

Metacarpal neck fractures usually result from an axial load (eg, from punching with a clenched fist).
(See also Overview of Fractures.)
This discussion pertains to fractures of the metacarpal bones other than the thumb metacarpal. Fractures of the neck of metacarpals 2 through 5 are common. They cause pain, swelling, tenderness, and sometimes deformity. may occur. The 5th metacarpal is most commonly injured by punching (boxer's fracture). When these fractures result from punching someone in the mouth, human oral flora may contaminate the wound, sometimes causing infection. Patients with fight bites require antibiotics.
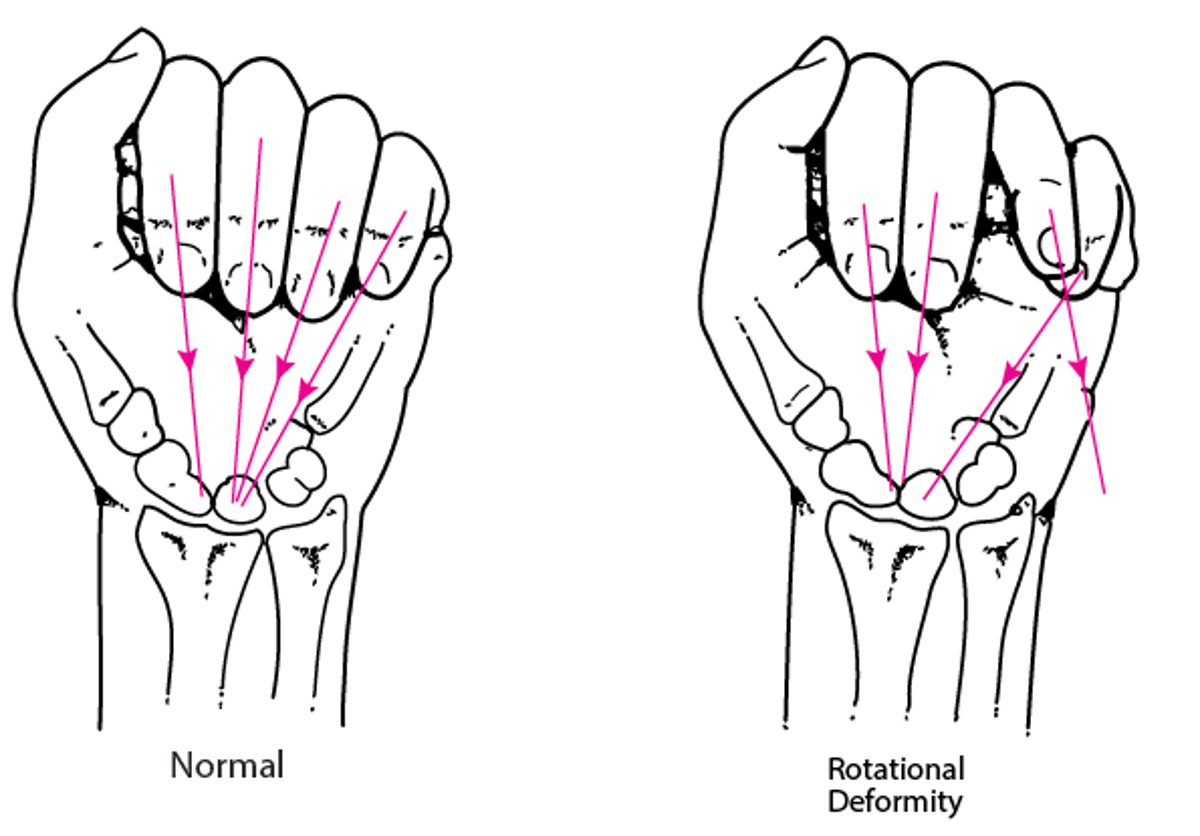
Rotational deformity due to a fracture in the hand
Normally, when the proximal interphalangeal joints are flexed to 90°, lines from the distal phalanges converge at a point on the proximal carpal bones. Deviation of one of these lines suggests a metacarpal fracture. |

Diagnosis of Metacarpal Neck Fractures
Radiographs


The 5th metacarpal neck bone is fractured midshaft.
The 5th metacarpal neck bone is fractured midshaft.
LIVING ART ENTERPRISES, LLC/SCIENCE PHOTO LIBRARY


This colored radiograph shows a fracture of the 5th metacarpal neck. In this view, angulation appears to be < 45°, suggesting that reduction is not necessary.
This colored radiograph shows a fracture of the 5th metacarpal neck. In this view, angulation appears to be < 45°, s
SCOTT CAMAZINE/SCIENCE PHOTO LIBRARY
The 5th metacarpal neck bone is fractured midshaft.
The 5th metacarpal neck bone is fractured midshaft.
LIVING ART ENTERPRISES, LLC/SCIENCE PHOTO LIBRARY
This colored radiograph shows a fracture of the 5th metacarpal neck. In this view, angulation appears to be < 45°, suggesting that reduction is not necessary.
This colored radiograph shows a fracture of the 5th metacarpal neck. In this view, angulation appears to be < 45°, s
SCOTT CAMAZINE/SCIENCE PHOTO LIBRARY
Typically, anteroposterior, lateral, and oblique views are diagnostic.
Treatment of Metacarpal Neck Fractures
Splinting
For certain fractures, reduction
Prophylactic antibiotics for open wounds
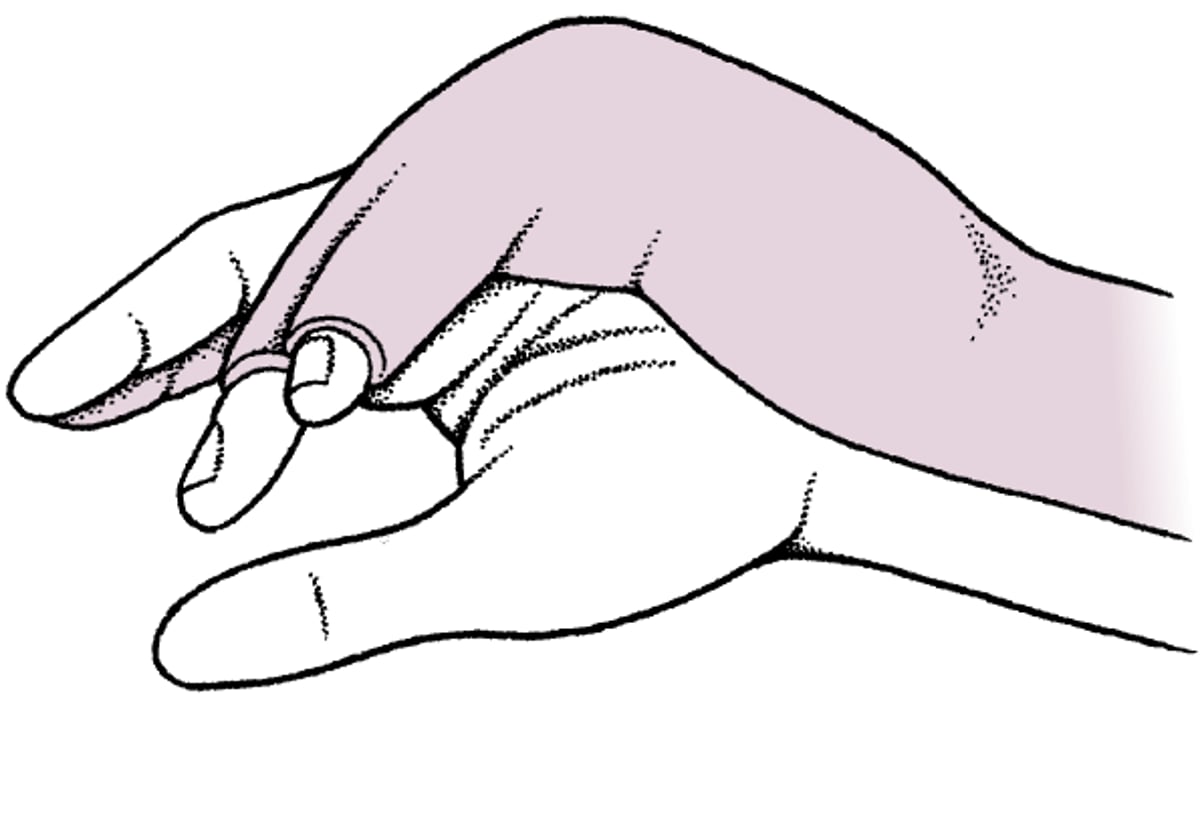
Treatment of a metacarpal neck fracture is with a splint (eg, an ulnar gutter splint for fractures of the 4th or 5th metacarpal), usually for at least a few weeks. Whether reduction is needed before the splint is applied depends on the fracture.
Reduction is not necessary for dorsal or volar angulation of
< 35° for the 4th metacarpal
< 45° for the 5th metacarpal
Reduction is necessary for
Rotational deformity of any metacarpal
Fractures of the 2nd and 3rd metacarpals with angulation
Usually, closed reduction is possible. Use of a hematoma block or an ulnar nerve block can help reduce the pain during reduction.
If patients have any wounds, particularly linear punctures, near the metacarpophalangeal joint, they should be specifically questioned about whether they punched someone in the mouth. If they did, contamination with human oral flora is possible, and measures to prevent infection (eg, wound exploration and cleaning, prophylactic antibiotics) are often required.
After the splint is removed, patients can gradually begin range-of-motion exercises.

Ulnar Gutter Splint

Key Points
Metacarpal neck fractures cause pain, swelling, tenderness, and sometimes deformity (eg, rotational deformity).
Take anteroposterior, lateral, and oblique radiographs.
If patients have wounds near the metacarpophalangeal joint, ask them whether they punched someone in the mouth; if they did, take measures to prevent infection (eg, prophylactic antibiotics).
Treat a metacarpal neck fracture with a splint; if angulation is significant or if rotational deformity is present, reduce the fracture first, usually using closed reduction.





