

Hypoplastic left heart syndrome consists of hypoplasia of the left ventricle and ascending aorta, maldevelopment and hypoplasia of the aortic and mitral valves (frequently aortic atresia is present), an atrial septal defect, and a patent ductus arteriosus. Unless normal closure of the patent ductus arteriosus is prevented with prostaglandin infusion, cardiogenic shock and death ensue within the first several days of life. A loud, single second heart sound (S2) and nonspecific systolic murmur are common. Diagnosis is by emergency echocardiography. Definitive treatment is staged surgical correction or heart transplantation.
(See also Overview of Congenital Cardiovascular Anomalies.)
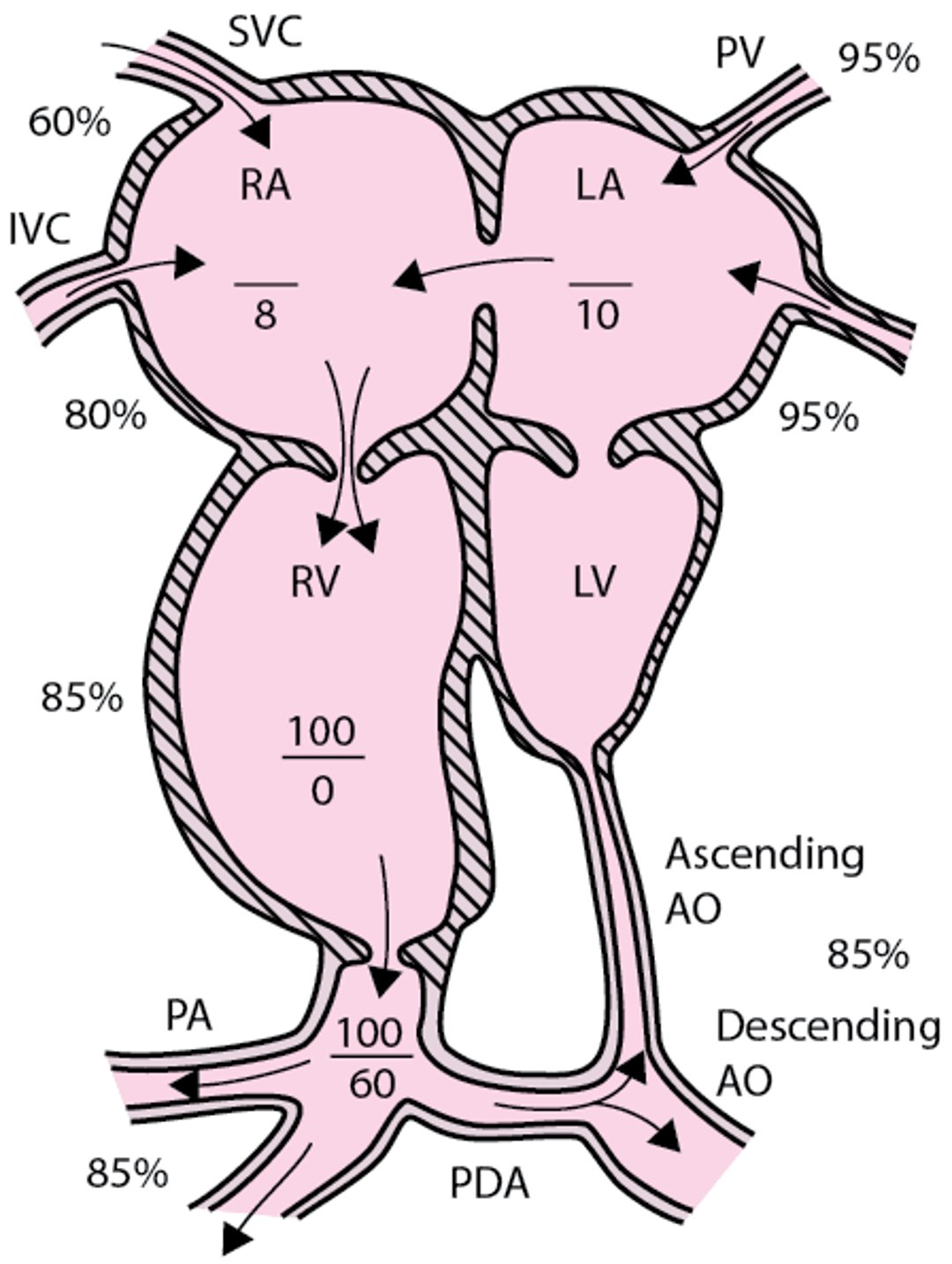
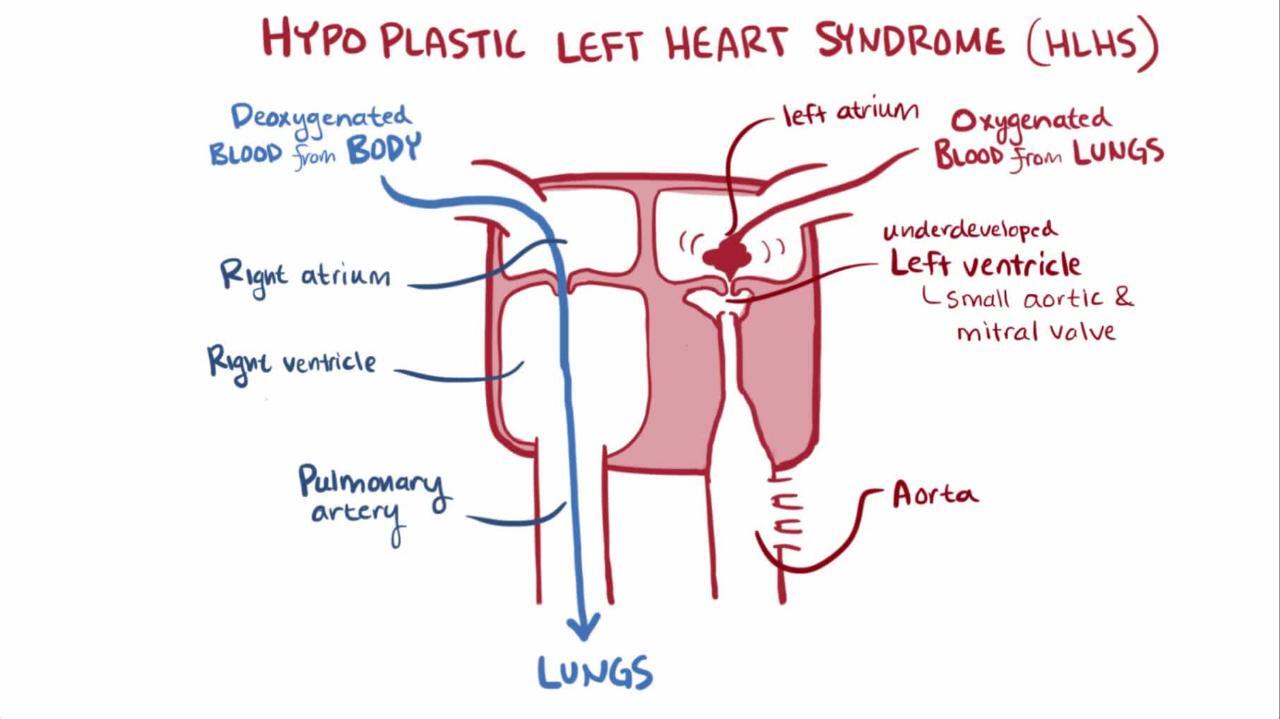
Hypoplastic left heart syndrome (HLHS) accounts for 2 to 4% of congenital heart anomalies and is the second most common left heart obstructive lesion. Because the mitral valve, left ventricle, and aortic valve are hypoplastic (often with aortic atresia), oxygenated blood coming into the left atrium from the lungs is diverted across the atrial communication into the right heart, where it mixes with desaturated systemic venous return (see figure ). This relatively desaturated blood exits the right ventricle through the pulmonary artery to the lungs and through the ductus arteriosus to the systemic circulation. Systemic blood flow is maintained only through the right-to-left ductal shunt; thus, immediate survival depends on patency of the ductus arteriosus.
Hypoplastic left heart
The left ventricle, ascending aorta, and aortic and mitral valves are hypoplastic; an atrial septal defect and a large patent ductus arteriosus are also present. AO = aorta; IVC = inferior vena cava; LA = left atrium; LV = left ventricle; PA = pulmonary artery; PDA = patent ductus arteriosus; PV = pulmonary veins; RA = right atrium; RV = right ventricle; SVC = superior vena cava. |


Symptoms and Signs of Hypoplastic Left Heart Syndrome
Symptoms of hypoplastic left heart syndrome appear when the ductus arteriosus begins to close during the first 24 to 48 hours of life. Subsequently, the clinical picture of cardiogenic shock (eg, tachypnea, dyspnea, weak pulse, pallor, cyanosis, hypothermia, metabolic acidosis, lethargy, oliguria or anuria) rapidly develops. When systemic circulation is compromised, coronary and cerebral perfusion may be reduced, leading to symptoms of myocardial or cerebral ischemia. Perfusion of the kidneys, liver, and mesentery is also inadequate, and oliguria or anuria are common. If the ductus arteriosus is not reopened, death rapidly ensues.
The patient often presents with a history of poor feeding, increased work of breathing, pale or gray coloration, and lethargy. Physical examination shows a very active precordium with a marked parasternal lift associated with very poor peripheral perfusion, cool extremities, bluish gray skin color, and absent or barely palpable pulses. The finding of a marked parasternal lift in a patient with critically low perfusion and near-absent peripheral pulses is a key to distinguishing cardiogenic shock from severe left heart obstruction and non-cardiac–related shock (eg, sepsis, metabolic, toxic). The second heart sound (S2) is loud and single. A soft, nonspecific systolic murmur is often present, as is hepatomegaly. Severe metabolic acidosis, often worsening if supplemental oxygen is administered, is characteristic of hypoplastic left heart syndrome.
Diagnosis of Hypoplastic Left Heart Syndrome
Chest x-ray and ECG
Echocardiography
Diagnosis of hypoplastic left heart syndrome is suspected clinically, particularly in neonates with metabolic acidosis that worsens after receiving oxygen; oxygen lowers pulmonary vascular resistance and thus increases the relative proportion of the right ventricle output that flows to the lungs rather than through the patent ductus arteriosus to the body. Diagnosis is confirmed by emergency echocardiography.
Pearls & Pitfalls
|
Cardiac catheterization is rarely required for diagnosis.
Chest x-ray shows cardiomegaly and pulmonary venous congestion or pulmonary edema. ECG shows right ventricular hypertrophy and diminished left ventricular forces, though it may be within normal limits for a neonate.
Treatment of Hypoplastic Left Heart Syndrome
Prostaglandin E1 (PGE1) infusion
Staged surgical repair
Sometimes heart transplantation
Fortunately, most patients with hypoplastic left heart syndrome are now diagnosed with prenatal ultrasonography or fetal echocardiography, allowing initiation of prostaglandin E1 and other appropriate therapies immediately after birth and before organ hypoperfusion can occur.
Medical management
All infants with hypoplastic left heart syndrome should be stabilized immediately in a neonatal ICU or pediatric cardiac ICU. Vascular access should be established rapidly via an umbilical venous catheter and/or peripheral IV, whichever is quicker. Prostaglandin E1 (beginning at 0.05 to 0.1 mcg/kg/minute IV) is infused to prevent closure of the ductus arteriosus or to reopen a constricted ductus. Neonates, particularly those who are critically ill at presentation, usually require tracheal intubation and mechanical ventilation. Metabolic acidosis is corrected via infusion of sodium bicarbonate. Severely ill neonates with cardiogenic shock may require inotropic drugs (eg, milrinone) and diuretics to improve cardiac function and control volume status.All infants with hypoplastic left heart syndrome should be stabilized immediately in a neonatal ICU or pediatric cardiac ICU. Vascular access should be established rapidly via an umbilical venous catheter and/or peripheral IV, whichever is quicker. Prostaglandin E1 (beginning at 0.05 to 0.1 mcg/kg/minute IV) is infused to prevent closure of the ductus arteriosus or to reopen a constricted ductus. Neonates, particularly those who are critically ill at presentation, usually require tracheal intubation and mechanical ventilation. Metabolic acidosis is corrected via infusion of sodium bicarbonate. Severely ill neonates with cardiogenic shock may require inotropic drugs (eg, milrinone) and diuretics to improve cardiac function and control volume status.
It is critical to keep pulmonary vascular resistance relatively high and systemic vascular resistance low to prevent marked pulmonary overcirculation at the expense of systemic perfusion. These resistance ranges are maintained by avoiding hyperoxia, alkalosis, and hypocarbia, all of which may lead to pulmonary vasodilation. Because oxygen is one of the most potent pulmonary vasodilators, infants are ventilated with room air or even hypoxic gas mixtures to aim for systemic saturations of 70 to 80%. If the infant requires mechanical ventilation, PCO2 can be controlled in the high normal or mildly elevated range. Systemic vascular resistance is managed by avoiding, or minimizing, the use of vasoconstricting drugs (eg, epinephrine or high-dose dopamine). Milrinone may be beneficial because it can cause systemic vasodilation. It is critical to keep pulmonary vascular resistance relatively high and systemic vascular resistance low to prevent marked pulmonary overcirculation at the expense of systemic perfusion. These resistance ranges are maintained by avoiding hyperoxia, alkalosis, and hypocarbia, all of which may lead to pulmonary vasodilation. Because oxygen is one of the most potent pulmonary vasodilators, infants are ventilated with room air or even hypoxic gas mixtures to aim for systemic saturations of 70 to 80%. If the infant requires mechanical ventilation, PCO2 can be controlled in the high normal or mildly elevated range. Systemic vascular resistance is managed by avoiding, or minimizing, the use of vasoconstricting drugs (eg, epinephrine or high-dose dopamine). Milrinone may be beneficial because it can cause systemic vasodilation.
In the uncommon circumstance of a markedly restrictive or prematurely closed patent foramen ovale, emergent transcatheter opening or enlargement of the foramen ovale may prevent imminent death.
Pearls & Pitfalls
|
Surgical procedures
Survival ultimately requires staged surgical procedures that enable the right ventricle to function as the systemic ventricle and establishing a controlled source of pulmonary blood flow.
Stage 1, done during the first week of life, is the Norwood procedure. The main pulmonary artery is divided, the distal stump is closed with a patch, and the hypoplastic aorta and proximal pulmonary artery are combined into a neoaorta. The ductus arteriosus is ligated. Pulmonary blood flow is reestablished by inserting a right-sided modified Blalock-Taussig-Thomas shunt or a right ventricular-pulmonary artery conduit (Sano modification). Finally, the atrial septal communication is enlarged.
An alternative, hybrid procedure, often a joint effort of heart surgeons and interventional cardiologists, involves inserting a stent into the ductus arteriosus (to maintain systemic blood flow) and placing bilateral branch pulmonary artery bands (to limit pulmonary blood flow). In some centers, the hybrid procedure is reserved for higher risk patients (eg, preterm or low birth weight infants, those with multisystem organ dysfunction).
Stage 2, done at 3 to 6 months of age, consists of a bidirectional Glenn or a hemi-Fontan procedure. These procedures connect the superior vena cava to the right pulmonary artery, which allows about half of the systemic venous return to bypass the right atrium and flow directly to the lungs for oxygenation. Unlike the bidirectional Glenn, the hemi-Fontan does not completely detach the superior vena cava from the right atrium.
The 3rd stage, done at 18 to 36 months, is a modified Fontan procedure, the inferior vena cava flow is diverted to the confluence of the superior vena cava and pulmonary artery. Diversion can be done via a baffle within the right atrium or by an extracardiac tube graft.
The mortality risk for children with hypoplastic left heart syndrome is highest in the first year of life (1). About 90% of patients who survive infancy will survive up to age 18. As with other children with complex congenital heart disease, survivors may have some degree of neurodevelopmental disability, which may be due to preexisting developmental abnormalities of the central nervous system (CNS) or to overt or occult CNS hypoperfusion or thromboemboli occurring during the multistage procedures.
In some infants with hypoplastic left heart syndrome, particularly those with severe tricuspid valve or ventricular dysfunction, heart transplantation is considered the procedure of choice; however, prostaglandin E1 infusion must be continued along with careful management of pulmonary and systemic vascular resistance until a donor heart is available. Because availability of donor hearts is very limited, about 20% of infants die while awaiting transplant. The 5-year survival rates after transplantation and after multistage surgery are similar. After heart transplantation, immunosuppressants are required. These drugs make patients more susceptible to infections and cause pathologic changes in the coronary arteries of the transplanted heart in a significant percentage of patients over a 5-year period. The only known treatment for allograft coronary artery disease is retransplantation.
Endocarditis prophylaxis is recommended for at least 6 months after each surgical intervention and subsequently for as long as the patient remains cyanotic or has a residual defect adjacent to a surgical patch or prosthetic material.
Treatment reference
1. Siffel C, Riehle-Colarusso T, Oster ME, et al: Survival of children with hypoplastic left heart syndrome. Pediatrics 136(4): e864–e870, 2015.
Key Points
In hypoplastic left heart syndrome, there is hypoplasia of the left ventricle and ascending aorta and maldevelopment and hypoplasia of the aortic and mitral valves; an atrial septal defect and a patent ductus arteriosus are necessary for systemic blood flow (and thus immediate survival).
Symptoms of cardiogenic shock (eg, tachypnea, dyspnea, weak pulse, pallor, cyanosis, hypothermia, metabolic acidosis, lethargy, oliguria or anuria) appear when the ductus arteriosus begins to close during the first 24 to 48 hours of life, becoming more pronounced if supplemental oxygen is given.
Initially, give PGE1 to keep the ductus arteriosus open, give as little oxygen as possible (to avoid decreasing pulmonary vascular resistance and increasing pulmonary flow at the expense of systemic flow), and avoid vasoconstrictors; give sodium bicarbonate as needed.Initially, give PGE1 to keep the ductus arteriosus open, give as little oxygen as possible (to avoid decreasing pulmonary vascular resistance and increasing pulmonary flow at the expense of systemic flow), and avoid vasoconstrictors; give sodium bicarbonate as needed.
Definitive treatment requires staged operations.
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
American Heart Association: Common Heart Defects: Provides overview of common congenital heart defects for parents and caregivers
American Heart Association: Infective Endocarditis: Provides an overview of infective endocarditis, including summarizing prophylactic antibiotic use, for patients and caregivers





