

Fallopian tube problems (a blocked or damaged fallopian tube) can prevent sperm from reaching the egg or prevent the egg or fertilized egg (zygote) from moving from the ovary to the uterus to be implanted. Abnormalities in the pelvis, including the uterus (such at uterine fibroids), can prevent the egg from attaching to (implanting in) the lining of the uterus and can block the fallopian tubes.
To identify a fallopian tube or other pelvic abnormality, doctors may take x-rays as a radiopaque contrast agent is injected through the cervix (hysterosalpingography), do ultrasonography after a salt solution is injected inside the uterus (sonohysterography), or view the organs through a viewing tube (laparoscope) inserted through an incision just below the navel.
Treatment depends on the type and location of the abnormality (fallopian tubes or uterus) and a woman's age, but in vitro fertilization or surgery may be recommended.
(See also Overview of Infertility.)
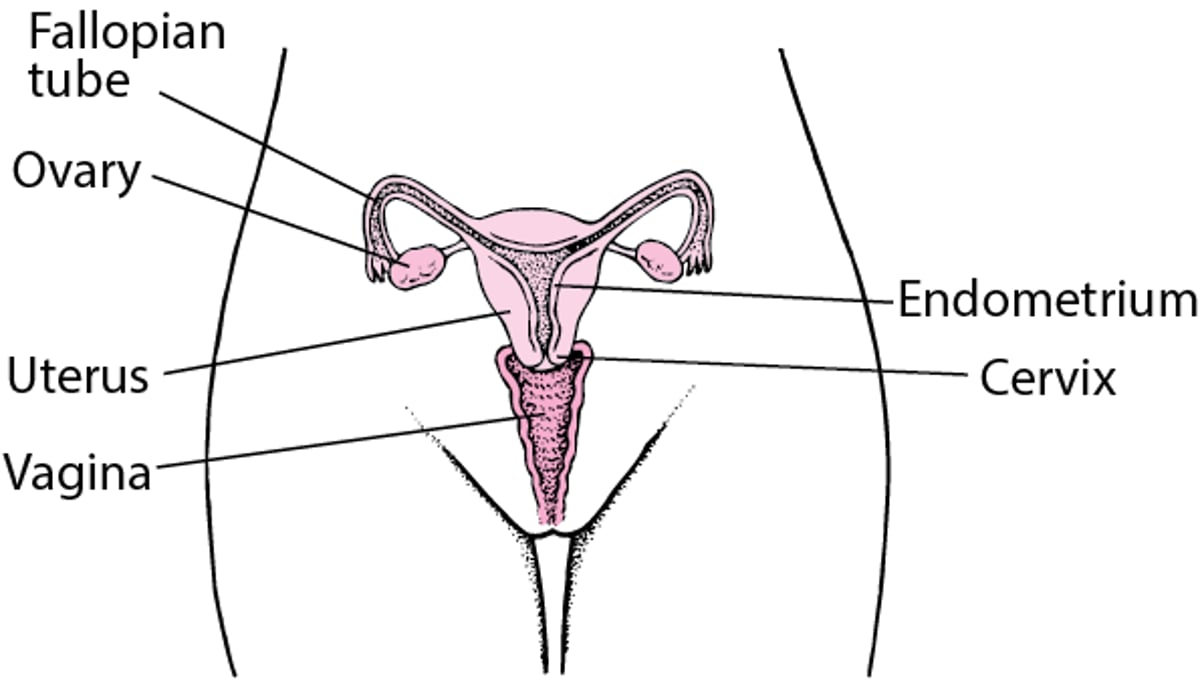
Internal Female Reproductive Anatomy

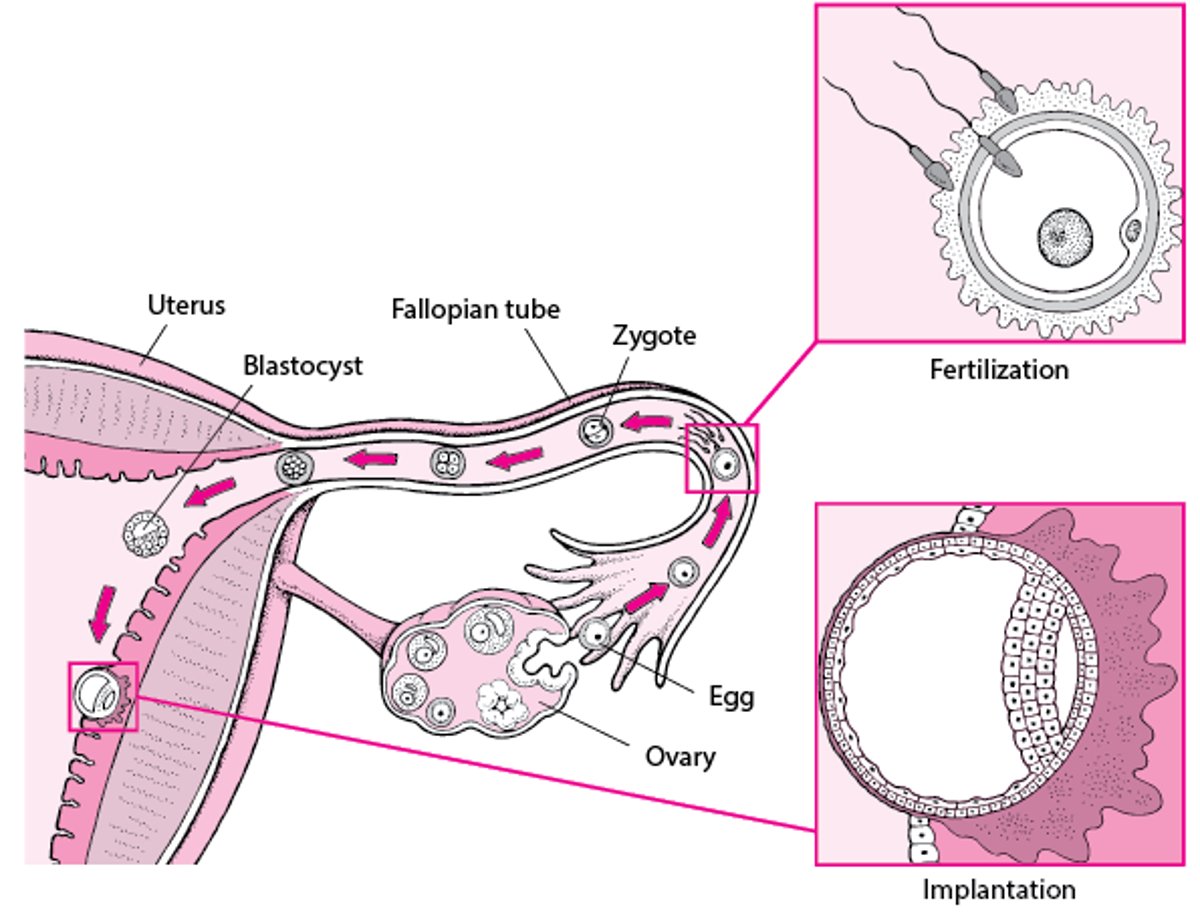
Ovulation and Implantation

Causes
Fallopian tube problems result from conditions that block or damage the tube, including the following:
Pelvic infections (such as pelvic inflammatory disease)
A past pregnancy in the fallopian tubes (ectopic pregnancy)
Surgery in the pelvis or lower abdomen
Inflammation that damages the uterus and fallopian tubes (such as that caused by tuberculosis or inflammatory bowel disease)
Bacteria, such as those that can cause pelvic inflammatory disease, can enter the vagina during sexual activity with a partner who has a sexually transmitted infection, such as gonorrhea. The bacteria can spread from the vagina to infect the cervix. They may then spread upward, to the uterus and sometimes the fallopian tubes. Some bacteria such as chlamydiae can infect the fallopian tubes without causing any symptoms. These infections may permanently damage the fallopian tubes. Scar tissue may form and block the fallopian tubes.
Abnormalities in the pelvis can block the tubes or prevent the egg from implanting in the uterus. They include the following:
Bands of scar tissue (adhesions) that form between normally unconnected structures in the uterus or pelvis (Asherman syndrome)
Birth defects of the uterus and fallopian tubes
Adhesions in the uterus are usually caused by infections or an injury during surgery, usually dilation and curettage (D and C). Scarring may also affect the cervix, especially after an infection of, injury to, or surgery on the cervix.
Diagnosis
Sometimes tests for pelvic infection
Sonohysterography (saline infusion sonography) or hysterosalpingography, if sonohysterography is not available
Hysteroscopy to further evaluate abnormalities
Rarely, laparoscopy
If pelvic infection is suspected, tests to check for gonorrhea or chlamydial infection are done. Screening for sexually transmitted infections is a usual part of routine care when women are trying to become pregnant.
Procedures are done to determine whether the fallopian tubes are blocked. They include hysterosalpingography, sonohysterography, laparoscopy, and hysteroscopy. During laparoscopy and hysteroscopy, diagnosis and treatment are often done at the same time.
Sonohysterography (saline infusion sonography)
Sonohysterography is used to detect and/or to further evaluate problems with the fallopian tubes and other abnormalities in the pelvis.
A salt (saline) solution is injected into the interior of the uterus through the cervix during ultrasonography so that the interior is distended and abnormalities can be seen more easily. If the solution flows into the fallopian tubes, the tubes are not blocked.
Sonohysterography is quick and does not require an anesthetic. It is considered safer than hysterosalpingography because it does not require radiation or injection of a contrast agent.
After sonohysterography, for unknown reasons, fertility in young women appears to be slightly improved if the results are normal. Doctors may wait to see if young women become pregnant after this procedure before additional tests of fallopian tube function are done.
Sonohysterography, where available, has replaced hysterosalpingography. Sonohysterography has the advantages of being able to be performed in the clinician's office, does not require exposure to radiation, and is generally less costly than hysterosalpingography.
Hysterosalpingography
For hysterosalpingography, x-rays are taken as a radiopaque contrast agent is injected through the cervix. The contrast agent outlines the interior of the uterus and fallopian tubes. This procedure is done a few days after a woman’s menstrual period ends and before ovulation occurs. Hysterosalpingography does not require an anesthetic. Allergic reactions to the contrast agent (including iodine) are possible.
Hysterosalpingography can detect some structural disorders that can block the fallopian tubes. However, in about 15% of cases, hysterosalpingography indicates that the fallopian tubes are blocked when they are not—called a false-positive result.
As with sonohysterography, after hysterosalpingography, fertility in young women appears to be slightly improved if the results are normal.
Hysteroscopy
If an abnormality within the uterus is detected, doctors may examine the uterus with an instrument with a camera called a hysteroscope, which is inserted through the vagina and cervix into the uterus. If adhesions, a polyp, or a small fibroid is detected, instruments inserted through the hysteroscope may be used to dislodge or remove the abnormal tissue, increasing the chances that a woman will become pregnant.
Laparoscopy
If evidence suggests that the fallopian tubes are blocked or that a woman may have endometriosis, a small viewing tube called a laparoscope is inserted in the pelvic cavity through a small incision just below the navel. Usually, a general anesthetic is used. Laparoscopy enables doctors to directly view the uterus, fallopian tubes, and ovaries. However, this procedure is rarely done to diagnose fallopian tube problems.
Instruments inserted through the laparoscope may also be used to dislodge or remove abnormal tissue in the pelvis.
Treatment
Antibiotics, if a pelvic infection is diagnosed
Laparoscopy and/or hysteroscopy to treat or remove abnormal tissue
In vitro fertilization or, in younger women, sometimes surgery
If pelvic infection is diagnosed, it is treated with antibiotics.
Treatment of fallopian tube or pelvic problems depends on the cause. Abnormal tissue is sometimes removed (such as uterine fibroids or polyps) if it is detected during a diagnostic surgery (for example, during hysteroscopy or laparoscopy).
Surgery can be done to repair a fallopian tube damaged by an ectopic pregnancy, an infection, or a prior tubal sterilization procedure, especially in younger women if the damage is not severe. However, after such surgery, the chances of a normal pregnancy are small. The chances of an ectopic pregnancy are higher than usual both before and after such surgery. Consequently, in vitro fertilization is often recommended instead.
Assisted reproductive technologies are often a necessity or an alternative, particularly in women under age 30.





