





Osteoarthritis is a chronic disorder that causes damage to the cartilage and surrounding tissues and is characterized by pain, stiffness, and loss of function.
Arthritis due to damage of joint cartilage and surrounding tissues becomes very common with aging.
Pain, swelling, and bony overgrowth are common, as well as stiffness that follows awakening or inactivity and disappears within 30 minutes, particularly if the joint is moved.
The diagnosis is based on symptoms and x-rays.
Treatment includes exercises and other physical measures, medications that reduce pain and improve function, and, for very severe cases, joint replacement or other surgery.
Osteoarthritis, the most common joint disorder, often begins in the 40s and 50s and affects almost all people to some degree by age 80. Before the age of 40, men develop osteoarthritis more often than do women, often because of injury or deformities. Many people have some evidence of osteoarthritis on x-rays (often by age 40), but only half of these people have symptoms. From age 40 to 70, women develop the disorder more often than do men. After age 70, the disorder develops in both sexes equally.
Osteoarthritis is classified as
Primary
Secondary
In primary (or idiopathic) osteoarthritis, the cause is not known (primary osteoarthritis represents the large majority of cases). Primary osteoarthritis may affect only specific joints, such as hand, knee, or hip joints, or it may affect many joints.
In secondary osteoarthritis, the cause is another disease or condition, such as
An infection
A joint abnormality that was present at birth
An injury
A metabolic disorder—for example, excess iron in the body (hemochromatosis) or excess copper in the liver (Wilson disease)
A disorder that has damaged joint cartilage—for example, rheumatoid arthritis or gout
Some people who repetitively stress 1 joint or a group of joints, such as foundry workers, farmers, coal miners, and bus drivers, are particularly at risk. The major risk factor for osteoarthritis of the knee comes from having an occupation that involves bending the joint. Curiously, long-distance running does not increase the risk of developing the disorder. However, once osteoarthritis develops, this type of exercise often makes the disorder worse. Obesity may be a major factor in the development of osteoarthritis, particularly of the knee and especially in women.
Causes of Osteoarthritis
Normally, cartilage reduces the friction level in joints and protects them from wearing out, even after years of typical use, overuse, or injury. The cause of osteoarthritis is often unknown, but it is sometimes caused by tissue damage. In an attempt to repair a damaged joint, chemicals accumulate in the joint and increase the production of the components of cartilage, such as collagen (a tough, fibrous protein in connective tissue) and proteoglycans (substances that provide resilience). Next, the cartilage may swell because of water retention, become soft, start to breakdown, and then develop cracks on the surface. Tiny cavities form in the bone beneath the cartilage, weakening the bone.
The attempt of the tissues to repair the damage may lead to new growth of bone and other tissue. Bone can overgrow at the edges of the joint, causing bumps or bone spurs (also called osteophytes) that can be seen and felt. Ultimately, the smooth, slippery surface of the cartilage becomes rough and pitted, so that the joint can no longer move smoothly and absorb impact. All the components of the joint—bone, joint capsule (tissues that enclose most joints), synovial tissue (tissue lining the joint cavity), tendons, ligaments, and cartilage—fail in various ways, thus altering the function of the joint.
Symptoms of Osteoarthritis
Usually, osteoarthritis symptoms develop gradually and affect only 1 or a few joints at first. Joints of the fingers, base of the thumbs, neck, lower back, big toes, hips, and knees are commonly affected.
Pain, often described as a deep ache, is the first symptom and, when in the weight-bearing joints (for example, the knees and hips), is usually made worse by activities that involve weight bearing (such as standing). In some people, the joint may be stiff after sleep or some other inactivity, but the stiffness usually subsides within 30 minutes, particularly if the joint is moved.
As the condition causes more symptoms, the joint may become less movable and may not be able to fully straighten or bend. New growth of bone and other tissue can enlarge the joints. The irregular cartilage surfaces cause joints to grind, grate, or crackle when they are moved, and tenderness develops.
Osteoarthritis in the hand can cause pain, stiffness, and functional limitations. Bony growths commonly develop in the joints closest to the fingertips (called Heberden nodes) or middle of the fingers (called Bouchard nodes).
In some joints (such as the knee), the ligaments, which surround and support the joint, stretch so that the joint becomes unstable and the muscles moving that joint may weaken. Alternatively, the hip or knee may become stiff, losing its range of motion. Moving the joint (particularly when standing, climbing stairs, or walking) can be very painful.
Osteoarthritis often affects the spine. Back pain is the most common symptom. Usually, damaged discs or joints in the spine cause only mild pain and stiffness. However, osteoarthritis in the neck or lower back can cause numbness, pain, and weakness in an arm or leg if the overgrowth of bone presses on nerves. The overgrowth of bone may be within the spinal canal in the lower back (lumbar spinal stenosis), pressing on nerves before they exit the canal to go to the legs. This pressure may cause leg pain with walking, suggesting incorrectly that the person has a reduced blood supply to the legs (intermittent claudication). Rarely, bony growths in the neck compress the esophagus, making swallowing difficult.
Osteoarthritis may be stable for many years or may progress very rapidly, but most often it progresses slowly after symptoms develop. Many people develop some degree of disability.
People who develop a red, hot, and swollen joint should be evaluated by a doctor because these episodes are not usually caused by osteoarthritis and could indicate an infection or gout.
Osteoarthritis (https://www.youtube.com/watch?v=sUOlmI-naFs) by Osmosis (https://open.osmosis.org/) is licensed under CC-BY-SA 4.0 (https://creativecommons.org/licenses/by-sa/4.0/).



Osteoarthritis of the hand causes the outermost joints of the fingers to become larger (Heberden nodes).
Osteoarthritis of the hand causes the outermost joints of the fingers to become larger (Heberden nodes).
DR P. MARAZZI/SCIENCE PHOTO LIBRARY


In this photo, the Bouchard nodes are most visible on the middle joints of the fingers of the right hand and the middle joints of the pointer and middle fingers of the left hand.
In this photo, the Bouchard nodes are most visible on the middle joints of the fingers of the right hand and the middle
© Springer Science+Business Media

Osteoarthritis (https://www.youtube.com/watch?v=sUOlmI-naFs) by Osmosis (https://open.osmosis.org/) is licensed under CC-BY-SA 4.0 (https://creativecommons.org/licenses/by-sa/4.0/).

Osteoarthritis of the hand causes the outermost joints of the fingers to become larger (Heberden nodes).
Osteoarthritis of the hand causes the outermost joints of the fingers to become larger (Heberden nodes).
DR P. MARAZZI/SCIENCE PHOTO LIBRARY
In this photo, the Bouchard nodes are most visible on the middle joints of the fingers of the right hand and the middle joints of the pointer and middle fingers of the left hand.
In this photo, the Bouchard nodes are most visible on the middle joints of the fingers of the right hand and the middle
© Springer Science+Business Media
Diagnosis of Osteoarthritis
X-rays
The doctor makes the diagnosis of osteoarthritis based on the characteristic symptoms, physical examination, and the appearance of joints on x-rays (such as bone enlargement and narrowing of the joint space). However, x-rays are not very useful for detecting osteoarthritis early because they do not show changes in cartilage, which is where the earliest abnormalities occur. Also, changes on the x-ray often do not closely correspond with a person's symptoms. For example, an x-ray may show only a minor change in a person who has severe symptoms, or an x-ray may show numerous changes in a person who has very few if any symptoms.
Magnetic resonance imaging (MRI) can reveal early changes in cartilage, but it is rarely needed for the diagnosis.
There are no blood tests for the diagnosis of osteoarthritis, but certain blood tests may help rule out other disorders.
If a joint is swollen, doctors may inject an anesthetic to numb the area and then insert a needle into the joint to draw a sample of the joint fluid. The fluid is examined to differentiate osteoarthritis from other joint disorders such as infection and gout.
Treatment of Osteoarthritis
Physical measures, including physical and occupational therapy, joint protection, and appropriate weight loss
Medications
Surgery
The main goals of osteoarthritis treatment are to
Relieve pain
Maintain joint flexibility
Optimize joint and overall function
These goals are primarily achieved by physical measures that involve exercises for strength, flexibility, and endurance and rehabilitation (physical therapy and occupational therapy). People are taught how modifying their daily activities can help them live with osteoarthritis. Additional treatment includes medications, surgery (for some people), and newer therapies.
Physical measures
Appropriate exercises—including stretching, strengthening, and postural exercises—help maintain healthy cartilage, increase a joint’s range of motion, and most importantly strengthen surrounding muscles so that they can absorb stress better. Exercise can improve joint symptoms, mobility, and quality of life in people with knee and/or hip osteoarthritis. Doctors often recommend people exercise in water (such as in a pool) particularly for people with more severe pain who may benefit from lower impact exercise.
Stretching exercises should be done daily.
Exercise must be balanced with a few minutes of rest of painful joints (every 4 to 6 hours during the day), but immobilizing a joint is more likely to worsen the disease than relieve it.
Using excessively soft chairs, recliners, mattresses, and car seats may worsen symptoms.
People should not put pillows under their knees when reclining because doing so can cause the hip and knee muscles to become tight. (This recommendation contrasts with the recommendation that people with low back pain and sciatica put a pillow between their knees. For such people, using a pillow relieves the stress on the lower back and hip [see Sciatica].)
Moving car seats forward, using straight-backed chairs with relatively high seats (such as kitchen or dining room chairs), firm mattresses, and bed boards (available at many lumber yards), and wearing orthotics, supportive shoes, or athletic shoes are often recommended.
Toilet seat risers can make standing up easier and less uncomfortable for people who have painful osteoarthritis of the knees or hips, particularly if their muscles are weak.
For osteoarthritis of the spine, specific exercises sometimes help, and back supports may be needed when pain is severe. Exercises should include both muscle-strengthening as well as low-impact aerobic exercises (such as walking, swimming, elliptical machine use, and stationary bicycle riding). If possible, people should maintain ordinary daily activities and continue to perform their normal activities, such as a hobby or job. However, physical activities may have to be adjusted to limit lifting and bending in ways that can aggravate the pain of osteoarthritis.
The following additional measures may help relieve pain and help people live with osteoarthritis:
Physical therapy, often with heat therapy, such as heating pads, and occupational therapy can be helpful.
Range-of-motion exercises done gently in warm water are helpful because heat improves muscle function by reducing stiffness and muscle spasm.
Shoe inserts (orthotics), supportive shoes, or athletic shoes may help reduce pain caused by walking.
Special equipment (for example, canes, crutches, walkers, neck collars, elastic knee supports to protect joints, or a fixed seat placed in a bathtub to prevent too much stretching while washing) should be used as needed.
Weight loss can relieve some of the pressure on joints and improve joint mechanics.
Medications
Medications are used to supplement exercise and physical therapy. Medications, which may be used in combination or individually, do not directly alter the course of osteoarthritis. They are used to reduce symptoms and thus allow more normal daily activities.
A nonsteroidal anti-inflammatory drug (NSAID) may be used to lessen pain and swelling. NSAIDs reduce pain and inflammation in joints. NSAIDs also come in gel and cream forms that can be rubbed into the skin (such as diclofenac gel 1%) over the joints of the hands and knees and may help relieve symptoms. NSAIDs taken by mouth have a risk of serious side effects and, therefore, should be used for the shortest possible duration. People who take NSAIDs by mouth often also take a medication to protect the stomach lining and also may have their kidney function and blood pressure monitored.
Sometimes other types of pain medicine may be needed. For example, a cream made from cayenne pepper—the active ingredient is capsaicin, which disrupts pain transmission—can be applied directly to the skin over the joint. Doctors may also recommend lidocaine patches to numb the pain, but there is no evidence these patches are effective. Duloxetine, a type of antidepressant taken by mouth that calms pain signals, may reduce the pain caused by osteoarthritis.
Acetaminophen may be helpful for some people, particularly those who cannot take NSAIDs. However, acetaminophen is not as effective as NSAIDs for relieving joint pain. People should not take acetaminophen in higher than recommended doses, particularly if they have liver disease or drink considerable alcohol. When taking acetaminophen, people should also make sure not to simultaneously take 1 of the numerous over-the-counter medication products that contain acetaminophen.
More potent analgesics (or pain relievers), such as tramadol or other opioids, should be avoided.
Several nutritional supplements (such as glucosamine sulfate and chondroitin sulfate) have been tested for potential benefit in treating osteoarthritis. So far, results are mixed, and the potential benefit of glucosamine sulfate and chondroitin sulfate in treating pain is unclear, and they do not seem to change the progression of joint damage. The use of other nutritional supplements, such as turmeric and Boswellia serrata, are not routinely recommended. People may reasonably try them, but evidence that such supplements reduce pain is limited.
Surgery
Surgical treatment may help when other treatments fail to reduce pain or improve function. Some joints, most commonly the hip and knee, can be replaced with an artificial joint. Replacement, particularly of the hip, is usually very successful, almost always improving motion and function and dramatically decreasing pain. Therefore, joint replacement should be considered when pain is unmanageable and function becomes limited. Because an artificial joint does not last forever, the procedure is often delayed in very young people so the need for repeated replacements can be minimized. If other treatments are ineffective, surgical procedures can be done to help relieve symptoms of back or neck osteoarthritis, particularly nerve compression. The benefit of limited, arthroscopic surgical procedures for osteoarthritis of the knee, such as repair of the meniscus or reconstruction of knee ligaments, is uncertain.
A variety of methods that restore cells inside cartilage have been used in younger people with osteoarthritis (often caused by an injury) to help heal small defects in cartilage. However, such methods have not yet proved valuable when cartilage defects are extensive, as commonly occurs in older adults.
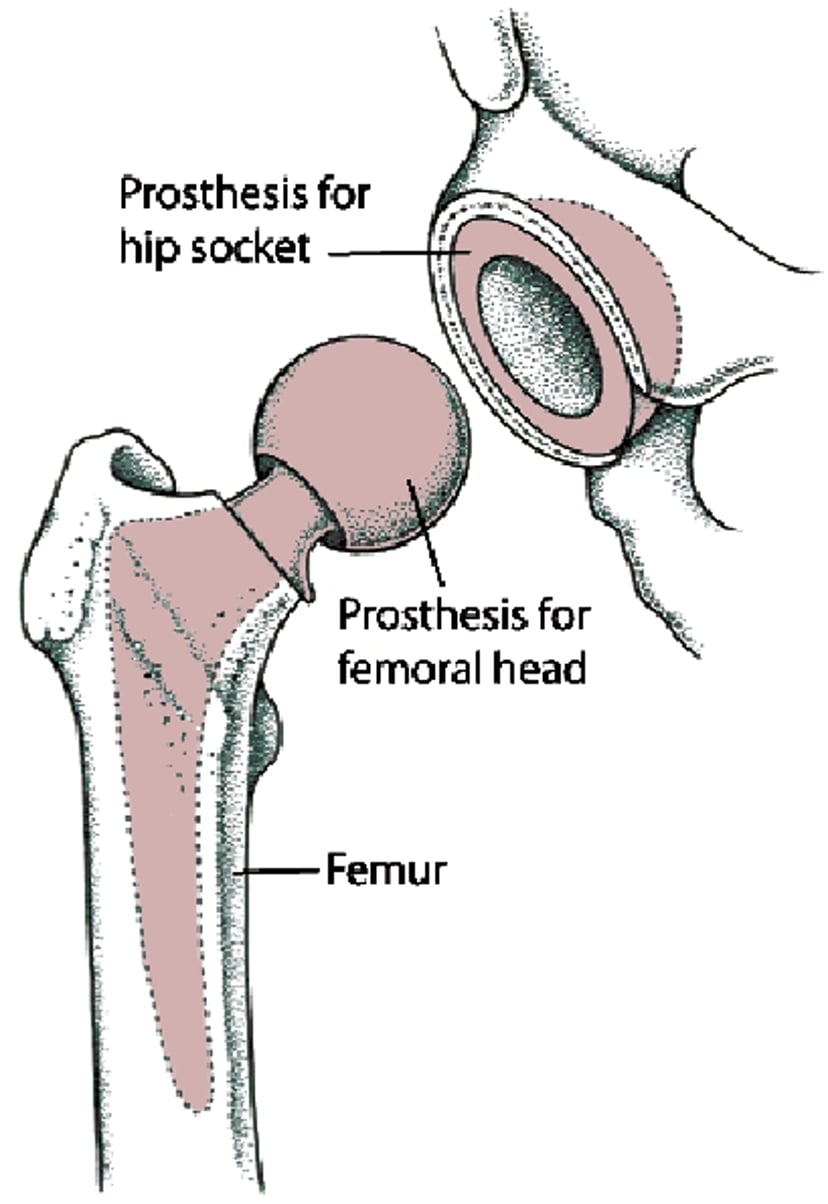
Replacing All of a Hip (Total Hip Replacement)
Sometimes the whole hip joint must be replaced. The whole hip joint is the top (head) of the thighbone (femur) and the surface of the socket into which the head of the thighbone fits. This procedure is called total hip replacement or total hip arthroplasty. The head of the thighbone is replaced with a ball-shaped part (prosthesis), made of metal. The prosthesis has a strong stem that fits within the center of the thighbone. The socket is replaced with a metal shell lined with durable plastic. |

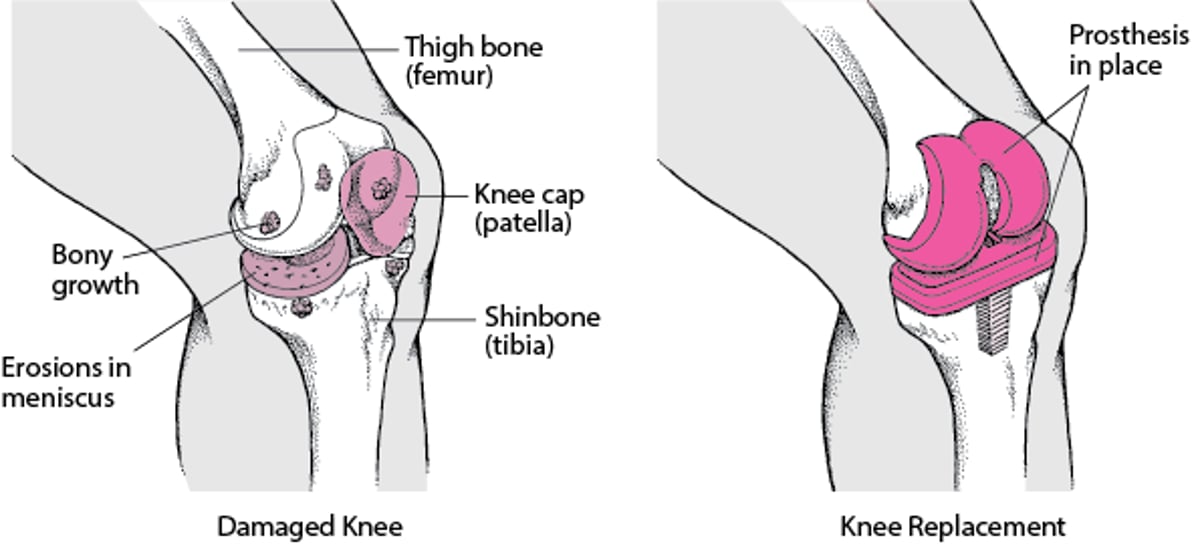
Replacing a Knee
A knee joint damaged by osteoarthritis may be replaced with an artificial joint. After a general anesthetic is given, the surgeon makes an incision over the damaged knee. The knee cap (patella) may be removed, and the ends of the thigh bone (femur) and shinbone (tibia) are smoothed so that the parts of the artificial joint (prosthesis) can be attached more easily. One part of the artificial joint is inserted into the thigh bone, the other part is inserted into the shinbone, and then the parts are cemented in place. |

Other treatments
Various other treatments are available to manage the pain of osteoarthritis, but their routine use is not recommended due to limited evidence of their effectiveness. However, some may reasonably be tried, particularly for people with symptoms that persist after other treatments are tried. Treatments that may reduce pain include
Heat therapy, such as heating pads or a damp and warm towel, can be applied to affected joints. (To avoid burns, people should be careful not to set a heating pad on high or leave it on for a long time.)
Cold may also be applied to reduce pain caused by temporary worsening in 1 joint.
Acupuncture releases various chemical messengers in the brain (neurotransmitters) that serve as natural painkillers and may be helpful.
Massage therapy by trained therapists and deep heat treatment with diathermy or ultrasound may be useful.
Sometimes a special form of cortisone may be injected directly into the joint. This treatment may provide temporary pain relief in some people.
A series of injections of hyaluronic acid (a substance similar to normal joint fluid) into the knee joint may provide some pain relief in some people. These injections should not be given more often than every 6 months. Hyaluronic acid injections do not slow the progression of the arthritis.
Electrical stimulation, such as transcutaneous electrical nerve stimulation (TENS), is not recommended for knee osteoarthritis.
Experimental therapies that may preserve cartilage are being studied.
Spotlight on Aging: Osteoarthritis
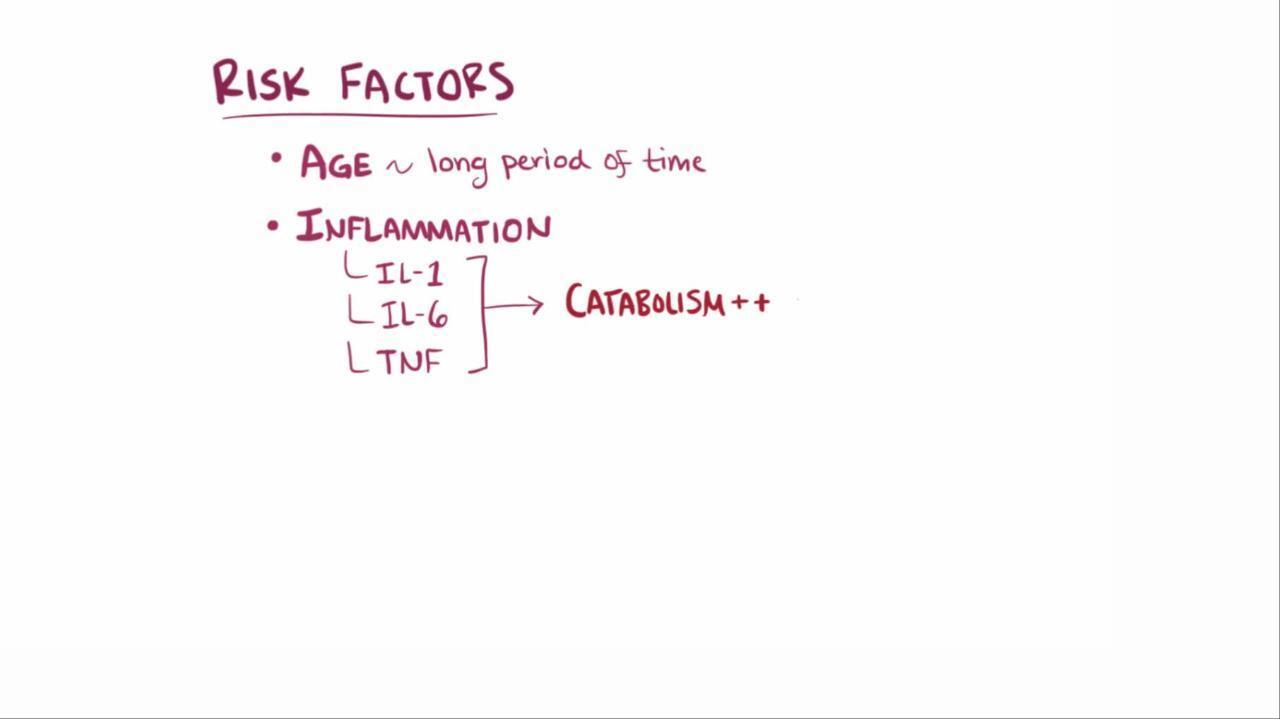
Many myths about osteoarthritis remain. For example, people think that it is an inevitable part of aging, like gray hair and skin changes, that it results in little disability, and that treatment is not effective. Osteoarthritis does become more common with aging. For instance, as people age, the following occur:
However, osteoarthritis is not an inevitable part of aging. It is not caused simply by the wear and tear that occurs with years of joint use. Other factors may include single or repeated injury, abnormal motion, metabolic disorders, joint infection, or another joint disorder. Effective treatment, such as pain medications (analgesics), exercises and physical therapy, and, in some cases, surgery, is available. Ligament damage is also common with aging. Ligaments, which bind joints together, tend to become less elastic as people age, making joints feel tight or stiff. This change results from chemical changes in the proteins that make up the ligaments. Consequently, most people become less flexible as they age. Ligaments tend to tear more easily, and when they tear, they heal more slowly. Older adults should have their exercise regimen reviewed by a trainer or doctor so that exercises likely to tear ligaments can be avoided. Nonsteroidal anti-inflammatory drugs (NSAIDs) that are rubbed into the skin over the affected joint may be a preferred option for older adults with osteoarthritis involving superficial joints such as the hands and knees. Less of the NSAID is absorbed than if it is taken by mouth, which minimizes the risk of side effects. Oral NSAIDs should be used for as short a period as possible given the risk of gastrointestinal bleeding and kidney dysfunction, which are increased in older adults. Acetaminophen is a reasonable alternative when oral NSAIDs cannot be taken, but acetaminophen is less effective than NSAIDs as an analgesic. More potent analgesics, such as tramadol, may occasionally be required, but doctors prescribe them only when necessary, to avoid problems with side effects and possible addiction. In addition, these medications can cause confusion in older adults. |
More Information
The following English-language resource may be useful. Please note that The Manual is not responsible for the content of this resource.
Drug Information for the Topic





