

In Wolff-Parkinson-White syndrome, antegrade conduction occurs over an accessory pathway. If atrial fibrillation, develops this is a medical emergency because very rapid ventricular rates can develop.
(See also Overview of Arrhythmias and Atrial Fibrillation.)
In manifest Wolff-Parkinson-White (WPW) syndrome, antegrade conduction occurs over the accessory pathway. If atrial fibrillation develops, the normal rate-limiting effects of the atrioventricular (AV) node are bypassed, and the resultant excessive ventricular rates (sometimes 200 to 300 beats/minutes) may lead to ventricular fibrillation (see figure ) and sudden death (1).
Patients with an accessory AV connection that does not conduct in the antegrade direction do not have the short PR interval and delta wave characteristic of WPW syndrome (concealed WPW syndrome). However, they may still have orthodromic reciprocating atrioventricular supraventricular tachycardia, in which the accessory AV connection is used in the retrograde direction, but they are not at risk of rapid conduction of atrial fibrillation, in which the accessory AV connection is used in the antegrade direction).
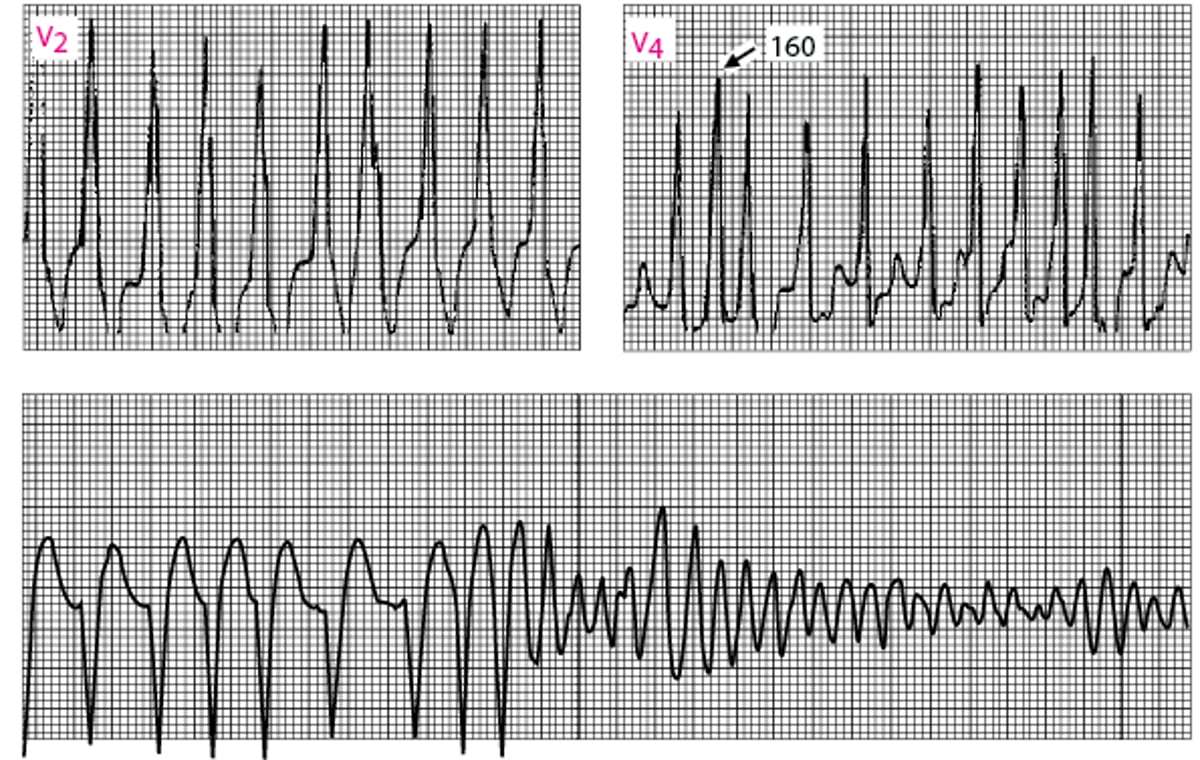
Atrial Fibrillation in Wolff-Parkinson-White Syndrome
Ventricular response is very fast (RR intervals minimum of 160 msec). Shortly thereafter, ventricular fibrillation develops (lead II continuous rhythm strip at bottom). |

General reference
1. Klein GJ, Bashore TM, Sellers TD, et al: Ventricular fibrillation in the Wolff-Parkinson-White syndrome. N Engl J Med 301(20):1080–1085, 1979. doi: 10.1056/NEJM197911153012003
Treatment of Atrial Fibrillation and WPW Syndrome
Direct-current cardioversion
The treatment of choice for Wolff-Parkinson-White syndrome with atrial fibrillation is direct current cardioversion (1). The usual rate-slowing medications used in atrial fibrillation are not effective, and digoxin, adenosine, and the nondihydropyridine calcium channel blockers (eg, verapamil, diltiazem) that may be used in many other forms of supraventricular tachycardia are contraindicated because they may increase the ventricular rate and cause ventricular fibrillation. ). The usual rate-slowing medications used in atrial fibrillation are not effective, and digoxin, adenosine, and the nondihydropyridine calcium channel blockers (eg, verapamil, diltiazem) that may be used in many other forms of supraventricular tachycardia are contraindicated because they may increase the ventricular rate and cause ventricular fibrillation.
If cardioversion is impossible, medications that prolong the refractory period of the accessory connection should be used. IV procainamide or ibutilide is preferred (If cardioversion is impossible, medications that prolong the refractory period of the accessory connection should be used. IV procainamide or ibutilide is preferred (1), but any class Ia, class Ic, or class III antiarrhythmic medication can be used.
Pearls & Pitfalls
|
Treatment reference
1. Joglar JA, Chung MK, Armbruster AL, et al: 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 149(1):e1–e156, 2024. doi: 10.1161/CIR.0000000000001193





