

Tumors rarely affect joints, unless by direct extension of an adjacent bone or soft tissue tumor. However, 2 conditions—synovial chondromatosis and tenosynovial giant cell tumor (formerly referred to as pigmented villonodular synovitis)—occur in the lining (synovium) of joints and are known as synovial proliferative disorders. These conditions are benign but locally aggressive. These conditions usually affect one joint, most often the knee and hip, and can cause pain and effusion. Both are treated by open synovectomy and, for synovial chondromatosis, removal of any intra-articular bodies and metaplastic synovium.
There is a malignant soft tissue tumor called synovial sarcoma that arises in different types of soft tissue but is not of synovial origin and seldom occurs inside of a joint. The term introduced many years ago to characterize the tumor ("synovial") is a misnomer.
Synovial chondromatosis
Synovial chondromatosis (previously called synovial osteochondromatosis) is considered metaplastic synovium. It is characterized by numerous calcified cartilaginous bodies in the synovium, which often continue to grow slowly over time and may become loose. Each body may be no larger than a grain of rice, in a swollen, painful joint. Malignant change, although very rare, can occur. Recurrence is common and is typically treated with repeat surgery.
Diagnosis of synovial chondromatosis is by imaging, with MRI being the preferred modality because it is more sensitive at detecting the smaller loose bodies. Larger loose bodies can be detected by CT or even radiographs as they ossify.


This radiograph of the knee shows multiple large calcified joint bodies both in front of and in back of the joint (arrows), which is typical of synovial chondromatosis.
Image courtesy of Michael J. Joyce, MD, and Hakan Ilaslan, MD.
Treatment of synovial chondromatosis may be symptomatic, but if mechanical symptoms are prominent, arthroscopic or open removal of the bodies or synovium is indicated.
Tenosynovial giant cell tumor
Tenosynovial giant cell tumor (previously called pigmented villonodular synovitis and giant cell tumor of tendon sheath) is considered a benign neoplastic tumor of the synovium that can occur both in tendon sheaths and in a joint. The tumor may be nodular (localized) or diffuse. The synovium becomes thickened and contains hemosiderin, which gives the tissue its blood-stained appearance and characteristic appearance on MRI. This tissue has the potential to invade adjacent bone, causing cystic destruction and damage to the cartilage. Thus, in addition to causing painful effusions, the blood products in the effusion are toxic to native cartilage and may lead to early secondary arthritis. Tenosynovial giant cell tumor is usually monarticular but may be polyarticular.
The tumors arise from neoplastic synovial cells that overexpress a growth factor CSF-1 (colony stimulating factor-1). The tumors are typically composed of a small number of these cells and a high percentage of myeloid precursors (monocytes and macrophages) that have CSF-1 receptors (CSF-1R). The CSF-1 stimulates the growth of these myeloid precursor cells.
Diffuse tenosynovial giant cell tumor has a high local recurrence rate that often leads to further surgery and morbidity. The standard treatment is complete removal by synovectomy. Smaller lesions of an accessible joint may be treated with arthroscopic resection. Open arthrotomy is usually necessary for a more complete resection. The tumor may lie both within and outside the capsule of the joint, especially when involving the popliteal space. Recurrent disease is treated with repeat excision if possible, consideration of radiotherapy, and systemic treatment options.
Pexidartinib, an oral medication, is used to treat symptomatic tenosynovial giant cell tumor causing severe morbidity or functional limitations that is not amenable to improvement by surgery. By binding to the CSF-1R expressed on monocytes, macrophages, and osteoclasts, the medication helps to prevent tumor proliferation. Adverse effects include hepatitis and liver failure. The role of Pexidartinib, an oral medication, is used to treat symptomatic tenosynovial giant cell tumor causing severe morbidity or functional limitations that is not amenable to improvement by surgery. By binding to the CSF-1R expressed on monocytes, macrophages, and osteoclasts, the medication helps to prevent tumor proliferation. Adverse effects include hepatitis and liver failure. The role ofpexidartinib is evolving, but is typically reserved for unresectable or recurrent disease (1). In the United States, the prescribing information includes a boxed warning about the risk of serious and potentially fatal liver injury. Pexidartinib is available in the United States only in cancer centers through the manufacturer's Risk Evaluation and Mitigation Strategy program.

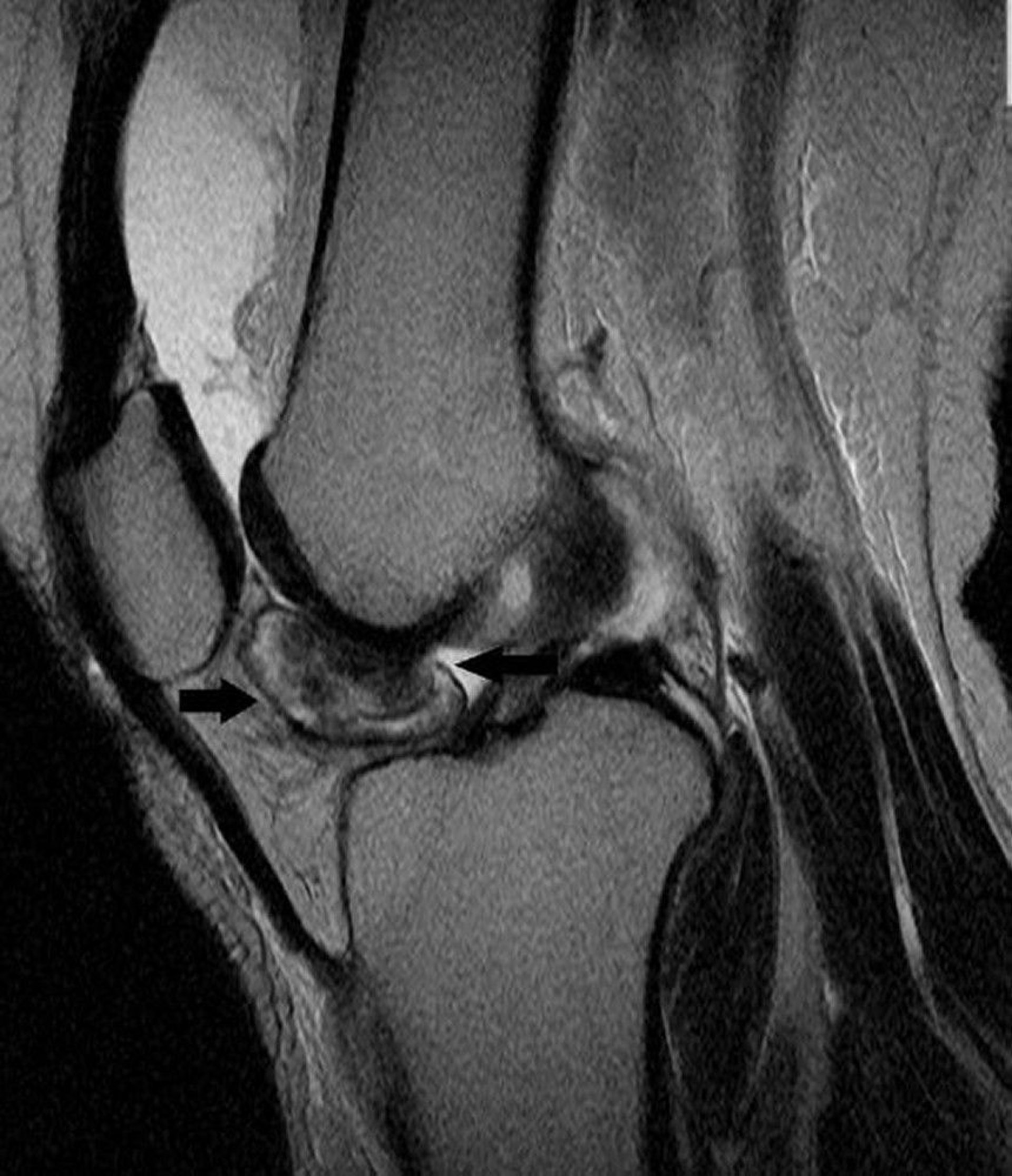
This MRI of the knee shows tenosynovial giant cell tumor in the lining of knee joint (arrows).
Image courtesy of Michael J. Joyce, MD, and Hakan Ilaslan, MD.
Reference
1. Gelderblom H, Wagner AJ, Tap WD, et al: Long-term outcomes of pexidartinib in tenosynovial giant cell tumors. Cancer. 15;127(6):884-893, 2021. doi: 10.1002/cncr.33312. Epub 2020 Nov 16. PMID: 33197285; PMCID: PMC7946703.
Drug Information for the Topic





