



Brugada syndrome is an inherited channelopathy, characterized by large J-waves and coved ST elevation with associated T-wave inversion in leads V1-V3, that causes an increased risk of ventricular tachycardia (VT) and ventricular fibrillation (VF), leading to syncope and sudden death. Diagnosis is by ECG and often provocative electrodiagnostic testing and/or genetic testing. Treatment is with an implanted cardioverter-defibrillator. Family members should be screened.
Overall the incidence of Brugada syndrome is approximately 5 in 10,000 (1) with wide variation in ethnicity and, consequently, geographic region. The majority of patients with clinically apparent Brugada syndrome are male (80 to 90%) (2, 3). Brugada syndrome may be responsible for up to approximately one-third of sudden cardiac deaths in young males (4, 5). (See also Overview of Arrhythmias and Overview of Channelopathies.)
General references
1. Vutthikraivit W, Rattanawong P, Putthapiban P, et al: Worldwide Prevalence of Brugada Syndrome: A Systematic Review and Meta-Analysis. Acta Cardiol Sin 34(3):267–277, 2018. doi: 0.6515/ACS.201805_34(3).20180302B
2. Krahn AD, Behr ER, Hamilton R, Probst V, Laksman Z, Han HC. Brugada Syndrome. JACC Clin Electrophysiol. 2022;8(3):386-405. doi:10.1016/j.jacep.2021.12.001
3. Sroubek J, Probst V, Mazzanti A, et al. Programmed Ventricular Stimulation for Risk Stratification in the Brugada Syndrome: A Pooled Analysis. Circulation. 2016;133(7):622-630. doi:10.1161/CIRCULATIONAHA.115.017885
4. Gaita F, Cerrato N, Giustetto C, Garberoglio L, Calò L. Brugada syndrome: identification of subjects at risk and therapy. Eur Heart J Suppl. 2024;26(Suppl 1):i69-i73. doi:10.1093/eurheartjsupp/suae021
5. Wilde AAM, Semsarian C, Márquez MF, et al. European Heart Rhythm Association (EHRA)/Heart Rhythm Society (HRS)/Asia Pacific Heart Rhythm Society (APHRS)/Latin American Heart Rhythm Society (LAHRS) Expert Consensus Statement on the state of genetic testing for cardiac diseases. Europace. 2022;24(8):1307-1367. doi:10.1093/europace/euac030
Pathophysiology of Brugada Syndrome
Brugada syndrome results from mutations that:
Decrease inward sodium or calcium currents OR
Increase early outward potassium currents
These abnormalities lead to early loss of the action potential plateau, particularly in the epicardial cells of the right ventricular outflow tract that produce characteristic right precordial ECG changes and a propensity to ventricular tachyarrhythmias. Although different mutations have been reported, most are in the SCN5A gene, producing a loss-of-function of the inward sodium current (1).
Typically, patients have no clinical evidence of structural heart disease, although most have microscopic structural abnormalities in the epicardial region of the right ventricular outflow tract. Relationships with other genetic and acquired structural heart diseases are increasingly being recognized, as are overlap syndromes with long QT syndrome type 3, early repolarization syndrome, and arrhythmogenic right ventricular cardiomyopathy (ARVC) (1, 2, 3).
Pathophysiology references
1. Antzelevitch C, Yan GX, Ackerman MJ, et al. J-Wave syndromes expert consensus conference report: Emerging concepts and gaps in knowledge. Europace. 2017;19(4):665-694. doi:10.1093/europace/euw235
2. Moncayo-Arlandi J, Brugada R. Unmasking the molecular link between arrhythmogenic cardiomyopathy and Brugada syndrome. Nat Rev Cardiol. 2017;14(12):744-756. doi:10.1038/nrcardio.2017.103
3. Veltmann C, Barajas-Martinez H, Wolpert C, et al. Further Insights in the Most Common SCN5A Mutation Causing Overlapping Phenotype of Long QT Syndrome, Brugada Syndrome, and Conduction Defect. J Am Heart Assoc. 2016;5(7):e003379. doi:10.1161/JAHA.116.003379
Symptoms and Signs of Brugada Syndrome
The majority of patients diagnosed with Brugada syndrome are asymptomatic (1). However, in some patients it leads to syncope or sudden cardiac death due to polymorphic ventricular tachycardia and ventricular fibrillation. Ventricular arrhythmias can cause sudden death during sleep. Approximately 10 to 20% of patients develop atrial tachyarrhythmias, predominantly atrial fibrillation (2, 3), and some present with atrial fibrillation as the first clinical manifestation of disease (4).
Events occur more often at night and are not usually related to exercise. Events may also be brought on by fever and by certain medications, including sodium channel blockers, beta-blockers, certain antidepressants and antipsychotics, lithium, alcohol, and cocaine (5).
Symptoms and signs references
1. Krahn AD, Behr ER, Hamilton R, Probst V, Laksman Z, Han HC. Brugada Syndrome. JACC Clin Electrophysiol. 2022;8(3):386-405. doi:10.1016/j.jacep.2021.12.001
2. Bordachar P, Reuter S, Garrigue S, et al. Incidence, clinical implications and prognosis of atrial arrhythmias in Brugada syndrome. Eur Heart J. 2004;25(10):879-884. doi:10.1016/j.ehj.2004.01.004
3. Giustetto C, Cerrato N, Gribaudo E, et al: Atrial fibrillation in a large population with Brugada electrocardiographic pattern: prevalence, management, and correlation with prognosis. Heart Rhythm 11(2):259–265, 2014. doi: 10.1016/j.hrthm.2013.10.043
4. Rodríguez-Mañero M, Namdar M, Sarkozy A, et al: Prevalence, clinical characteristics and management of atrial fibrillation in patients with Brugada syndrome. Am J Cardiol 111(3):362–367, 2013. doi:10.1016/j.amjcard.2012.10.012
5. Antzelevitch C, Yan GX, Ackerman MJ, et al. J-Wave syndromes expert consensus conference report: Emerging concepts and gaps in knowledge. Europace. 2017;19(4):665-694. doi:10.1093/europace/euw235
Diagnosis of Brugada Syndrome
Electrocardiography (ECG)
Family history
Provocative testing to induce characteristic ECG changes
Genetic testing
Diagnosis should be considered in patients with unexplained cardiac arrest or syncope or a family history of such when the affected people do not have structural heart disease.
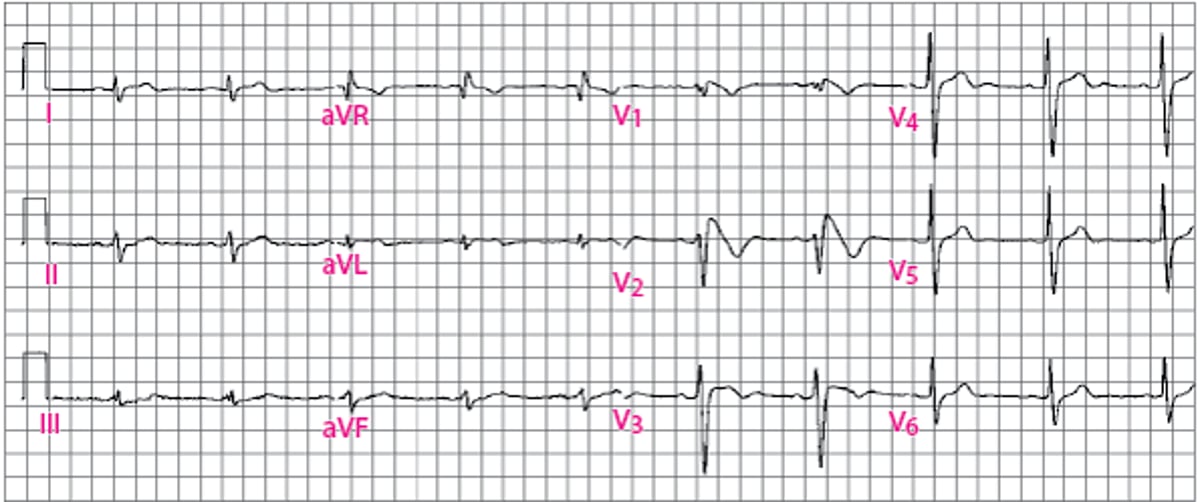
Initial diagnosis of Brugada syndrome is based on a characteristic ECG pattern, the type 1 Brugada ECG pattern (see figure ). The type 1 Brugada ECG pattern has prominent J-point and ST elevation in V1 and V2 (sometimes involving V3) that causes the QRS complex in these leads to resemble right bundle branch block. The ST segment is coved and descends to an inverted T-wave. These characteristics may be more evident in V1 and V2 leads recorded from the second or third intercostal spaces rather than the usual fourth intercostal space. Only a spontaneous type 1 pattern is considered diagnostic for Brugada syndrome according to the Shanghai Brugada syndrome score (1).
Lesser degrees of these patterns (type 2 and type 3 Brugada ECG patterns) are not considered diagnostic. The type 2 and type 3 patterns may change to a type 1 pattern spontaneously, with fever, or in response to medications. The latter is the basis of a provocative challenge usually using IV ajmaline, procainamide, flecainide or pilsicainide. Scores have been developed to aid in diagnosing Brugada syndrome, with a diagnosis of "possible" Brugada syndrome defined for borderline cases (1). Application of clinical, family history, and genetic criteria is the required to establish the diagnosis (1).
Genetic testing is usually recommended and has a yield of approximately 20% (2).
The diagnosis of Brugada syndrome includes considering, and excluding, other disorders that produce similar cardiac findings, including hypothermia, hypocalcemia, right bundle branch block, arrhythmogenic right ventricular cardiomyopathy, acute pulmonary embolism, and left anterior descending coronary artery of conus branch of the right coronary artery occlusion (1).
Type 1 Brugada ECG Pattern
Prominent J-point elevation to a coved ST segment, leading to an inverted T-wave in leads V1 and V2. |

Diagnosis references
1. Antzelevitch C, Yan GX, Ackerman MJ, et al. J-Wave syndromes expert consensus conference report: Emerging concepts and gaps in knowledge. Europace. 2017;19(4):665-694. doi:10.1093/europace/euw235
2. Wilde AAM, Semsarian C, Márquez MF, et al. European Heart Rhythm Association (EHRA)/Heart Rhythm Society (HRS)/Asia Pacific Heart Rhythm Society (APHRS)/Latin American Heart Rhythm Society (LAHRS) Expert Consensus Statement on the state of genetic testing for cardiac diseases. J Arrhythm. 2022;38(4):491-553. doi: 10.1002/joa3.12717
Treatment of Brugada Syndrome
Sometimes an implantable cardioverter-defibrillator (ICD)
Quinidine
Catheter ablation
Screening of family members
It is important to avoid factors that can trigger arrhythmias. Patients should monitor their temperature during infectious illness and take antipyretic therapy for fever. When possible, clinicians should stop any predisposing medications and prescribe alternatives. Patients should avoid substances, particularly cocaine and excessive alcohol, that are arrhythmogenic in Brugada syndrome (for an up-to-date list, see www.brugadadrugs.org).
Patients with a spontaneous or provoked type 1 Brugada syndrome ECG pattern and sustained VT, cardiac arrest, and in some cases syncope presumed to be due to ventricular arrhythmia, should typically have an implantable cardioverter-defibrillator (ICD) (1, 2).
Optimal treatment of Brugada syndrome in patients diagnosed based on ECG pattern and family history but who do not have syncope or arrhythmia is unclear, although they do have increased risk of sudden death. Multiple scoring systems have been developed to aid in determining if an ICD is appropriate therapy in such patients (3, 4, 5).
The role of electrophysiologic testing for risk stratification in patients with type 1 Brugada ECG but no arrhythmia symptoms is currently debated. In asymptomatic patients with a spontaneous type 1 Brugada ECG, inducible ventricular tachycardia or ventricular fibrillation with programmed ventricular stimulation limited to 2 extra stimuli is associated with an increased risk of future serious arrhythmic events (6). Thus, electrophysiology study may be considered in asymptomatic patients with a spontaneous type 1 Brugada ECG, particularly if the result would influence the decision to place an ICD (eg, if inducible ventricular arrhythmia is demonstrated) (1, 2).
When frequent ICD discharges need to be suppressed, or when the patient qualifies for an ICD but declines, quinidine, which blocks the transient outward potassium current that may be increased in Brugada syndrome, should be used, or considered (1, 2). IV isoproterenol has also been used for frequently recurrent ventricular tachyarrhythmias (7). In patients refractory to such therapy, catheter ablation of the arrhythmogenic substrate may be considered (8).
Treatment references
1. Al-Khatib SM, Stevenson WG, Ackerman MJ, et al: 2017 AHA/ACC/HRS Guideline for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation. 2018;138(13):e272-e391. doi: 10.1161/CIR.0000000000000549
2. Zeppenfeld K, Tfelt-Hansen J, de Riva M, et al. 2022 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur Heart J. 2022;43(40):3997-4126. doi:10.1093/eurheartj/ehac262
3. Kawada S, Morita H, Antzelevitch C, et al. Shanghai Score System for Diagnosis of Brugada Syndrome: Validation of the Score System and System and Reclassification of the Patients. JACC Clin Electrophysiol. 2018;4(6):724-730. doi:10.1016/j.jacep.2018.02.009
4. Honarbakhsh S, Providencia R, Garcia-Hernandez J, et al. A Primary Prevention Clinical Risk Score Model for Patients With Brugada Syndrome (BRUGADA-RISK). JACC Clin Electrophysiol. 2021;7(2):210-222. doi:10.1016/j.jacep.2020.08.032
5. Rattanawong P, Mattanapojanat N, Mead-Harvey C, et al. Predicting arrhythmic event score in Brugada syndrome: Worldwide pooled analysis with internal and external validation. Heart Rhythm. 2023;20(10):1358-1367. doi:10.1016/j.hrthm.2023.06.013
6. Sroubek J, Probst V, Mazzanti A, et al. Programmed Ventricular Stimulation for Risk Stratification in the Brugada Syndrome: A Pooled Analysis. Circulation. 2016;133(7):622-630. doi:10.1161/CIRCULATIONAHA.115.017885
7. Brodie OT, Michowitz Y, Belhassen B: Pharmacological Therapy in Brugada Syndrome. Arrhythm Electrophysiol Rev 7(2):135–142, 2018. doi: 10.15420/aer.2018.21.2
8.Antzelevitch C, Yan GX, Ackerman MJ, et al. J-Wave syndromes expert consensus conference report: Emerging concepts and gaps in knowledge. Europace. 2017;19(4):665-694. doi:10.1093/europace/euw235
Key Points
Brugada syndrome is a genetic disorder causing characteristic ECG changes and an increased risk of ventricular arrhythmias, which can cause syncope and sometimes sudden cardiac death at a relatively young age.
Risk factors for symptomatic arrhythmias include fever and numerous medications and other substances (eg, alcohol, cocaine).
Diagnosis is by ECG, sometimes with provocative testing.
An implantable cardioverter-defibrillator may be required.
Drug Information for the Topic





