



Oral cancer refers to cancer occurring between the vermilion border of the lips and the junction of the hard and soft palates or the posterior one-third of the tongue. Over 95% of people with oral squamous cell carcinoma smoke tobacco, drink alcohol, or both. Early, curable lesions are rarely symptomatic; thus, preventing fatal disease requires early detection by screening. Treatment is with surgery, radiation, or both, although surgery plays a larger role in the treatment of most oral cavity cancer.
(See also Overview of Head and Neck Tumors.)
Oral squamous cell carcinoma affects about 35,000 people in the United States each year (1). In the United States, 3% of cancers in males and 2% in females are oral squamous cell carcinomas, most of which occur after age 50 years. As with most head and neck sites, squamous cell carcinoma is the most common oral cancer.
The chief risk factors for oral squamous cell carcinoma are
Smoking (especially > 2 packs/day)
Alcohol use
Risk increases dramatically when alcohol use exceeds 177 mL (6 oz) of distilled liquor, 148 mL (5 oz) of wine, or 1065 mL (36 oz) of beer/day. The combination of heavy smoking and heavy alcohol consumption is estimated to raise the risk 100-fold in females and 38-fold in males.
Squamous cell carcinoma of the tongue may also result from any chronic irritation, such as dental caries, overuse of mouthwash, chewing tobacco, or the use of betel quid. Oral human papillomavirus (HPV), typically acquired via oral-genital contact, may have a role in the etiology of some oral cancers; however, HPV is identified in oral cancer much less often than it is in oropharyngeal cancer, and its presence in resected tissue does not necessarily imply causation.
Oral cancer refers to cancer occurring between the vermilion border of the lips and the junction of the hard and soft palates or the posterior one-third of the tongue. Intraoral squamous cell carcinomas may begin on the floor of the mouth or on the lateral and ventral surfaces of the tongue. Oral squamous cell carcinomas that occur on the lower lip are usually solar-related cancers on the external surface.
General reference
1. Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024 [published correction appears in CA Cancer J Clin. 2024 Mar-Apr;74(2):203. doi: 10.3322/caac.21830]. CA Cancer J Clin 2024;74(1):12-49. doi:10.3322/caac.21820
Symptoms and Signs of Oral Squamous Cell Carcinoma
Oral lesions are asymptomatic initially, highlighting the need for oral screening. The lesions may appear as areas of erythroplakia or leukoplakia and may be exophytic or ulcerated. Cancers are often indurated and firm with a rolled border. As the lesions increase in size, pain, dysarthria, and dysphagia may result.

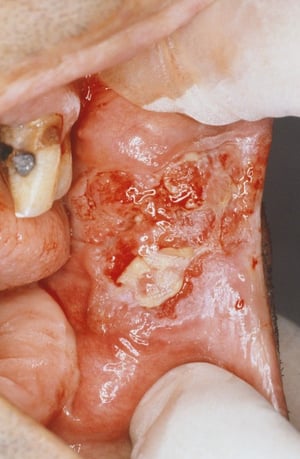
This photo shows a close-up of the inside of the mouth (the buccal mucosa) in a patient with squamous cell carcinoma of the oral mucosa.
This photo shows a close-up of the inside of the mouth (the buccal mucosa) in a patient with squamous cell carcinoma of
CLINICA CLAROS/SCIENCE PHOTO LIBRARY


Erythroplakia is a general term that can describe red, flat, or eroded velvety lesions that develop in the mouth. In this image, an exophytic squamous cell carcinoma on the tongue is surrounded by a margin of erythroplakia.
Erythroplakia is a general term that can describe red, flat, or eroded velvety lesions that develop in the mouth. In th
Image provided by Jonathan A. Ship, DMD.

Leukoplakia is a general term that can describe white hyperkeratotic plaques that develop in the mouth. The majority prove to be benign. However, in this image, squamous cell carcinoma is present in 1 of the leukoplakic lesions on the ventral surface of the tongue (arrow).
Leukoplakia is a general term that can describe white hyperkeratotic plaques that develop in the mouth. The majority pr
Image provided by Jonathan A. Ship, DMD.
This photo shows a close-up of the inside of the mouth (the buccal mucosa) in a patient with squamous cell carcinoma of the oral mucosa.
This photo shows a close-up of the inside of the mouth (the buccal mucosa) in a patient with squamous cell carcinoma of
CLINICA CLAROS/SCIENCE PHOTO LIBRARY
Erythroplakia is a general term that can describe red, flat, or eroded velvety lesions that develop in the mouth. In this image, an exophytic squamous cell carcinoma on the tongue is surrounded by a margin of erythroplakia.
Erythroplakia is a general term that can describe red, flat, or eroded velvety lesions that develop in the mouth. In th
Image provided by Jonathan A. Ship, DMD.
Leukoplakia is a general term that can describe white hyperkeratotic plaques that develop in the mouth. The majority prove to be benign. However, in this image, squamous cell carcinoma is present in 1 of the leukoplakic lesions on the ventral surface of the tongue (arrow).
Leukoplakia is a general term that can describe white hyperkeratotic plaques that develop in the mouth. The majority pr
Image provided by Jonathan A. Ship, DMD.
Diagnosis of Oral Squamous Cell Carcinoma
Biopsy
Endoscopy to detect second primary cancer
Chest CT or radiograph and CT of head and neck
Most lesions are discovered during routine examination. Dental professionals carefully examine the oral cavity and oropharynx during routine care and may do a brush biopsy of abnormal areas.
Any suspicious areas should be biopsied. Incisional or brush biopsy can be done depending on the surgeon's preference.
Direct laryngoscopy and esophagoscopy are done in all patients with oral cavity cancer to exclude a simultaneous second primary cancer. Head and neck CT usually is done, and a chest CT or radiograph is done; however, as in most sites in the head and neck, PET/CT plays a larger role in the evaluation of patients with oral cavity cancer. (See table .)
Staging of Lip and Oral Cancer
Stage | Tumor (Maximum Penetration)* | Regional Lymph Node Metastasis† | Distant Metastasis‡ |
|---|---|---|---|
I | T1 | N0 | M0 |
II | T2 | N0 | M0 |
III | T3 or | N0 | M0 |
T1–3 | N1 | M0 | |
IVA | T1–3 | N2 | M0 |
T4a | N0–2 | M0 | |
IVB | T4b | Any N | M0 |
Any T | N3 | M0 | |
IVC | Any T | Any N | M1 |
* Definition of Primary Tumor (T) | |||
T1 | Tumor ≤ 2 cm with DOI (depth of invasion, not tumor thickness) ≤ 5 mm | ||
T2 | Tumor ≤ 2 cm with DOI > 5 mm OR tumor > 2 cm and ≤ 4 cm with DOI ≤ 10 mm | ||
T3 | Tumor > 2 cm and ≤4 cm with DOI > 10 mm OR tumor > 4 cm with DOI ≤ 10 mm | ||
T4a | Moderately advanced local disease Lip: Tumor invades through cortical bone or involves the inferior alveolar nerve, floor of mouth, or skin of face (eg, chin or nose) Oral cavity: Tumor > 4 cm with DOI > 10 mm OR tumor invades adjacent structures only (eg, through cortical bone of the mandible or maxilla, or involves the maxillary sinus or skin of the face) Note: Superficial erosion of bone/tooth socket (alone) by a gingival primary is not sufficient to classify a tumor as T4. | ||
T4b | Very advanced local disease Tumor invades masticator space, pterygoid plates, or skull base and/or encases internal carotid artery | ||
† Definition of Regional Lymph Node (N) | |||
N1 | Metastasis in a single ipsilateral node ≤ 3 cm and no extranodal extension | ||
N2 | Metastasis in single ipsilateral node > 3 cm but ≤ 6 cm and no extranodal extension; OR in multiple ipsilateral nodes ≤ 6 cm and no extranodal extension; OR in bilateral or contralateral nodes ≤ 6 cm and no extranodal extension | ||
N3 | Metastasis in a node > 6 cm and no extranodal extension; OR in any nodes and extranodal extension | ||
‡ Definition of Distant Metastasis (M) | |||
M0 | No distant metastasis | ||
M1 | Distant metastasis | ||
Data from Amin MB, Edge S, Greene F, Byrd DR, et al: American Joint Committee on Cancer (AJCC) Cancer Staging Manual, 8th edition. New York, Springer, 2017; AJCC Cancer Staging Form Supplement, 2018. | |||
Treatment of Oral Squamous Cell Carcinoma
Surgery, with postoperative radiation or chemoradiation as needed
For most oral cavity cancers, surgery is the initial treatment of choice. Radiation or chemoradiation is added postoperatively if disease is more advanced or has high-risk histologic features (1).
Selective neck dissection is indicated if the risk of nodal disease exceeds 15 to 20%. Although there is no firm consensus, neck dissections are typically done for any lesion with a depth of invasion > about 3.5 mm.
Routine surgical reconstruction is the key to reducing postoperative oral disabilities; procedures range from local tissue flaps to free tissue transfers. Speech and swallowing therapy may be required after significant resections.
Radiation therapy is an alternative treatment. Chemotherapy is not used routinely as primary therapy but is recommended as adjuvant therapy along with radiation in patients with advanced nodal disease.
Treatment of squamous cell carcinoma of the lip is surgical excision with reconstruction to maximize postoperative function. When large areas of the lip exhibit premalignant change, the lip can be surgically shaved, or a laser can remove all affected mucosa. Mohs surgery can be used. Thereafter, appropriate sunscreen application is recommended.
Treatment reference
1. National Cancer Institute: Lip and Oral Cancer Treatment (PDQ)---Health Professional Version. updated June 4, 2024. Accessed July 30, 2024.
Prognosis for Oral Squamous Cell Carcinoma
If carcinoma of the tongue is localized (no lymph node involvement), 5-year survival is > 80% (1). For localized carcinoma of the floor of the mouth, 5-year survival is about 75% (1). Lymph node metastasis decreases survival rate. Metastases reach the regional lymph nodes first and later the lungs.
For localized carcinoma of the lip, 5-year survival is > 90% (1). For lower lip lesions, metastases are rare. Carcinoma of the upper lip tends to be more aggressive and metastatic.
Prognosis reference
1. American Cancer Society medical and editorial content team: Oral Cavity (Mouth) and Oropharyngeal (Throat) Cancer: Survival rates for oral cavity and oropharyngeal cancer. Updated March 1, 2023. Accessed July 30, 2024.
Key Points
The chief risk factors for oral squamous cell carcinoma are heavy smoking and alcohol use.
Oral cancer is sometimes asymptomatic initially, so oral screening (typically by dental professionals) is useful for early diagnosis.
Perform direct laryngoscopy and esophagoscopy to exclude a simultaneous second primary cancer.
Once cancer is confirmed, do head and neck CT, a chest imaging (CT or radiograph), and sometimes PET/CT.
Initial treatment is usually surgical.





