

Pemphigoid gestationis is a rare pruritic papular and vesicobullous eruption that occurs during pregnancy or postpartum. Diagnosis is clinical or by skin biopsy. Treatment is with topical or systemic corticosteroids. Most fetuses are unaffected, but neonatal morbidity or mortality is possible.
Pemphigoid gestationis appears to be an autoimmune phenomenon, probably caused by an IgG antibody to a 180-kD antigen in the basement membrane zone of the epidermis. Although previously called herpes gestationis (because the rash resembles the vesicobullous rash due to herpes simplex virus infection), this disorder is not caused by herpesvirus.
Pemphigoid gestationis occurs in 1/50,000 to 60,000 pregnancies (1); it usually begins during the second or third trimester but may begin during the first trimester or immediately postpartum. It usually recurs with subsequent pregnancies and occurs after oral contraceptive use in approximately 25% of women. Flare-ups are common 24 to 48 hours postpartum and can occur during subsequent menses or ovulation.
Most fetuses are unaffected; however, transient lesions occur in < 5% of neonates born to mothers with pemphigoid gestationis. Risks, including infant mortality, are likely due to placental insufficiency and are increased after preterm delivery and in infants who are small for gestational age.
Reference
1. Himeles JR, Pomeranz MK. Recognizing, Diagnosing, and Managing Pregnancy Dermatoses. Obstet Gynecol. 2022;140(4):679-695. doi:10.1097/AOG.0000000000004938
Symptoms and Signs of Pemphigoid Gestationis
The rash is very pruritic. Lesions often start around the umbilicus, then become widespread. Vesicles and bullae are the most specific lesions; erythematous plaques may develop. The palms, soles, trunk, buttocks, and extremities may be affected but usually not the face or mucous membranes.
The rash worsens during labor or immediately postpartum in up to 75% of women, typically remitting within a few weeks or months.


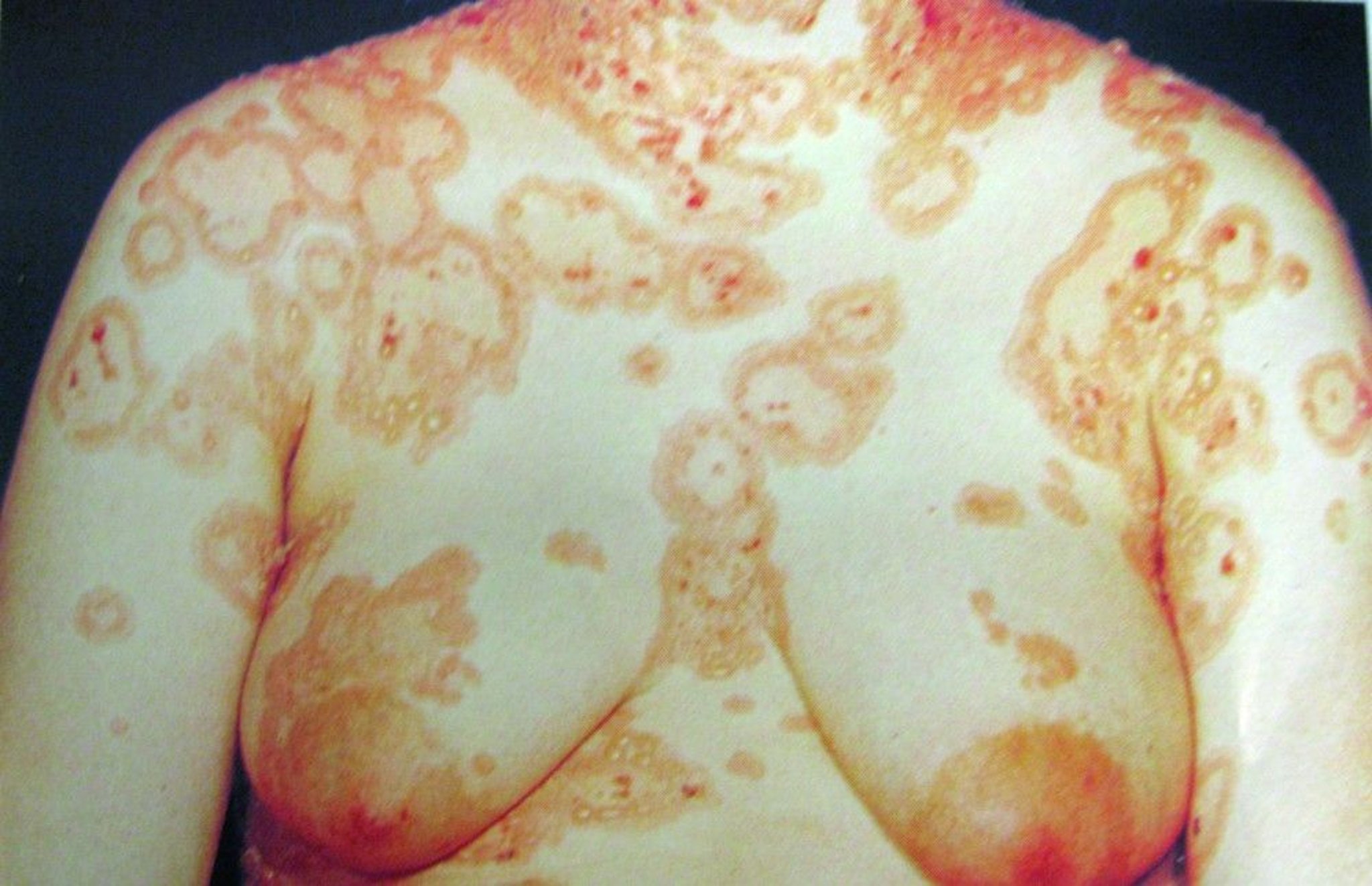
Pemphigoid gestationis can cause erythematous, urticariform, annular plaques on the trunk. In this patient, the rash has the multiforme-like iris configuration and involves the periumbilical area.
© Springer Science+Business Media

This photo shows the bullous pemphigoid-like eruption of pregnancy called pemphigoid gestationis. Vesicles and bullae are shown. Although the rash resembles the vesicobullous eruption of herpes simplex virus (hence the previous name herpes gestationis), the disorder is not an infection.
© Springer Science+Business Media
Neonates may have erythematous plaques or vesicles that resolve spontaneously in a few weeks.
Diagnosis of Pemphigoid Gestationis
Characteristic skin lesions
Sometimes biopsy with direct immunofluorescence
Pemphigoid gestationis may be confused clinically with several other pruritic eruptions of pregnancy, particularly polymorphic eruption of pregnancy. Pemphigoid gestationis can often be distinguished because it usually begins in the periumbilical area; polymorphic eruption of pregnancy usually begin in the striae.
Direct immunofluorescence examination of perilesional skin is diagnostic. It detects a linear band of C3 at the basement membrane zone.
Treatment of Pemphigoid Gestationis
Corticosteroids topically or, for severe symptoms, orally
Nonsedating oral antihistamines
For mild symptoms, topical corticosteroids (eg, 0.1% triamcinolone acetonide cream up to 6 times a day) may be effective. Prednisone (eg, 40 mg orally once a day) relieves moderate or severe pruritus and prevents new lesions; dose is tapered until few new lesions erupt, but it may need to be increased if symptoms become more severe (eg, during labor). Systemic corticosteroids given late in pregnancy and in short bursts, do not seem to harm the fetus.For mild symptoms, topical corticosteroids (eg, 0.1% triamcinolone acetonide cream up to 6 times a day) may be effective. Prednisone (eg, 40 mg orally once a day) relieves moderate or severe pruritus and prevents new lesions; dose is tapered until few new lesions erupt, but it may need to be increased if symptoms become more severe (eg, during labor). Systemic corticosteroids given late in pregnancy and in short bursts, do not seem to harm the fetus.
Nonsedating oral antihistamines can also be used to relieve pruritus.
Fetal status may be monitored with ultrasonography every 4 weeks if growth is normal or every 2 weeks if growth is restricted. Nonstress testing is also done when growth is restricted.
Key Points
Pemphigoid gestationis probably has an autoimmune etiology; it is not caused by herpesvirus, even though the rash resembles the vesicobullous rash due to herpes simplex virus infection.
Most fetuses are unaffected.
Try to differentiate the rash based on clinical criteria (eg, its initial appearance in the periumbilical area).
Treat women with topical corticosteroids or, if symptoms are severe, oral corticosteroids.
Drug Information for the Topic





