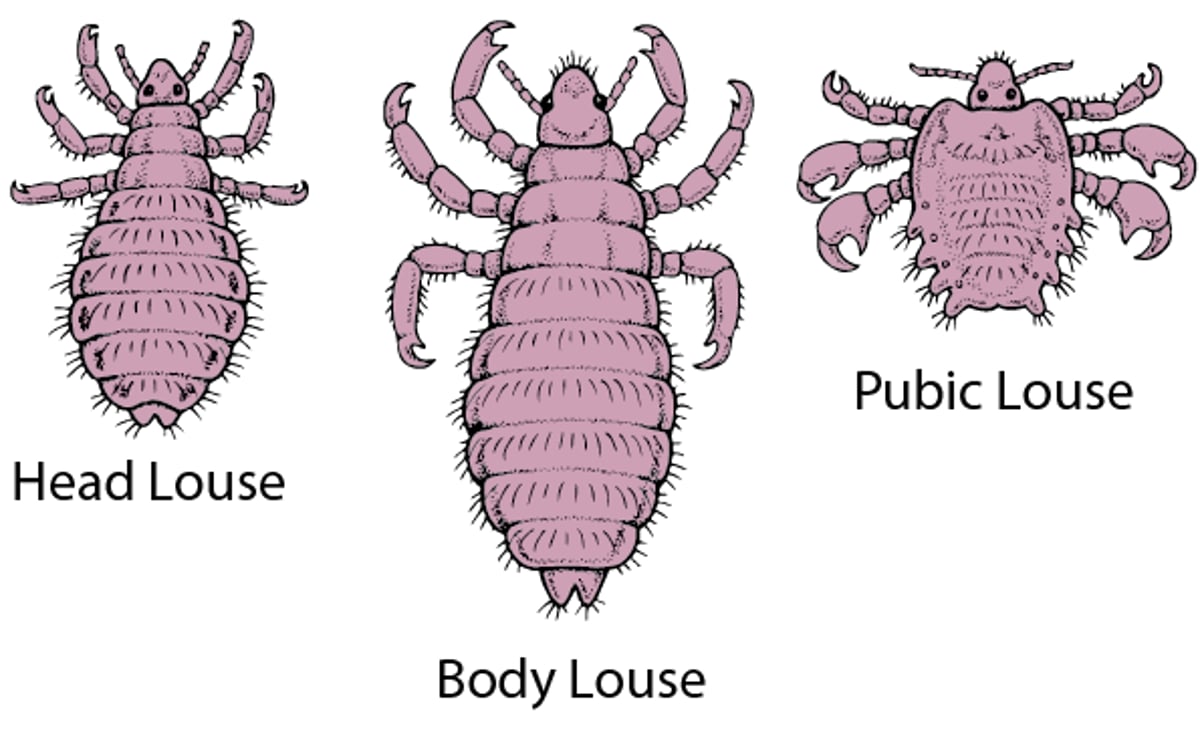
Lice are wingless, blood-sucking insects that infest the head (Pediculus humanus var. capitis), body (P. humanus var. corporis), or pubis (Phthirus pubis). The 3 types of lice differ substantially in morphology and clinical features (see figure ). Head lice and pubic lice live directly on the host; body lice live in garments. All types occur worldwide.
Head lice
A Close-Up Look at Lice

An estimated 6 to 12 million infestations of head lice occur each year in the United States among young children (1). Head lice are most common among girls aged 5 to 11 years but can affect almost anyone; infestations are less common in Black people (2). Head lice are easily transmitted from person to person in close contact (as occurs within households and classrooms) and may be ejected from hair by static electricity or wind; transmission by these routes (or by sharing of combs, brushes, and hats) is likely but unproved. Although poor hygiene or low socioeconomic status have been implicated as risk factors, this has not been conclusively established (3).
Infestation typically involves the hair and scalp but may involve other hair-bearing areas. Active infestation usually involves ≤ 20 lice and causes severe pruritus. Examination is most often normal but may reveal scalp excoriations and posterior cervical adenopathy.
Diagnosis of head lice depends on demonstration of living lice. Lice are detected by a thorough combing-through of wet hair from the scalp with a fine-tooth comb (teeth of comb approximately 0.2 mm apart); lice are usually found at the back of the head or behind the ears. Nits are more commonly seen and are ovoid, grayish white eggs fixed to the base of hair shafts. Each adult female louse lays 3 to 5 eggs/day, so nits typically vastly outnumber lice and are not a measure of severity of infestation.


Lice nits are ovoid, grayish white eggs fixed to the hair shafts (top); they have a distinctive appearance on low-power microscopy (bottom).
Initial treatment of head lice with topical pediculicides is outlined in the table Initial Treatment Options for Lice. Medication resistance is common, and the initial choice should be based on local resistance patterns and adverse effects (4). Topical therapies include malathion, permethrin or other pyrethroids, spinosad, and ivermectin (). Topical therapies include malathion, permethrin or other pyrethroids, spinosad, and ivermectin (5). Lindane shampoo is no longer recommended because of the widespread resistance and risk of neurotoxicity (). Lindane shampoo is no longer recommended because of the widespread resistance and risk of neurotoxicity (6). Oral ivermectin is typically reserved for refractory infestations (). Oral ivermectin is typically reserved for refractory infestations (7).
After applying a topical pediculicide, nits are removed by using a fine-tooth comb on wet hair (wet combing). Termination or removal of live (viable) nits is important in preventing reinfestation; live nits fluoresce on illumination with a Wood lamp. Most pediculicides also kill nits. Dead nits remain after successful treatment and do not signify active infection; they do not have to be removed. Nits grow away from the scalp with time; the absence of nits less than one fourth of an inch from the scalp rules out current active infection. Hot air has been shown to kill > 88% of nits but has been variably effective in killing hatched lice. Thirty minutes of hot air, slightly cooler than a blow dryer, may be an effective adjunctive measure to treat head lice.
Controversy surrounds the need to clean the personal items of people with lice or nits and the need to exclude children with head lice or nits from school; there are no conclusive data supporting either approach. The U.S. Centers for Disease Control and Prevention (CDC) recommends that children diagnosed with head lice do not need to be sent home early from school. They should be sent home from school at the end of the day and may return after appropriate treatment has been started (1). However, some experts recommend replacement of personal items or thorough cleaning, followed by drying at 54° C (130° F) for 30 minutes. Items that cannot be washed may be placed in airtight plastic bags for 2 weeks to kill the lice, which live only approximately 10 days.
Body lice
Body lice primarily live on bedding and clothing, not people, and are most frequently found in cramped, crowded conditions (eg, military barracks, some households), conditions with poor hygiene, and places with communal beds. Transmission is by sharing of contaminated clothing and bedding. Body lice are main vectors of epidemic typhus, trench fever, and relapsing fever.


Louse-borne relapsing fever is caused by Borrelia recurrentis, which is transmitted to humans by body lice.
Body lice cause pruritus; signs are small red puncta caused by bites, usually associated with linear scratch marks, urticaria, or superficial bacterial infection. These findings are especially common on the shoulders, buttocks, and abdomen. Nits may be present on body hairs.
The diagnosis of body lice is based on demonstration of lice and nits in clothing, especially at the seams.
Primary treatment of body lice is thorough cleaning (eg, cleaning, followed by drying at 65° C [149° F]) or replacement of clothing and bedding, which is often difficult because affected people can often have few resources and limited control over their environment (8).
Pubic lice
Pubic lice (“crabs”) are sexually transmitted infestations in adolescents and adults and may be transmitted to children by close parental contact. They may also be transmitted by fomites (eg, towels, bedding, clothing). They most commonly infest pubic and perianal hairs but may spread to the thighs, trunk, and facial hair (ie, beard, mustache, and eyelashes).


© Springer Science+Business Media


Image provided by Thomas Habif, MD.


Pubic lice may spread to the eyelashes. This photo shows eyelashes infested with a louse and nits.
Pubic lice may spread to the eyelashes. This photo shows eyelashes infested with a louse and nits.
PAUL PARKER/SCIENCE PHOTO LIBRARY


Maculae ceruleae are the blue spots in the thigh. They are thought to be secondary to anticoagulant activity of louse saliva.
Maculae ceruleae are the blue spots in the thigh. They are thought to be secondary to anticoagulant activity of louse s
© Springer Science+Business Media


© Springer Science+Business Media


Louse excreta are the reddish brown dots on the skin.
Louse excreta are the reddish brown dots on the skin.
© Springer Science+Business Media


© Springer Science+Business Media
© Springer Science+Business Media
Image provided by Thomas Habif, MD.
Pubic lice may spread to the eyelashes. This photo shows eyelashes infested with a louse and nits.
Pubic lice may spread to the eyelashes. This photo shows eyelashes infested with a louse and nits.
PAUL PARKER/SCIENCE PHOTO LIBRARY
Maculae ceruleae are the blue spots in the thigh. They are thought to be secondary to anticoagulant activity of louse saliva.
Maculae ceruleae are the blue spots in the thigh. They are thought to be secondary to anticoagulant activity of louse s
© Springer Science+Business Media
© Springer Science+Business Media
Louse excreta are the reddish brown dots on the skin.
Louse excreta are the reddish brown dots on the skin.
© Springer Science+Business Media
© Springer Science+Business Media
Pubic lice cause pruritus. Physical signs are few, but some patients have excoriations and regional lymphadenopathy and/or lymphadenitis. Pale, bluish gray skin macules (maculae ceruleae) on the trunk, buttocks, and thighs are caused by anticoagulant activity of louse saliva while feeding; they are unusual but characteristic of infestation. Eyelash infestation manifests as eye itching, burning, and irritation.
Diagnosis of pubic lice is by demonstration of nits, lice, or both by close inspection (such as with a Wood lamp) or microscopic analysis. A supporting sign of infestation is scattering of dark brown specks (louse excreta) on skin or undergarments.
The treatment of pubic lice is outlined in the table . Initial treatment is typically with topical pediculicides (9) Oral ivermectin is sometimes used for patients with pubic lice infestation that is refractory to topical therapies. The treatment of eyelid and eyelash infestation is often difficult and involves use of petrolatum, physostigmine ointment, oral ivermectin, or physical removal of lice with forceps. Household inhabitants should be inspected and treated if there is evidence of an active infestation. Sex partners should also be treated.) Oral ivermectin is sometimes used for patients with pubic lice infestation that is refractory to topical therapies. The treatment of eyelid and eyelash infestation is often difficult and involves use of petrolatum, physostigmine ointment, oral ivermectin, or physical removal of lice with forceps. Household inhabitants should be inspected and treated if there is evidence of an active infestation. Sex partners should also be treated.
Initial Treatment Options for Lice
Therapy | Instructions | Comments |
|---|---|---|
Lice, head | ||
Ivermectin 0.5% lotionIvermectin 0.5% lotion | Apply lotion to dry hair to coat the hair and scalp; rinse after 10 minutes with water Single-use application | For use in patients > 6 months of age |
Permethrin (eg, 1% lotion or cream rinse), other pyrethroid or pyrethrin lotions*Permethrin (eg, 1% lotion or cream rinse), other pyrethroid or pyrethrin lotions* | Wash hair and apply to wet hair, behind ears and on nape; wash off in 10 minutes May repeat in 7 days if live nits (closer than a 1/4 inch away from the scalp) are seen | Contraindicated in patients sensitive to the chrysanthemum family of plants |
Spinosad 0.9% topical suspensionSpinosad 0.9% topical suspension | Apply to dry scalp and rub in until scalp is moistened, then apply to dry hair, completely covering the scalp and hair; leave on for 10 minutes then thoroughly rinse off with warm water If live lice are seen after 7 days, a second treatment should be performed | For use in patients ≥ 4 years of age Contains benzyl alcohol and derivatives; avoid in neonates and those younger than 6 months of age because of potential toxicity and in patients with sensitivity to benzyl alcoholContains benzyl alcohol and derivatives; avoid in neonates and those younger than 6 months of age because of potential toxicity and in patients with sensitivity to benzyl alcohol May cause eyelid redness and swelling; avoid contact with eyes |
Malathion 0.5% lotionMalathion 0.5% lotion | Apply to dry hair and scalp, wash and rinse in 8–12 hours, shampoo scalp, and remove nits May repeat in 7–9 days if live nits (nits closer than a 1/4 inch away from the scalp) are seen | Highly effective but not 1st-line treatment because of flammability and unpleasant odor |
Wet combing with a metal nit comb | Should be combined with all of the therapies | — |
Lice, body | ||
— | Treatment of pruritus and secondary infection | Topical measures not used because body lice are found in clothing Wash clothes and linens and dry them at 65° C (149° F) Dry cleaning or ironing clothes |
Lice, pubic | ||
Permethrin 1% (60 mL) creamPermethrin 1% (60 mL) cream | Same as for head lice Must repeat in 10 days | — |
Pyrethrins* with piperonyl butoxide (60 mL) shampoo | Apply to dry hair and skin, leave on for 10 minutes, rinse, and repeat in 7–10 days | Cannot be applied more than twice in 24 hours |
Lice, eyelashes | ||
Fluorescein drops 10–20%Fluorescein drops 10–20% | Applied to the eyelids | Provides immediate pediculicidal effect |
Petrolatum ointment | Apply 3–4 times a day for 8–10 days | — |
* Pyrethrins are natural components of chrysanthemum flowers, with strong insecticidal activity; pyrethroids are synthetic and natural relatives of pyrethrin; and permethrin is a commonly used synthetic pyrethroid. Pyrethrins are combined with a piperic acid derivative (piperonyl butoxide) to enhance efficacy.* Pyrethrins are natural components of chrysanthemum flowers, with strong insecticidal activity; pyrethroids are synthetic and natural relatives of pyrethrin; and permethrin is a commonly used synthetic pyrethroid. Pyrethrins are combined with a piperic acid derivative (piperonyl butoxide) to enhance efficacy. | ||
References
1. U.S. Centers for Disease Control and Prevention (CDC). About Head Lice. June 4, 2024. Accessed October 16, 2025.
2. Meinking TL, Burkhart CG, Burkhart CN. Head lice. N Engl J Med347(17):1381-1382, 2002; author reply 1381-2. doi: 10.1056/NEJM200210243471720
3. Falagas ME, Matthaiou DK, Rafailidis PI, et al. Worldwide prevalence of head lice. Emerg Infect Dis. 2008;14(9):1493-1494. doi:10.3201/eid1409.080368
4. Thomas C, Castillo Valladares H, Berger TG, Chang AY. Scabies, Bedbug, and Body Lice Infestations: A Review. JAMA. Published online September 9, 2024. doi:10.1001/jama.2024.13896
5.Nolt D, Moore S, Yan AC, et al. Head lice. Pediatrics 2022;150(4):e2022059282. doi:10.1542/peds.2022-059282
6. Nolan K, Kamrath J, Levitt J. Lindane toxicity: A comprehensive review of the medical literature. . Lindane toxicity: A comprehensive review of the medical literature.Pediatr Dermatol.29(2):141-146, 2012. doi: 10.1111/j.1525-1470.2011.01519.x
7. Chosidow O, Giraudeau B, Cottrell J, et al. Oral ivermectin versus malathion lotion for difficult-to-treat head lice. . Oral ivermectin versus malathion lotion for difficult-to-treat head lice.N Engl J Med362(10):896-905, 2010. doi: 10.1056/NEJMoa0905471. Erratum in: N Engl J Med 362(17):1647, 2010. PMID: 20220184.
8. Nyers ES, Elston DM. What's eating you? Human body lice (Pediculus humanus corporis). Cutis 105(3):118-120, 2020. PMID: 32352435
9. U.S. Centers for Disease Control and Prevention (CDC). Treatment of Head Lice. November 12, 2024. Accessed October 16, 2025.
Key Points
Head and pubic lice live on people, whereas body lice live in garments.
Confirm the diagnosis of lice by finding live lice or live nits.
Treat head or pubic lice with a topical medication (eg, a pyrethroid) or, when refractory to topical therapy, with oral ivermectin.Treat head or pubic lice with a topical medication (eg, a pyrethroid) or, when refractory to topical therapy, with oral ivermectin.
Treat body lice symptomatically and by eliminating the source of lice.
Drug Information for the Topic





