

Choking in an infant is usually caused by a small object in the oropharynx, hypopharynx, or trachea (eg, food, toy, button, coin, or balloon). If the airway obstruction is severe, then back blows followed by chest thrusts are administered to dislodge the object.
(See also Overview of Respiratory Arrest and Airway Establishment and Control.)
Indications
Severe upper airway obstruction in an infant (under age 1 year), caused by choking on a foreign object.
Signs of severe airway obstruction in an infant include:
Inability to cry or make much sound
Weak, ineffective coughing
Stridor
Retractions during inspiratory effort with no air movement
Cyanosis
Do not interfere if the infant can cry and make significant sounds, cough effectively, or breathe adequately; such infants do not have severe airway obstruction. Furthermore, strong coughs and cries can help expel the object out of the airway (1).
Contraindications
Absolute contraindications:
Do not do back blows or chest thrusts if the infant stops breathing for reasons other than an obstructed airway (eg, asthma, respiratory infection, severe trauma).
For an unconscious infant with a suspected upper airway obstruction perform cardiopulmonary resuscitation (CPR)
Relative contraindications:
None
Complications
Rib injury or fracture
Internal organ injury
Equipment
None
Additional Considerations
This rapid first aid procedure is done immediately wherever the infant is choking.
Relevant Anatomy
The epiglottis usually protects the airway from aspiration of foreign objects. Objects that are aspirated beyond the epiglottis may be stopped by the vocal cords in the larynx and, at this level or below, cause life-threatening airway obstruction.
In infants and children, the cricoid cartilage, which lies inferior to the vocal cords, is the narrowest part of the upper airway. Sometimes, objects become trapped between the vocal cords and the cricoid ring, resulting in an obstruction that is particularly difficult to clear.
Positioning
For back blows, place the infant prone along your forearm, using your thigh or lap for support. Hold the infant’s chest in your hand and the jaw with your fingers. Tilt the infant head-downward, such that the head is lower than the body (see figure ).
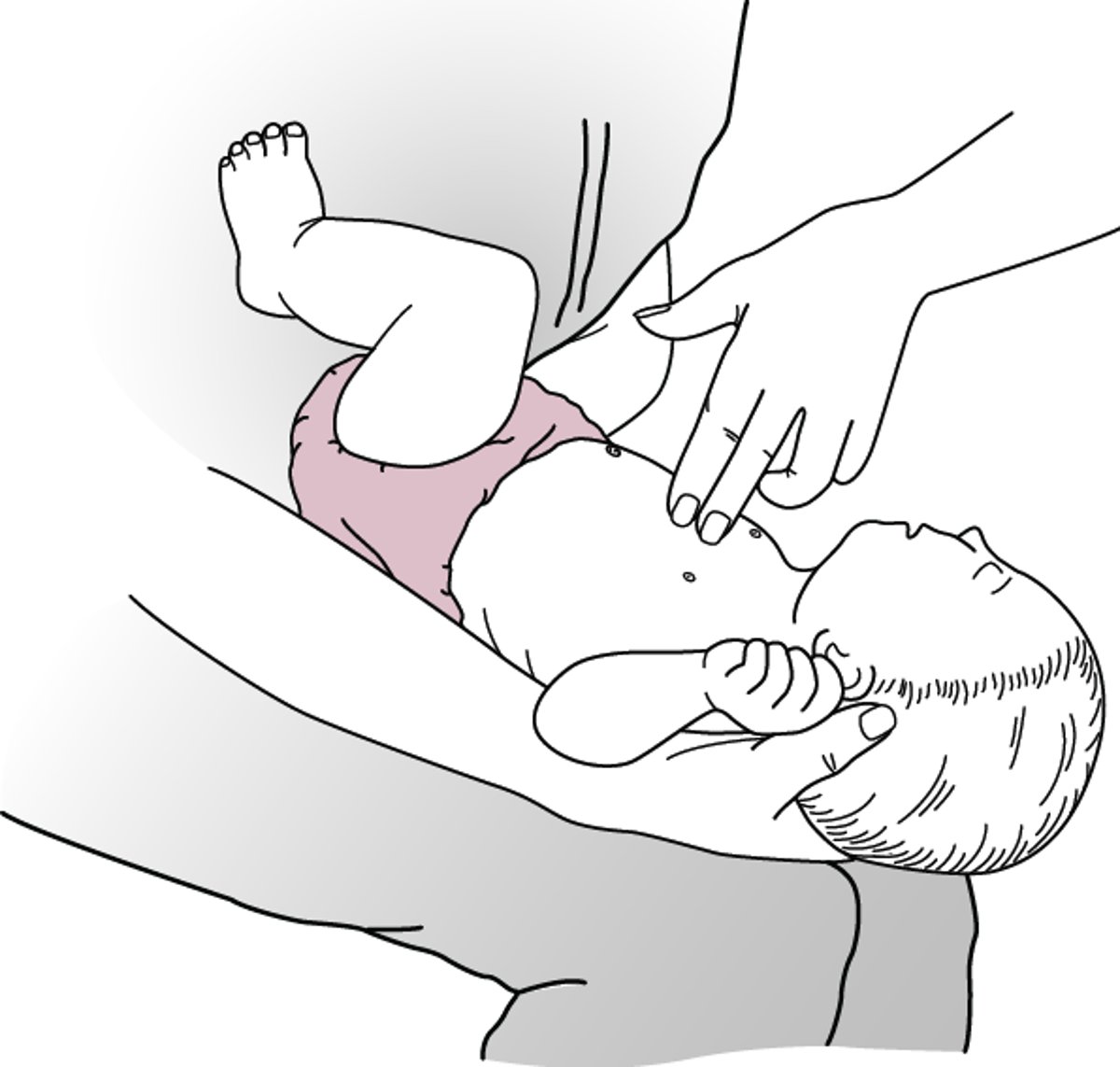
For chest thrusts, place the infant supine along your forearm, using your thigh or lap for support. Hold the back of the infant's head in your hand. Again, incline the infant such that the head is dependent to the body (see figure ).
Back Blows—Infant

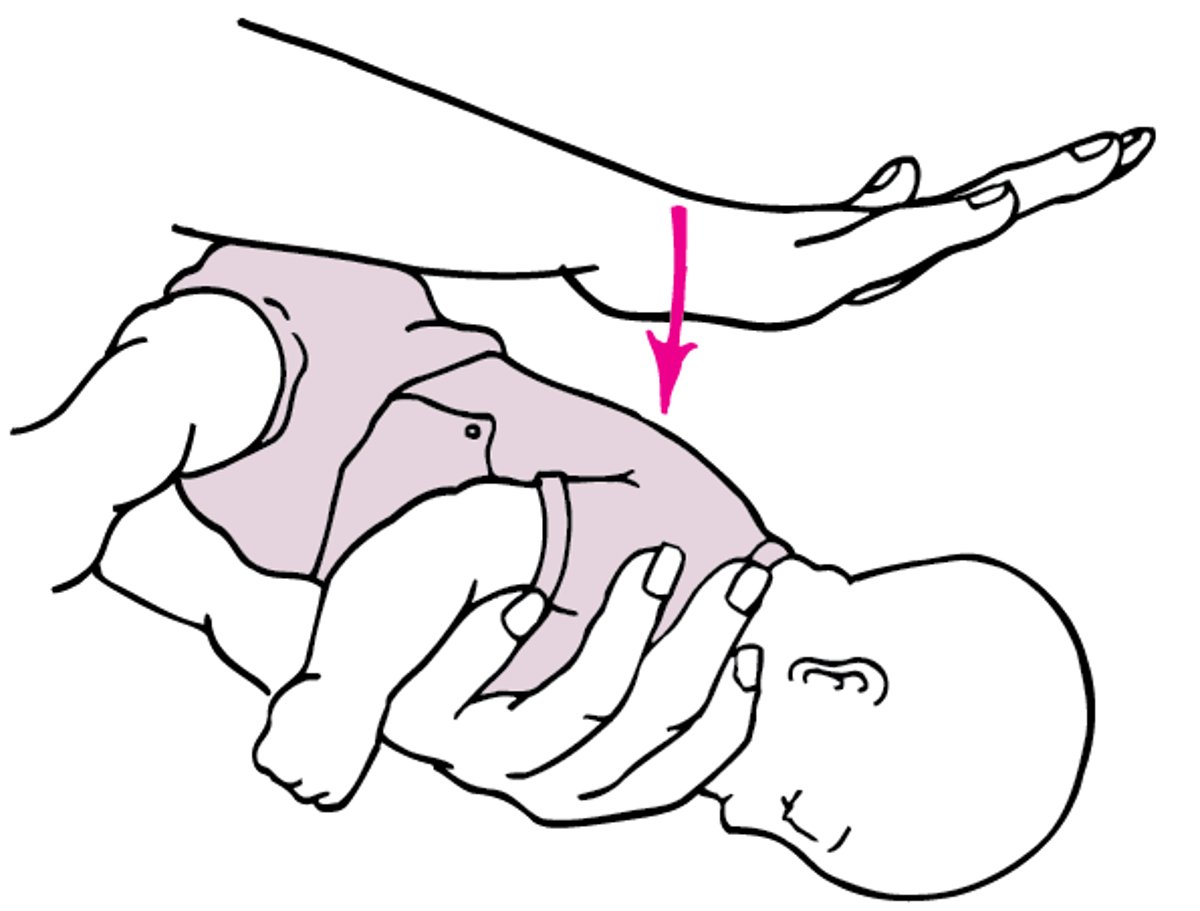
Chest Thrusts—Infant
Chest thrusts are delivered on the lower half of the sternum, just below the nipple level. |

Step-by-Step Description of Procedure
Determine if there is severe airway obstruction. Look for signs of severe airway obstruction, such as the inability to cry audibly, cough effectively, or breathe adequately (eg, stridor, retractions, cyanosis).
If the infant has a strong cry or is coughing hard, do not do these procedures. If you have determined that the infant has severe airway obstruction, proceed with the following procedures.
Tell someone to call 911 (or other local emergency response system) while you begin the procedure. If you are alone, shout for help and begin the procedure.
Hold the infant face-down along your forearm using your thigh or lap for support. Hold the infant’s chest in your hand and open the jaw by pulling the mandible with your fingers. Point the infant’s head downward and lower than the body.
Give up to 5 quick, forceful back blows between the infant’s shoulder blades using the palm of your free hand.
Check the mouth to see whether the aspirated foreign body is visible; if it can be easily removed, remove it.
If the object does not come out of the airway after 5 back blows, turn the infant face-up.
Hold the infant face-up along your forearm using your thigh or lap for support. Hold the head in your hand with the head lower than the torso.
Place the second and third fingers on the middle of the infant’s sternum just below the nipples. Avoid the lower ribs or the tip of the sternum.
Give up to 5 quick thrusts, compressing the chest about one-third to one-half the depth of the chest—usually about 1.5 to 4 cm (0.5 to 1.5 inches) for each thrust.
Continue to deliver 5 back blows followed by 5 chest thrusts until the object is dislodged or the infant becomes unconscious.
Do not try to grasp and pull out the object if the infant is conscious.
If the infant becomes unresponsive (unconscious), shout for help if you are still alone and begin infant cardiopulmonary resuscitation (CPR). If you are alone, after 1 minute of CPR ensure that the local emergency response system has been activated.
If the infant is unconscious and you can see the object blocking the airway, try to remove it with a finger. Try to remove the object only if you can see it.

Aftercare
Carefully examine the infant as soon as possible, even after successful removal of the airway obstruction and resumption of normal breathing.
If not already at a healthcare facility, ensure that the infant is evaluated by a clinician to be evaluated for complications (eg rib injury, blunt internal organ injury).
Warnings and Common Errors
Do not do back blows or chest thrusts if the choking infant can cry audibly, cough forcefully, or breathe adequately.
Do not do back blows or chest thrusts if the infant stops breathing for reasons other than an obstructed airway (eg, asthma, respiratory infection, severe trauma). Do perform CPR in these cases.
Do not do blind finger sweeps on infants.
Do not do abdominal thrusts (Heimlich maneuver) on infants as it risks injuring the liver.
Tips and Tricks
It is important to use gravity as an ally. Keep the infant's head lower than its torso during the procedure.
Reference
1. Topjian AA, Raymond TT, Atkins D, et al. Part 4: Pediatric Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2020;142(16_suppl_2):S469-S523. doi:10.1161/CIR.0000000000000901





