

The goal of a pelvic examination is to examine all the parts of the female reproductive anatomy. Whether to have a pelvic examination should be a shared decision between a woman and her doctor or other health care professional. (See also the American College of Obstetricians and Gynecologists (ACOG): Pelvic Exams—Frequently Asked Questions.)
If a woman has any questions or concerns about the pelvic examination, she should talk with her clinician beforehand. Women who have never had a pelvic examination should ask the clinician to explain what happens during the examination. If any part of the examination causes pain, a woman should be encouraged to let the clinician know during the examination.
A pelvic examination is done
When women have symptoms, such as pelvic pain or abnormal vaginal bleeding
When screening for cervical cancer or sexually transmitted infections (STIs) is needed
As part of a gynecologic procedure
Women should talk with their health care professional about whether and how often a pelvic examination needs to be done. A woman does not need a pelvic examination before starting a new birth control method, except for an intrauterine device. A pelvic examination is not consistently reliable as a way to detect ovarian cancer.
At age 21 to 25 years old, most women should start having tests to screen for cervical cancer, such as a Papanicolaou (Pap) test and/or testing for human papillomavirus (HPV). Screening tests are usually done every 3 to 5 years, depending on the person's age, type of test, risk factors for cervical cancer, and previous test results.
The pelvic examination includes the following:
Examination of the external female reproductive anatomy
Evaluation and examination of the internal female reproductive anatomy
Examination of the rectum (sometimes)
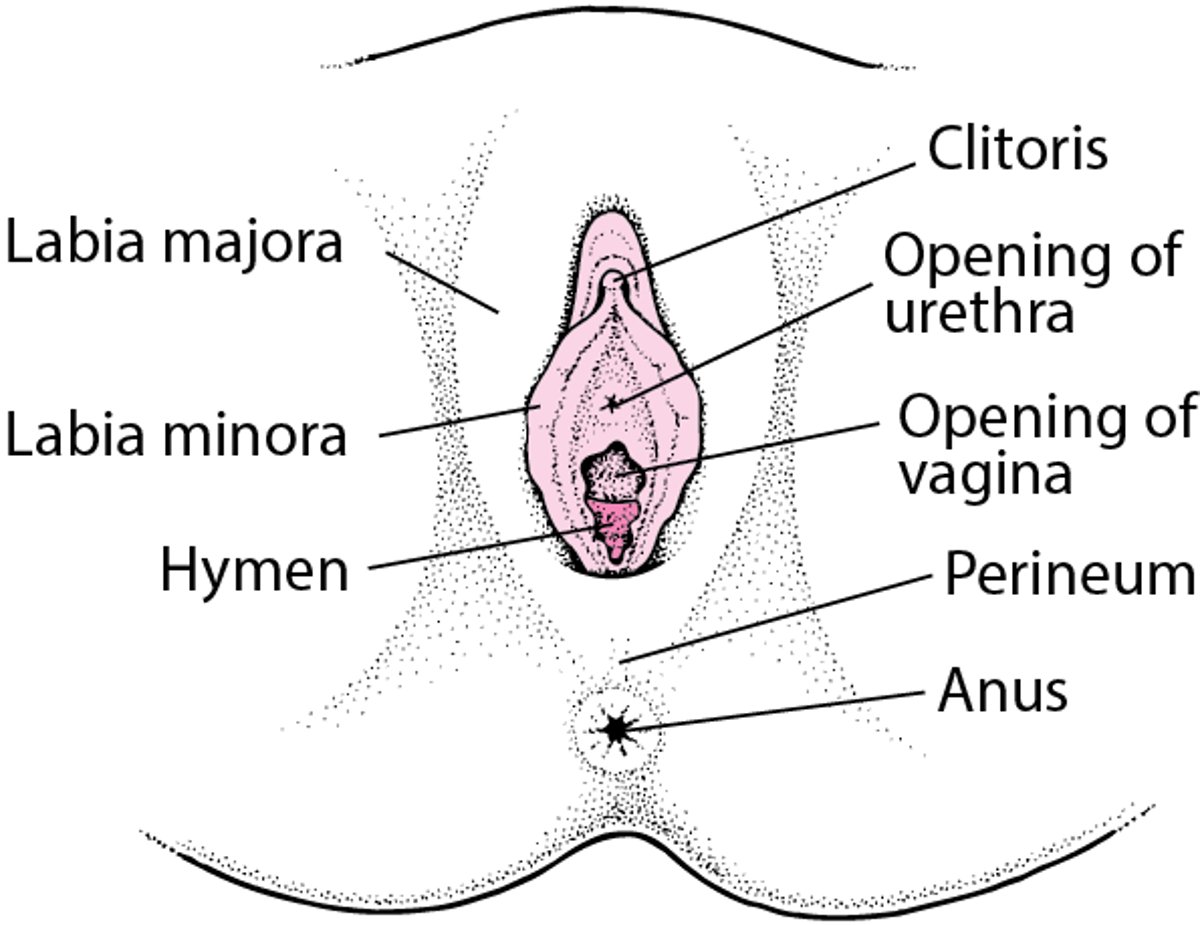
External Female Reproductive Anatomy

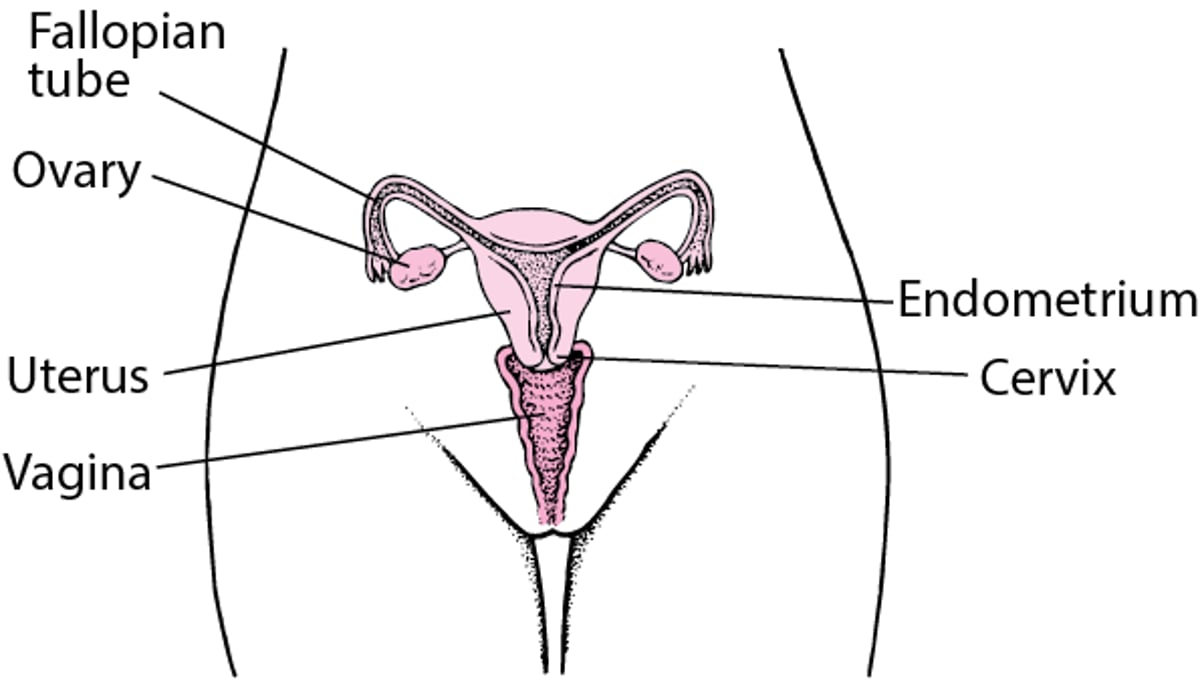
Internal Female Reproductive Anatomy

A woman should empty her bladder before the pelvic examination and may be asked to collect a urine sample for analysis. Usually, a gown or sheet is provided, and an assistant is present to chaperone and sometimes to help with the examination. If a woman wants to observe the pelvic examination, she should tell the clinician, who may be able to provide a mirror. The clinician may explain the examination or review the findings before, during, or after the examination.
During a pelvic examination, a woman lies on her back with her hips and knees bent and her buttocks at the edge of the examining table. This position helps to open up the pelvis so the clinician can examine the internal gynecologic anatomy. Special pelvic examination tables have heel stirrups to help a woman maintain this position. Before the pelvic examination begins, the clinician asks the woman to relax her legs and hips.

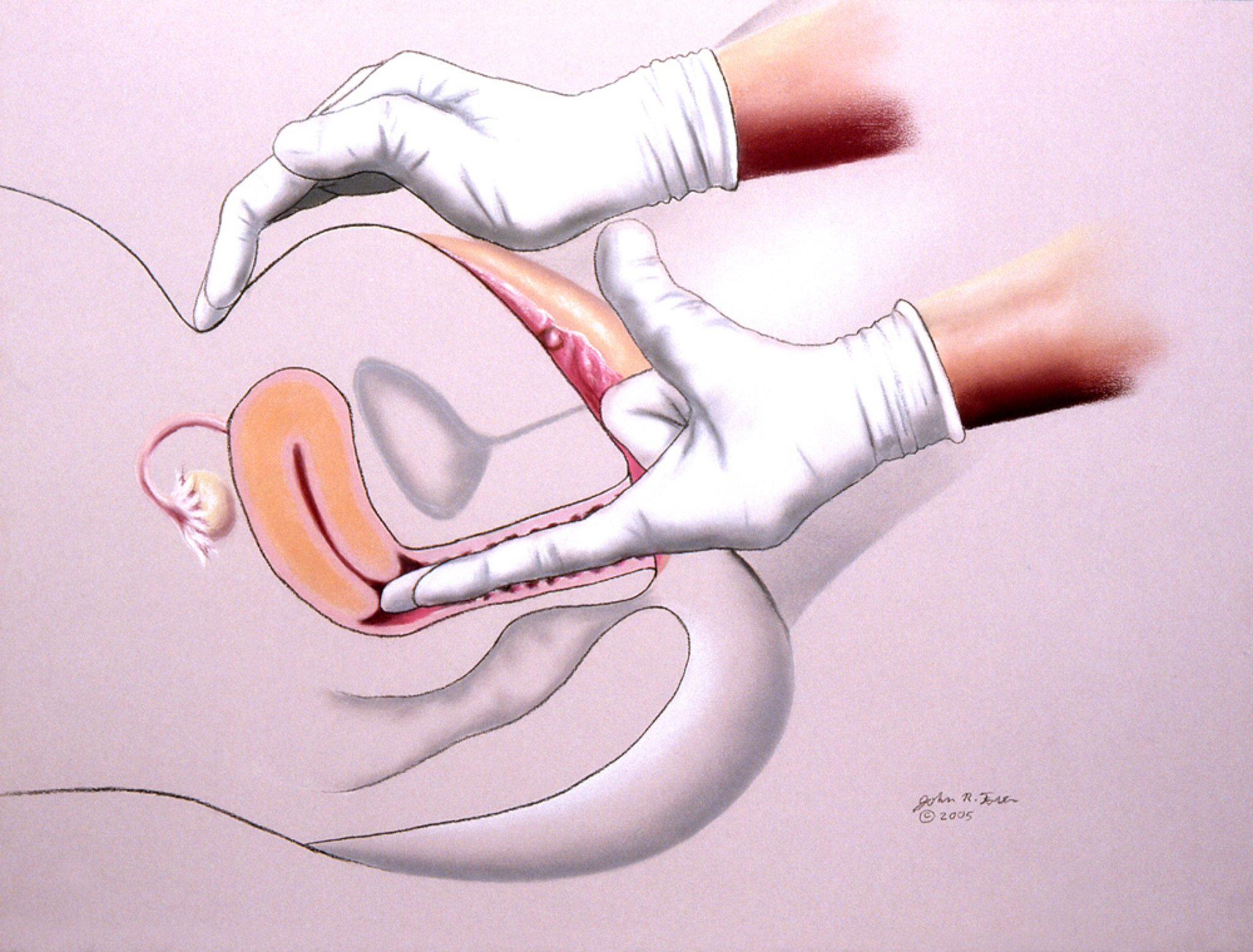
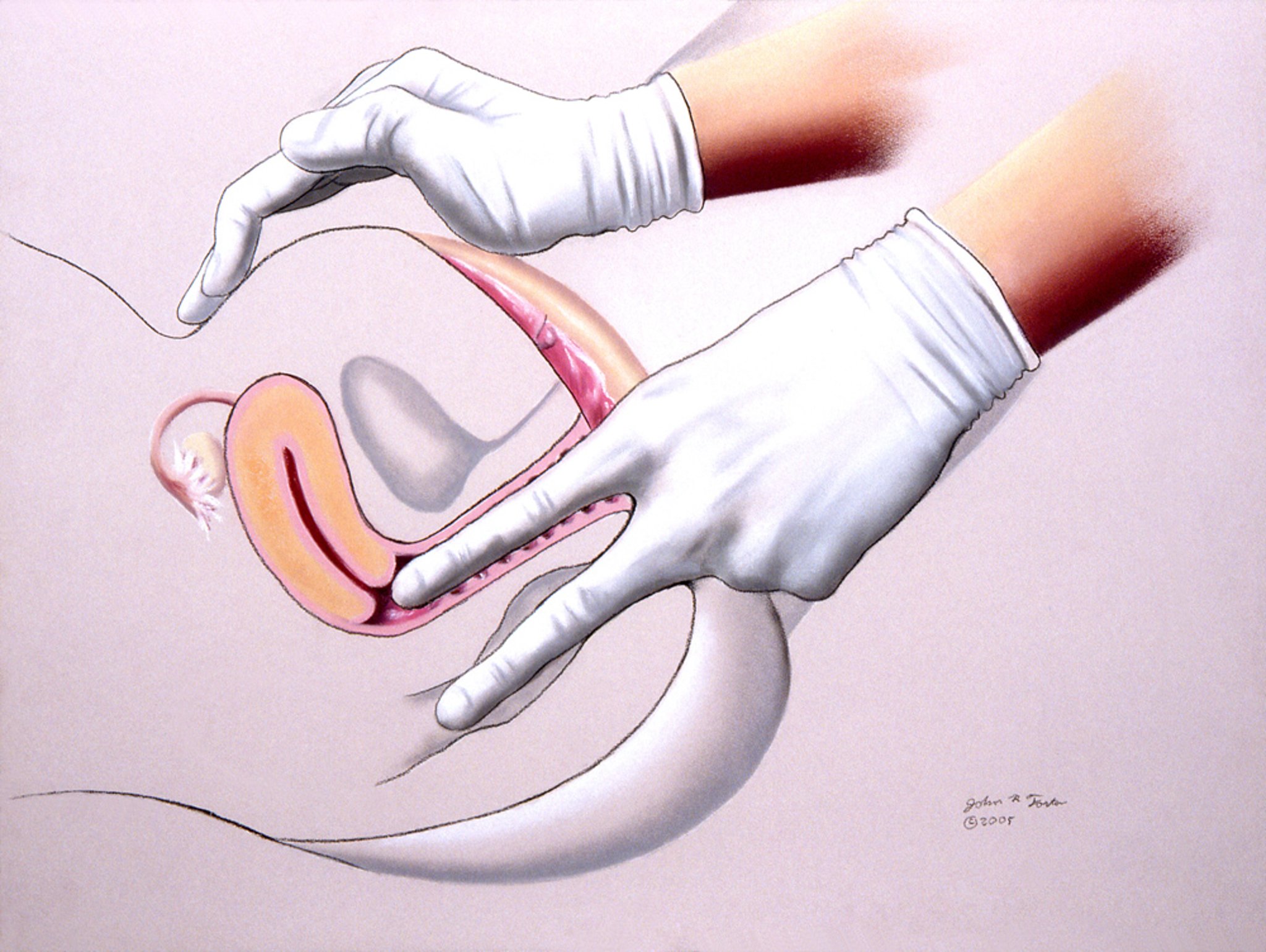
This illustration shows a pelvic examination being performed by a health care professional.
JOHN FOSTER/SCIENCE PHOTO LIBRARY
For the examination, the clinician first inspects the external genital area and notes any abnormalities, discoloration, discharge, or inflammation. This examination may detect no abnormalities or may give clues to hormonal issues, cancer, infections, injury, or sexual abuse.
The clinician spreads the tissues around the opening of the vagina (called the vulva, or labia minora) and examines the opening. Using a speculum (a metal or plastic instrument that holds open the walls of the vagina), the clinician examines the vagina and the cervix (the lower part of the uterus).
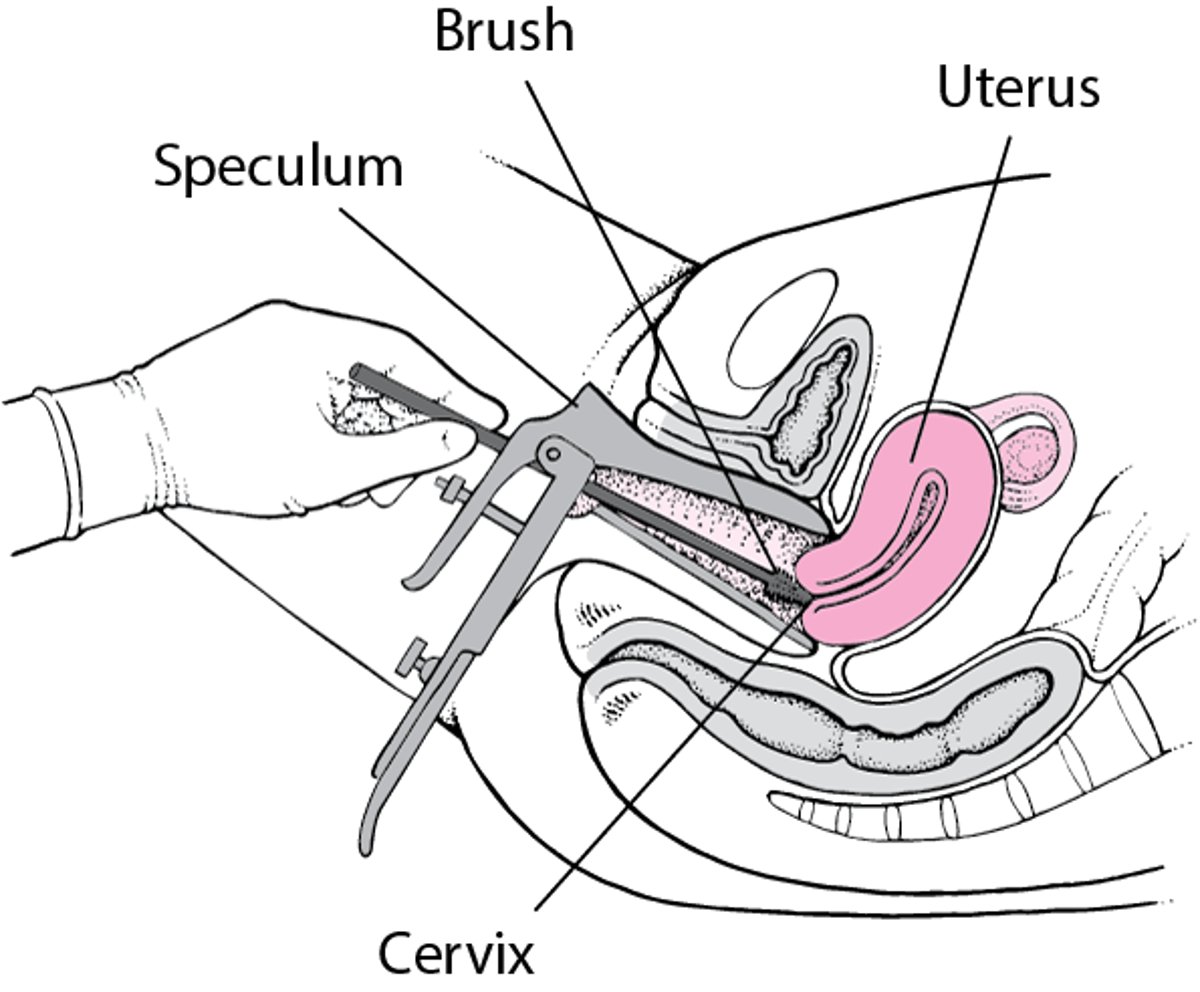
The vagina is examined for abnormalities (such as cysts) and discharge. The cervix is examined closely for signs of inflammation, abnormalities, or cervical cancer. The clinician may use a small plastic brush to obtain a sample for testing, usually a Papanicolaou (Pap) test and/or HPV testing (to screen for cervical cancer). A sample may be taken from the vagina or cervix to be tested for causes of vaginitis, such as bacterial vaginosis, vaginal yeast infection, or sexually transmitted infections.
The clinician asks the woman to cough or bear down to check for pelvic organ prolapse , which is protrusion of the bladder, rectum, or intestine into the vagina.
Pap Test
Doctors use a speculum (a metal or plastic instrument) to hold open the walls of the vagina. Then they insert a small plastic brush to obtain a sample from the cervix (the lower part of the uterus) for testing. |

After removing the speculum from the vagina, the clinician inserts the index and middle fingers of one gloved hand into the vagina and feels the vaginal walls for any abnormalities or tender areas. The clinician also feels the cervix for any abnormalities or tenderness that could not be detected during the speculum examination.

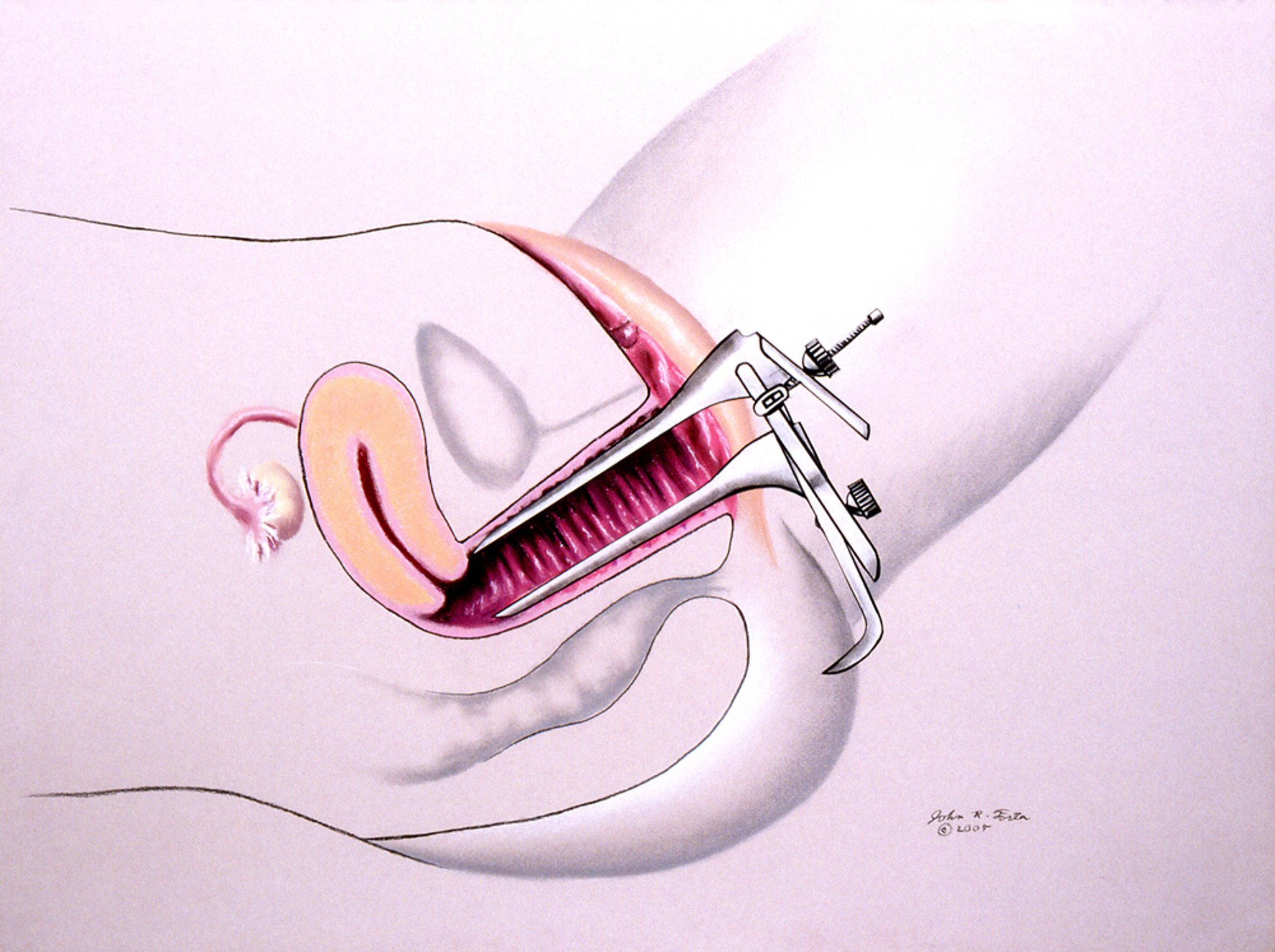
This illustration shows a pelvic examination with a speculum.
JOHN FOSTER/SCIENCE PHOTO LIBRARY
With the fingers still in the vagina, the clinician then places the fingers of the other hand on the lower abdomen above the pubic bone (called a bimanual examination). The examination is to feel the uterus and ovaries and any abnormal mass or tenderness of the female reproductive system. Between the two hands, the uterus can usually be felt as a pear-shaped, smooth, firm structure, and its position, size, consistency, mobility, and degree of tenderness (if any) can be determined.
Then the clinician attempts to feel the ovaries and other structures around the uterus (such as a swollen fallopian tube) by moving the hand on the abdomen more to the side and exerting slightly more pressure. More pressure is required because the ovaries are small and much more difficult to feel than the uterus. After menopause, the ovaries become smaller (because of the decrease in hormonal function), and usually a doctor cannot feel them during a pelvic examination. A woman may find this part of the examination to be slightly uncomfortable, but it should not be painful. The clinician determines if there are any abnormalities of the ovaries and whether there is tenderness in the ovaries or other structures.

Rectovaginal examination
A combination of a rectal and vaginal examination may be done. Sometimes masses or abnormalities in the posterior part of the pelvis (the part toward the spine) or in the tissue between the vagina and rectum can only be detected with this type of examination. The clinician inserts the index finger into the vagina and the middle finger into the rectum.
In addition, the clinician can examine the rectum for hemorrhoids, fissures, polyps, and lumps. A small sample of stool can be obtained with a gloved finger and tested for unseen (occult) blood. A woman may be given a take-home kit to test for occult blood in the stool.

This illustration shows a pelvic rectovaginal examination being performed by a health care professional.
JOHN FOSTER/SCIENCE PHOTO LIBRARY





