

Human African trypanosomiasis is an infection with protozoa of the species Trypanosoma brucei, transmitted by the bite of a tsetse fly. Symptoms include characteristic skin lesions, intermittent fever, headache, rigors, transient edema, generalized lymphadenopathy, and often fatal meningoencephalitis. Diagnosis is made by identification of the organism in blood, lymph node aspirate, or cerebrospinal fluid or sometimes by serologic tests. Treatment is with fexinidazole, suramin, pentamidine, melarsoprol, or eflornithine, depending on the infecting subspecies, clinical stage, and drug availability., transmitted by the bite of a tsetse fly. Symptoms include characteristic skin lesions, intermittent fever, headache, rigors, transient edema, generalized lymphadenopathy, and often fatal meningoencephalitis. Diagnosis is made by identification of the organism in blood, lymph node aspirate, or cerebrospinal fluid or sometimes by serologic tests. Treatment is with fexinidazole, suramin, pentamidine, melarsoprol, or eflornithine, depending on the infecting subspecies, clinical stage, and drug availability.
There are 2 forms of human African trypanosomiasis (sleeping sickness). West African sleeping sickness is caused by Trypanosoma brucei gambiense in West and Central Africa. East African sleeping sickness is caused by T. brucei rhodesiense in eastern and southern areas of Africa. Both species are endemic in Uganda. T. brucei gambiense accounts for > 97% of all cases of African trypanosomiasis, and T. brucei rhodesiense accounts for approximately 3% (1).
African trypanosomiasis has been targeted for eradication by the World Health Organization (WHO), and, as a result of control efforts, there has been a dramatic decrease (> 95%) in the number of reported cases worldwide. In 2023, approximately 675 combined cases were reported to the WHO, with over 90% caused by T. b. gambiense (1). On average, 1 case is diagnosed in the United States each year, always in a traveler returning to the United States from an endemic region (2).
Humans are the main reservoir of T. b. gambiense, but this species may also reside in animals. Wild game animals are the main reservoirs of T. b. rhodesiense, followed by domestic livestock (3). The organisms are transmitted by tsetse flies and can be transmitted transplacentally from mother to fetus (4). Rarely, trypanosomiasis can be transmitted through blood transfusions; theoretically, it could also be transmitted through organ transplantation.
Another trypanosomal species, Trypanosoma cruzi, is endemic in South and Central America and causes Chagas disease (American trypanosomiasis).
General references
1. World Health Organization (WHO): Human African trypanosomiasis (sleeping sickness). Accessed February 10, 2025.
2. Centers for Disease Control and Prevention (CDC): Trypanosomiasis, African. CDC Yellow Book 2024.
3. Chimelli L, Scaravilli F. Trypanosomiasis. Brain Pathol. 1997;7(1):599-611. doi:10.1111/j.1750-3639.1997.tb01077.x
4. Traub N, Hira PR, Chintu C, Mhango C. Congenital trypanosomiasis: report of a case due to Trypanosoma brucei rhodesiense. East Afr Med J. 1978;55(10):477.
Pathophysiology of African Trypanosomiasis
The life cycle of T. b. gambiense involves both the tsetse fly and human host. The tsetse fly becomes infected by feeding on the blood of an infected mammal. The life cycle begins when an infected tsetse fly (genus Glossina) bites a human and injects metacyclic trypanosome parasites into the bloodstream. Metacyclic trypomastigotes then transform into bloodstream trypomastigotes, which multiply by binary fission and spread through the lymphatics and bloodstream after inoculation. Bloodstream trypomastigotes multiply until specific antibodies produced by the host sharply reduce parasite levels. However, a subset of parasites can escape immune destruction by a change in their variant surface glycoprotein and start a new multiplication cycle. The cycle of multiplication and lysis then repeats. The life cycle continues when a tsetse fly bites an infected human or animal. (See also Trypanosomiasis in Animals.)
Late in the course of African trypanosomiasis, trypanosomes appear in the interstitial fluid of many organs, including the myocardium and eventually the central nervous system.

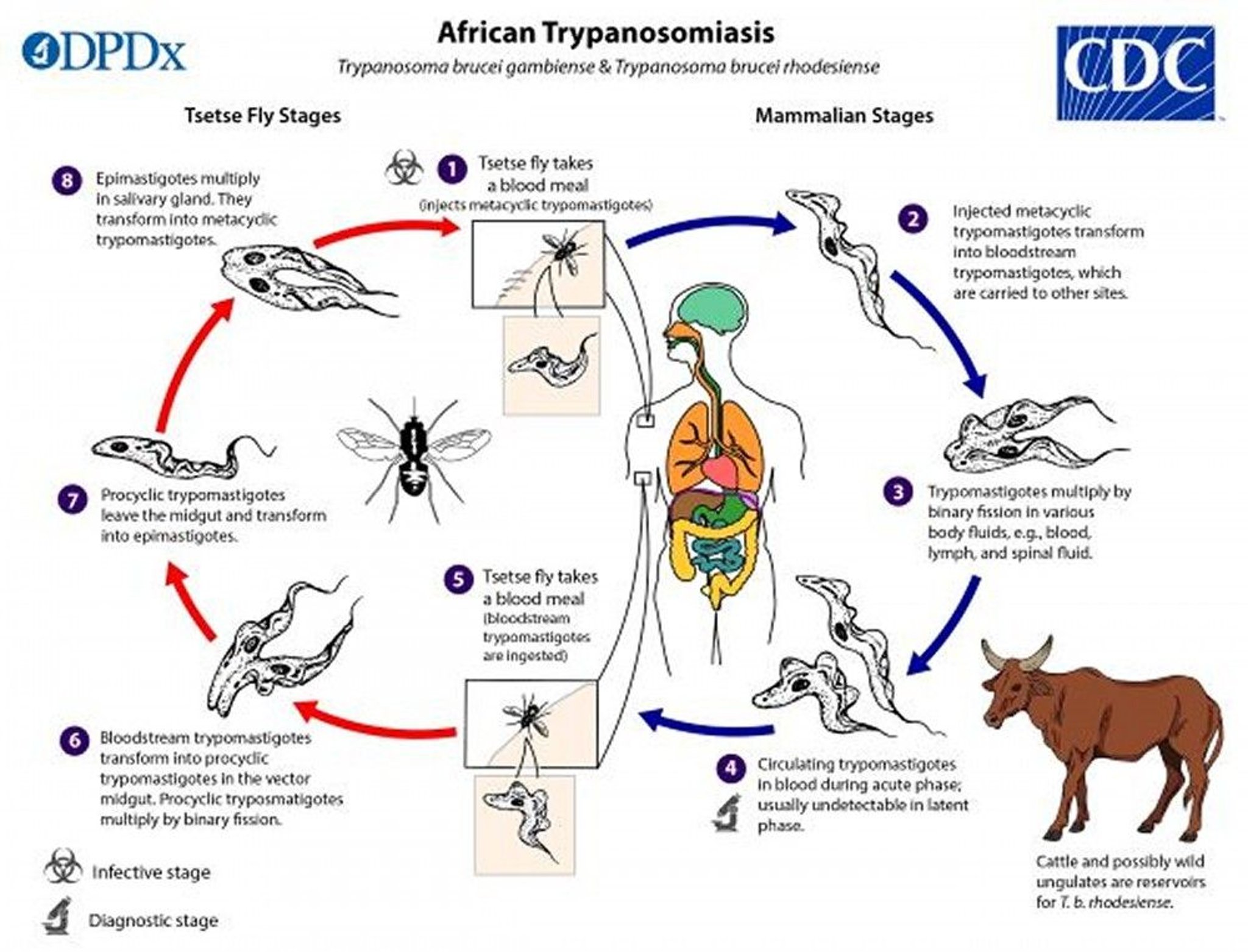
1. During a blood meal on a mammalian host, an infected tsetse fly injects metacyclic trypomastigotes into skin tissue. The parasites enter the lymphatic system and pass into the bloodstream.
2. Inside the host, they transform into bloodstream trypomastigotes, are carried to other sites throughout the body, and enter other body fluids (eg, lymph, spinal fluid).
3. The trypomastigotes multiply by binary fission.
4. They circulate in the bloodstream.
5. During a blood meal from an infected mammalian host, a tsetse fly becomes infected with bloodstream trypomastigotes.
6. In the fly's midgut, the parasites transform into procyclic trypomastigotes and multiply by binary fission.
7. The procyclic trypomastigotes leave the midgut and transform into epimastigotes.
8. The epimastigotes reach the fly's salivary glands, multiply by binary fission, and develop into metacyclic trypomastigotes.
Image from the Centers for Disease Control and Prevention, Global Health, Division of Parasitic Diseases and Malaria.
Symptoms and Signs of African Trypanosomiasis
African trypanosomiasis has 3 stages:
Cutaneous
Hemolymphatic
Central nervous system
Cutaneous
A papule may develop at the site of the tsetse fly bite within a few days to 2 weeks. It evolves into a red, painful, indurated nodule that may ulcerate (trypanosomal chancre).


This photo shows a tender, well-circumscribed, and indurated nodule on a person's leg, marking the site of the initial bite of the Glossina fly, the vector for human African trypanosomiasis infection.
Hemolymphatic
Intermittent fever, headaches, rigors, muscle and joint pain, and transient facial swelling develop over several months in T. b. gambiense infection but over a period of weeks in T. b. rhodesiense infection. An evanescent, circinate, erythematous rash may develop. It is most readily visible in people with light skin. Generalized lymphadenopathy often occurs.
Lymphadenopathy in the posterior cervical triangle (Winterbottom sign) is characteristic of trypanosomiasis caused by T. b. gambiense. Anemia may occur during any stage of infection because the parasites themselves can disrupt production and hasten lysis of red blood cells.
Central nervous system
In T. b. gambiense infection, central nervous system (CNS) involvement occurs months to several years after the onset of acute disease.
In T. b. rhodesiense infection, disease is more fulminant, and CNS invasion often occurs within a few weeks.
CNS involvement can result in persistent headache, inability to concentrate, personality changes (eg, progressive lassitude and indifference), daytime somnolence, tremor, ataxia, and in terminal stages, coma.
Without treatment, death can occur within months of infection with T. b. rhodesiense and during the second or third year of infection with T. b. gambiense. Untreated patients may die of complications such as coma, which often results from severe undernutrition or secondary infections.
Clinical suspicion for severe disease (also called the severe meningo-encephalitic stage) is raised when the patient exhibits the following neurologic symptoms indicating significant cognitive and motor dysfunction:
Mental confusion
Abnormal behavior
Logorrhea (excessive uncontrollable or incoherent speech)
Anxiety
Ataxia
Tremors
Motor weakness
Speech impairment
Abnormal gait
Uncontrollable movements
Seizures
Diagnosis of African Trypanosomiasis
Light microscopy of blood (thin or thick smears) or other fluid sample for all subspecies of T. brucei
Serologic tests for T. b. gambiense
Other supportive laboratory tests (complete blood count, serum immunoglobulin levels)
The diagnosis of T. b. gambiense human African trypanosomiasis (HAT) is often by serologic screening followed by parasitologic confirmation. Serologic tests include lateral flow rapid tests and a card agglutination test that is useful in mass screening programs. For parasitologic confirmation, specimens of lymph, blood, or both are examined microscopically. Wet preparations contain motile trypanosomes, and smears can also be fixed, stained with Giemsa (or Field) before examination. The number of trypanosomes in blood is often low in T. b. gambiense infection, and concentration techniques (eg, microhematocrit centrifugation, miniature anion-exchange centrifugation, quantitative buffy coat technique) enhance sensitivity.
Antibody detection is less useful for T. b. rhodesiense, which progresses rapidly, often before a strong antibody response develops. Diagnosis therefore relies on light microscopic detection of parasites in blood or cerebrospinal fluid (CSF). If a chancre is present, trypanosomes can be detected using chancre aspirate. T. b. rhodesiense typically has higher trypanosome density in blood, which makes concentration techniques that are performed before microscopic examination less important.
For both forms of HAT, the disease stage is determined by examination of CSF. Disease stage influences treatment decisions for patients < 6 years old, those weighing < 20 kg, and for those with clinical features suggestive of severe disease; a lumbar puncture should be performed in these groups.
Patients without neurologic symptoms are considered to have a low probability of being in the severe meningo-encephalitic stage and do not require a lumbar puncture for treatment guidance.
Patients with symptoms and signs of severe disease should be evaluated by lumbar puncture and CSF examination. This step is crucial because the choice of treatment depends on whether the central nervous system (CNS) is involved. Laboratory diagnosis of severe disease is made according to the following parameters:
For T. b. gambiense HAT, white blood cell count ≥ 100 cells/mcL (≥ 0.1 × 109/L) in CSF with or without trypanosomes in CSF
For T. b. rhodesiense HAT, white blood cell count > 5 cells/mcL (> 0.005 × 109/L) or trypanosomes in CSF
Other, nonspecific laboratory findings include anemia, monocytosis, and markedly elevated serum levels of polyclonal IgM.
Treatment of African Trypanosomiasis
For T. b. gambiense human African trypanosomiasis (HAT): Oral fexinidazole for patients aged ≥ 6 years and body weight ≥ 20 kg presenting without clinical features of severe disease; sometimes IM pentamidine or oral nifurtimox/IV eflornithine combination therapyhuman African trypanosomiasis (HAT): Oral fexinidazole for patients aged ≥ 6 years and body weight ≥ 20 kg presenting without clinical features of severe disease; sometimes IM pentamidine or oral nifurtimox/IV eflornithine combination therapy
For T. b. rhodesiense HAT: Oral fexinidazole for patients aged ≥ 6 years and body weight ≥ 20 kg presenting without clinical features of severe disease; sometimes IV suramin, IV melarsoprol, or IM pentamidineHAT: Oral fexinidazole for patients aged ≥ 6 years and body weight ≥ 20 kg presenting without clinical features of severe disease; sometimes IV suramin, IV melarsoprol, or IM pentamidine
The treatment of HAT is guided by the pathologic species, stage of disease, patient age and weight, and drug availability. See table for medications.
Patients with severe disease who cannot be evaluated by lumbar puncture or who cannot be treated with fexinidazole (ie, age < 6 years or body weight < 20 kg) should be treated as outlined below.
Alternative regimens have been proposed for debilitated patients with severe CNS (meningoencephalitic) involvement. Serial follow-up examinations, including CSF analysis, are recommended every 6 months (sooner if symptoms return) for 2 years.
Corticosteroids have been used to decrease the risk of CNS inflammation (ie, encephalopathic reactions).
There is no test of cure. After treatment, patients should be monitored for relapse for 24 months. Recurrence of symptoms necessitates re-examination of CSF for parasites.
Treatment of Human African Trypanosomiasis (HAT)
Patient Age and Body Weight | LP/CSF Examination and First-Line Medication* | Second-Line Medication* | Adverse Effects | Comments | |
|---|---|---|---|---|---|
Trypanosoma brucei gambiense HAT | |||||
< 6 years or < 20 kg | If WBC count ≤ 5 cells/mcL (≤ 0.005 × 109/L) and no trypanosomes: Pentamidine/L) and no trypanosomes: Pentamidine | — | Pentamidine: Dizziness, nausea, vomiting, and pain at injection sitePentamidine: Dizziness, nausea, vomiting, and pain at injection site | Pentamidine can be given IM.Pentamidine can be given IM. | |
If WBC count > 5 cells/mcL (> 0.005 × 109/L), or trypanosomes: Oral nifurtimox/IV eflornithine combination therapy (NECT)/L), or trypanosomes: Oral nifurtimox/IV eflornithine combination therapy (NECT) | EflornithineEflornithine | Eflornithine: Fever, pruritus, hypertension, nausea, vomiting, diarrhea, abdominal pain, headaches, bone marrow suppression, and seizures Nifurtimox: Anorexia, nausea, vomiting, weight loss, polyneuropathy, headache, dizziness, and vertigo NECT: Abdominal pain, nausea, vomiting, and headache | Eflornithine is ineffective for T. b. rhodesiense HAT. Eflornithine monotherapy is given for CNS stage T. b. gambiense HAT when NECT is not feasible because nifurtimox is unavailable or contraindicated and when fexinidazole cannot be given. | ||
≥ 6 years and ≥ 20 kg | Lumbar puncture not needed if no suspicion of severe HAT: FexinidazoleLumbar puncture not needed if no suspicion of severe HAT: Fexinidazole | LP needed: Pentamidine (hemolymphatic stage) or NECT (CNS stage)†LP needed: Pentamidine (hemolymphatic stage) or NECT (CNS stage)† | Fexinidazole: Vomiting, nausea, decreased appetite, headache, insomnia, QT interval prolongation, and neutropenia | Fexinidazole is given orally.Fexinidazole is given orally. | |
Lumbar puncture needed if suspicion of severe HAT:
| WBC count < 100 cells/mcL (< 0.1 × 109/L): Pentamidine (hemolymphatic stage) or NECT (CNS stage)/L): Pentamidine (hemolymphatic stage) or NECT (CNS stage) WBC count ≥ 100 cells/mcL (≥ 0.1 × 109/L): Fexinidazole/L): Fexinidazole | — | — | ||
T. b. rhodesiense HAT | |||||
< 6 years or < 20 kg | ≤ 5 WBC/mcL and no trypanosomes: Suramin | PentamidinePentamidine | Suramin: Nausea, vomiting, photophobia, hyperesthesias, peripheral neuropathy, nephrotoxicity, urticaria, and pruritus | Suramin is given IV. Suramin is the only drug effective for the hemolymphatic stage of T. b. rhodesiense. Suramin is not used to treat T. b. gambiense because although potentially effective, it has been associated with adverse effects. Caution must be exercised when administering suramin because serious hypersensitivity reactions can occur in patients co-infected with Onchocerca volvulus, which is endemic in many areas of West Africa where T. b. gambiense occurs. | |
> 5 WBC/mcL, or trypanosomes: Melarsoprol | — | Melarsoprol: Encephalopathic reactions, exfoliative dermatitis, cardiovascular toxicity (hypertension, arrhythmia, heart failure), pruritus, and gastrointestinal and renal toxicity | IV melarsoprol, an organic arsenical, is often used in African countries because of the limited availability of eflornithine, even though adverse effects can be severe and life threatening.‡ | ||
≥ 6 years and ≥ 20 kg | LP not needed: FexinidazoleLP not needed: Fexinidazole | LP needed: Suramin or pentamidine (hemolymphatic stage) or melarsoprol (CNS stage)LP needed: Suramin or pentamidine (hemolymphatic stage) or melarsoprol (CNS stage) | — | — | |
* In the United States, pentamidine and nifurtimox are commercially available, fexinidazole is available from the manufacturer, and eflornithine, suramin, and melarsoprol can be obtained from the CDC. | |||||
† For T. b. gambiense HAT, patients with ≤ 5 WBC/mL (≤ 0.005 × 109/L) and no trypomastigotes in CSF are in the hemolymphatic stage, whereas those with > 5 WBC/mL (> 0.005 × 109/L) or trypomastigotes in CSF are in the CNS stage. | |||||
‡ Melarsoprol is only indicated for T. b. gambiense HAT for treatment of recurrent relapse after first-line and other treatment failure. Melarsoprol is only indicated for T. b. rhodesiense HAT for the following:
| |||||
CDC = Centers for Disease Control and Prevention; CNS = central nervous system; CSF = cerebrospinal fluid; LP = lumbar puncture; NECT = oral nifurtimox/IV eflornithine combination therapy; WBC = white blood cell. | |||||
Data fromWorld Health Organization: Guidelines for the treatment of human African trypanosomiasis. June 2024. | |||||
Treatment of T. b. gambiense HAT
Treatment approaches for T. b. gambiense HAT are based on the World Health Organization guidelines (1).
Patients with T. b. gambiense who are ≥ 6 years of age or weigh ≥ 20 kg who have no suspicion of severe disease do not require a lumbar puncture, and the first-line medication is oral fexinidazole. who are ≥ 6 years of age or weigh ≥ 20 kg who have no suspicion of severe disease do not require a lumbar puncture, and the first-line medication is oral fexinidazole.
However, if severe disease is suspected, a lumbar puncture is necessary. If the CSF WBC count is < 100 cells/mcL (< 0.1 × 109/L), oral fexinidazole is used. If the WBC count is ≥ 100 cells/mcL (≥ 0.1 × 109/L) or if the lumbar puncture fails, oral nifurtimox/IV eflornithine combination therapy (NECT) is the medication of choice. Adverse effects of /L) or if the lumbar puncture fails, oral nifurtimox/IV eflornithine combination therapy (NECT) is the medication of choice. Adverse effects ofeflornithine include gastrointestinal symptoms, bone marrow suppression, and seizures. Common adverse effects of nifurtimox are anorexia, nausea, vomiting, weight loss, polyneuropathy, headache, dizziness, and vertigo.
In children who are > 6 years of age or weigh > 20 kg, the approach depends on the CSF WBC count and on the presence of trypanosomes. If the WBC count is ≤ 5 cells/mcL (≤ 0.005 × 109/L) and no trypanosomes are present, the recommended medication is IM pentamidine. However, if the WBC count is > 5 cells/mcL (> 0.005 × 10/L) and no trypanosomes are present, the recommended medication is IM pentamidine. However, if the WBC count is > 5 cells/mcL (> 0.005 × 109/L) or trypanosomes are present, the recommended medication is NECT.
In the United States, pentamidine and nifurtimox are commercially available, fexinidazole is available from the manufacturer, and eflornithine can be obtained from the CDC.
Treatment of T. b. rhodesiense HAT
Treatment approaches for T. b. rhodesiense HAT are based on the World Health Organization guidelines (1).
Patients with T. b. rhodesiense who are ≥ 6 years of age or weigh ≥ 20 kg do not usually need a lumbar puncture, and the first-line medication is oral fexinidazole. If severe disease is suspected and a lumbar puncture is needed, either IV suramin or IM pentamidine is recommended. who are ≥ 6 years of age or weigh ≥ 20 kg do not usually need a lumbar puncture, and the first-line medication is oral fexinidazole. If severe disease is suspected and a lumbar puncture is needed, either IV suramin or IM pentamidine is recommended.Fexinidazole is still being evaluated for T. b. rhodesiense, and all treated patients should be evaluated clinically for relapse 1, 3, 6, and 12 months after treatment.
In children who are > 6 years of age or weigh > 20 kg, the approach also depends on the CSF WBC count and on the presence of trypanosomes. If the WBC count is ≤ 5 cells/mcL (≤ 0.005 × 109/L) and no trypanosomes are present, IV suramin is the recommended medication. If the WBC count is > 5 cells/mcL (> 0.005 × 109/L) or trypanosomes are present, IV melarsoprol is used.
Suramin is the only effective drug for the hemolymphatic stage of T. b. rhodesiense, where the benefits of therapy outweigh its risks. Suramin is not used to treat T. b. gambiense because although potentially effective, it has been associated with adverse effects, including nausea, vomiting, photophobia, hyperesthesias, peripheral neuropathy, nephrotoxicity, urticaria, and pruritus. Caution must be used when administering suramin because serious hypersensitivity reactions can occur in patients coinfected with Onchocerca volvulus, which is endemic in many areas of West Africa where T. b. gambiense occurs (2).
IV melarsoprol, an organic arsenical, is often used in African countries because of the limited availability of eflornithine, even though adverse effects can be severe and life threatening. Serious adverse effects of melarsoprol include encephalopathic reactions, exfoliative dermatitis, cardiovascular toxicity (hypertension, arrhythmia, heart failure), and gastrointestinal and renal toxicity.
In the United States, pentamidine is commercially available, fexinidazole is available from the manufacturer, and suramin and melarsoprol can be obtained from the CDC.
Treatment references
1. World Health Organization: Guidelines for the treatment of human African trypanosomiasis. June 2024.
2. Wiedemar N, Hauser DA, Mäser P. 100 Years of Suramin. Antimicrob Agents Chemother. 2020;64(3):e01168-19. Published 2020 Feb 21. doi:10.1128/AAC.01168-19
Prevention of African Trypanosomiasis
The prevention of African trypanosomiasis includes avoiding endemic areas and protecting against tsetse flies (vector control measures).
Visitors to game parks should wear substantial wrist- and ankle-length clothing (tsetse flies bite through thin clothes) in neutral colors that blend with the background and should use insect repellents, although efficacy of repellents against tsetse flies may be limited.
Surveillance in endemic areas is helpful to arrest ongoing disease transmission when resources are available.
Prophylactic medication is not advised because the risks outweigh the potential benefits.
Key Points
African trypanosomiasis is caused by Trypanosoma brucei gambiense in West and Central Africa and by T. b. rhodesiense in East Africa; tsetse flies are the main vector.
T. b. gambiense is more prevalent; T. b. rhodesiense is less frequent in humans.
There are 3 stages of disease: cutaneous, hemolymphatic, and CNS (sleeping sickness).
Diagnose using light microscopy of blood (thin or thick smears) or another fluid sample.
Treatment of African trypanosomiasis varies by species, stage of disease, and drug availability.
For nonsevere T. b. gambiense or T. b. rhodesiense infection, fexinidazole is first-line therapy for most patients.infection, fexinidazole is first-line therapy for most patients.
For severe T. b. gambiense infection, use fexinidazole or eflornithine (if available) alone or in combination with nifurtimox (NECT), and sometimes use pentamidine.or eflornithine (if available) alone or in combination with nifurtimox (NECT), and sometimes use pentamidine.
For severe T. b. rhodesiense, use suramin or pentamidine; use melarsoprol only in patients who cannot receive fexinidazole.
More Information
The following English-language resources may be useful. Please note that The Manual is not responsible for the content of these resources.
Centers for Disease Control and Prevention (CDC): Clinical Guidance for Human African Trypanosomiasis
MSD Veterinary Manual: Trypanosomiasis in Animals





