

Ankle sprains are very common, most often resulting from turning the foot inward (inversion). Common findings are pain, swelling, and tenderness, which are maximal at the anterolateral ankle. Diagnosis is by clinical evaluation and sometimes radiographs. Treatment is protection, rest, ice, compression, and elevation (PRICE) and early weight bearing for mild sprains and immobilization followed by physical therapy for moderate and severe sprains; some very severe sprains require surgical repair.
(See also Overview of Sprains and Other Soft-Tissue Injuries.)
The most important ankle ligaments are the following:
Deltoid (the strong, medial ligament)
Anterior and posterior talofibular (lateral ligaments)
Calcaneofibular (lateral ligaments—see figure )
Ligaments of the Ankle

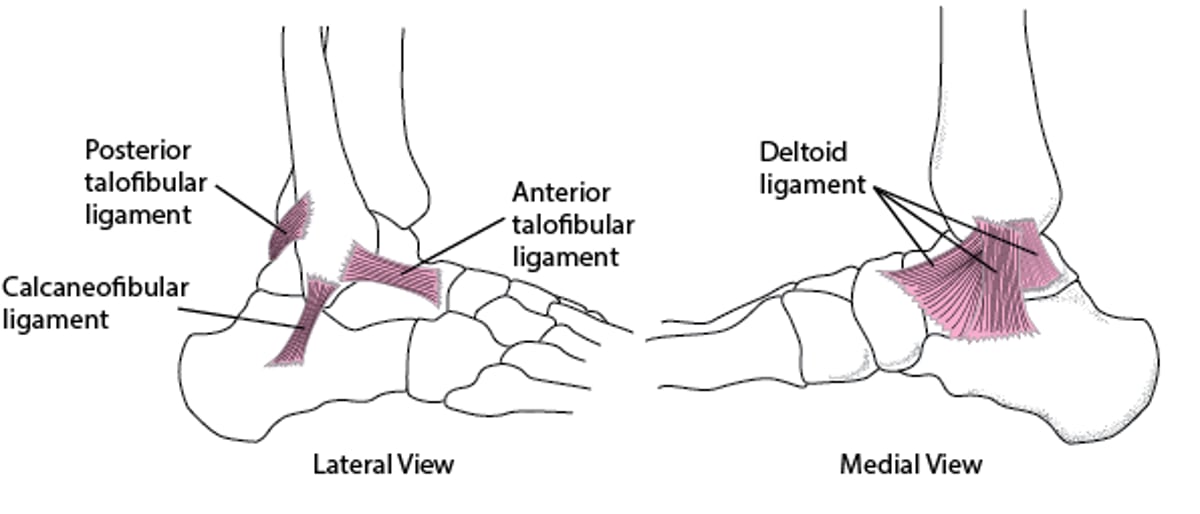
Inversion (turning the foot inward) tears the lateral ligaments, usually beginning with the anterior talofibular ligament. Most tears result from inversion. Severe 2nd- and 3rd-degree sprains sometimes cause chronic joint instability and predispose to additional sprains. Inversion can also cause talar dome fractures, with or without an ankle sprain.
Eversion (turning the foot outward) stresses the joint medially. This stress often causes an avulsion fracture of the medial malleolus rather than a ligament sprain because the deltoid ligament is so strong. However, eversion can also cause a sprain. Eversion also compresses the joint laterally; this compression, often combined with dorsiflexion, may fracture the distal fibula or tear the syndesmotic ligaments between the tibia and fibula just proximal to the ankle (called a high ankle sprain). Sometimes eversion forces are transmitted up the fibula, fracturing the fibular head just below the knee (called a Maisonneuve fracture).
Recurrent ankle sprains can damage ankle proprioception and thus predispose to future ankle sprains. Most ankle sprains are mild (1st- or 2nd-degree).


Symptoms and Signs of Ankle Sprains
Ankle sprains cause pain, swelling, and sometimes muscle spasms. The location of pain and swelling varies with the type of injury:
Inversion sprains: Usually maximal at the anterolateral ankle
Eversion injuries: Maximal over the deltoid ligament
Maisonneuve fracture: Over the proximal fibula as well as the medial and sometimes lateral ankle
Third-degree sprains (complete tears, often involving both medial and lateral ligaments): Often diffuse (sometimes the ankle appears egg-shaped)
Generally, tenderness is maximal over the damaged ligaments rather than over the bone; tenderness that is greater over bone than over ligaments suggests fracture.
In mild (1st-degree) ankle sprains, the pain and swelling are minimal, but the ankle is weakened and prone to reinjury. Healing takes hours to days.
In moderate to severe (2nd-degree) ankle sprains, the ankle is often swollen and bruised; walking is painful and difficult. Healing takes days to weeks.
In very severe (3rd-degree) ankle sprains, the whole ankle may be swollen and bruised. The ankle is unstable and cannot bear weight. Nerves may also be damaged. Articular cartilage may be torn, resulting in long-term pain, swelling, joint instability, early arthritis, and occasionally gait abnormalities. Healing of very severe ankle sprains usually takes 6 to 8 weeks.
Diagnosis of Ankle Sprains
Primarily history and physical examination
Sometimes radiographs to exclude fractures
Rarely MRI
Diagnosis of ankle sprains is primarily clinical; not every patient requires radiographs.
Stress testing to evaluate ligament integrity is important. However, if patients have marked pain and swelling or spasm, the examination is typically delayed until radiographs exclude fractures. Also, swelling and spasm may make joint stability difficult to evaluate; thus, reexamination after several days is helpful. The ankle may be immobilized until examination is possible.
The ankle anterior drawer test is performed to evaluate the stability of the anterior talofibular ligament and thus help differentiate between 2nd- and 3rd-degree lateral ligament sprains. For this test, patients sit or lie supine with the knee at least slightly flexed; one of the clinician's hands prevents forward movement of the anterior distal tibia while the other hand cups the heel, pulling it anteriorly. Forward movement of the foot indicates a 3rd-degree tear.
High ankle sprains injuring the anterior inferior tibiofibular and posterior inferior tibiofibular ligaments and the interosseous membrane should be considered when eversion is the mechanism and when eversion reproduces pain; the distal tibiofibular joint, just proximal to the talar dome, may be tender.


If the ankle is stable, the intra-articular surfaces of the talus and tibia should be parallel. Here, they are widely misaligned, indicating gross joint instability. Instability would have been clearly evident clinically, and instability is normally assessed clinically without need for radiographs.
ZEPHYR/SCIENCE PHOTO LIBRARY
If findings suggest a deltoid ligament or high ankle sprain, clinicians should check for evidence of a proximal fibular fracture.
Ankle sprains should be differentiated from avulsion fractures of the base of the 5th metatarsal, Achilles tendon injuries, and talar dome fractures, which may cause similar symptoms.
Imaging
Anteroposterior, lateral, and oblique (mortise) ankle radiographs are taken to exclude clinically significant fractures. Clinical criteria (Ottawa ankle and foot rules [1]) are used to determine whether radiographs are needed; these criteria are used to help limit radiographs to patients more likely to have a fracture that requires specific treatment.
Ottawa ankle rules
An ankle radiograph is recommended only if patients have ankle pain and one of the following:
Inability to bear weight without assistance immediately after the injury AND in the emergency department (for 4 steps), with or without limping
Bone tenderness within 6 cm of the posterior edge or tip of either malleolus
If ankle radiographs show a widened mortise, proximal tibia/fibula radiographs should be obtained to evaluate for a Maisonneuve fracture.
Ottawa foot rules
A foot radiograph is recommended only if patients have midfoot pain and one of the following:
Inability to bear weight without assistance immediately after the injury AND in the emergency department (for 4 steps), with or without limping
Bone tenderness at the navicular
Bone tenderness at the base of the 5th metatarsal
Patients with unreliable sensory findings (eg, with neuropathy, or who are intoxicated) may require radiographs regardless of the Ottawa rules. The Ottawa rules should only be applied to patients ≥ 2 years old. The need for radiographs for children < 2 years old is based on clinician discretion.
Sprains that are painful after 6 weeks may require additional testing (eg, MRI) to identify overlooked and subtle injuries, such as talar dome fractures, high ankle sprains, or other complex ankle sprains.
Diagnosis reference
1. Stiell IG, Greenberg GH, McKnight RD, et al. Decision rules for the use of radiography in acute ankle injuries. Refinement and prospective validation. JAMA. 1993;269(9):1127-1132. doi:10.1001/jama.269.9.1127
Treatment of Ankle Sprains
PRICE (protection, rest, ice, compression, and elevation) and early mobilization for mild sprains
Immobilization and/or surgical repair for moderate or severe sprains
Most ankle sprains heal well with minimal intervention and early mobilization. Splinting alleviates pain but does not appear to affect final outcome.


Other treatment depends on severity of the sprain:
Mild (eg, 1st-degree) sprains: PRICE and weight bearing and mobilization as soon as it can be tolerated (usually within a few days)
Moderate (eg, 2nd-degree) sprains: PRICE, including immobilization of the ankle in a neutral position with a posterior splint or a commercially available boot, followed by mobilization and physical therapy
Severe (eg, 3rd-degree) sprains: Immobilization (possibly with a cast), possibly surgical repair, and physical therapy
High ankle sprains usually require a cast for several weeks.
Key Points
Before diagnosing an ankle sprain, consider an avulsion fracture of the base of the 5th metatarsal, an Achilles tendon injury, or a talar dome fracture.
Use the Ottawa ankle and foot rules to help decide whether radiographs are necessary.
Evaluate joint stability by stress testing (eg, anterior drawer test), but if needed, delay this testing until swelling and pain subside.
Encourage early mobilization if the sprain is mild.





