



Coma is unresponsiveness from which the patient cannot be aroused and in which the patient's eyes remain closed. Impaired consciousness refers to similar, less severe disturbances of consciousness; these disturbances are not considered coma. The mechanism for coma or impaired consciousness involves dysfunction of both cerebral hemispheres or bilateral brainstem regions containing several monoaminergic neuronal populations (also known as the ascending arousal system). Causes may be structural or nonstructural (eg, toxic or metabolic disturbances). Damage may be focal or diffuse. Diagnosis is clinical; identification of cause requires laboratory tests and neuroimaging. Treatment is immediate stabilization and specific management of the cause. For long-term disorders of consciousness, adjunctive treatment includes passive range-of-motion exercises, enteral feedings, and measures to prevent pressure ulcers.
Decreased or impaired consciousness or alertness refers to decreased responsiveness to external stimuli. Severe impairment includes
Coma: The patient cannot be aroused, and the eyes are closed and do not open in response to any stimulation.
Vegetative State/Unresponsive Wakefulness: The patient remains fully unresponsive with some periods of spontaneous eye opening during the day.
Minimally Conscious State: The patient shows reliable but intermittent evidence of conscious behavioral responses but does not demonstrate functional communication.
Stupor: The patient can be awakened only by vigorous physical stimulation.
Less severely impaired levels of consciousness are often labeled as lethargy or, if more severe, obtundation. Lethargy usually involves fatigue and a lack of energy. Obtundation is a reduced level of alertness or consciousness. However, differentiation between less severely impaired levels is often imprecise; the label is less important than a precise clinical description (eg, “the best level of response is short sentences spoken after sitting up with mild stimulation of the sternum”).
Delirium is marked by fluctuation in cognitive disturbances (primarily in attention, but also specific domains of cognition, and/or level of consciousness) and typically indicates metabolic disturbance due to an acute clinical problem (eg, infection, blood loss). Patients with delirium may have alternating periods of appropriate attention and cognition and periods of impaired attention and cognition with agitation or marked underactivation (hypoactive delirium).
Delirium is typically considered an acute loss of prior mental function. However, features consistent with those found in acute delirium may be seen in patients with stable chronic impairment after structural brain injuries (known as "confusional state" and sometimes included within the grouping of disorders of consciousness).
Pathophysiology of Coma and Impaired Consciousness
Maintaining alertness requires intact function of the cerebral hemispheres and preservation of the brain stem arousal system, sometimes referred to as the reticular activating system. This system is comprised of a collection of interconnected distinct nuclei that feed back upon each other (typically signaling via monoamines). These nuclei are located in the upper pons, midbrain, basal forebrain, and hypothalamus; most project to both the cortex and the central regions of the thalamus.
Impaired consciousness requires bilateral dysfunction, either in both cerebral hemispheres or in the arousal system (1, 2). Unilateral cerebral hemisphere disorders are not sufficient to impair consciousness, although they may cause severe neurologic deficits. Rarely, however, a unilateral massive hemispheric focal lesion (eg, left middle cerebral artery stroke) impairs consciousness if the contralateral hemisphere is already compromised or if it results in compression of the contralateral hemisphere (eg, by causing edema).
Dysfunction of the brain stem arousal system can result from conditions that have diffuse effects, such as toxic or metabolic disturbances (eg, hypoglycemia, hypoxia, uremia, overdose of a substance, illicit drug, or medication). Dysfunction can also be caused by focal ischemia (eg, certain upper brain stem infarcts), hemorrhage, or direct mechanical disruption.
Any condition that increases intracranial pressure (ICP) may decrease cerebral perfusion pressure, resulting in secondary brain ischemia. Secondary brain ischemia may affect the brain stem or both cerebral hemispheres, impairing consciousness.
When brain damage is extensive, brain herniation (see also figure and table ) may occur. Neurologic deterioration due to brain herniation may result from the following mechanisms:
Direct compression of brain tissue
Decreased blood supply to areas of the brain
Increased ICP
Obstruction of the cerebral ventricular system causing hydrocephalus
Neuronal and vascular cell dysfunction
Shift of brain structures from one side to the other
In addition to the direct effects of increased ICP on neuronal and vascular cells, cellular pathways of apoptosis and autophagy (forms of programmed cell death or destruction) can become activated by ICP, although these most commonly occur in anoxic brain injury and hypoxic ischemic injuries. Apoptosis leads to the destruction of cellular deoxyribonucleic acid (DNA). In autophagy, components of neuronal and vascular cell cytoplasm are recycled in an attempt to remove nonfunctional organelles (3). Additional pathways tied to apoptosis and autophagy involve circadian clock genes that oversee daily cellular function (4). Circadian clock gene pathways control brain cell survival and death through apoptosis and autophagy. They also oversee multiple systems that involve brain blood flow, oxygenation, and metabolism, which can affect the patient's prognosis for coma.
Impaired consciousness may progress to coma and ultimately to brain death.
Pathophysiology references
1. Giacino JT, Katz DI, Schiff ND, et al. Practice guideline update recommendations summary: Disorders of consciousness: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology; the American Congress of Rehabilitation Medicine; and the National Institute on Disability, Independent Living, and Rehabilitation Research. Neurology. 2018;91(10):450-460. doi:10.1212/WNL.0000000000005926
2. Posner J, Saper C, Schiff ND, Claassen J. Plum and Posner's Diagnosis and Treatment of Stupor and Coma 5th Edition. Oxford University Press; 2019.
3. Maiese K, Chong ZZ, Shang YC, Wang S. Targeting disease through novel pathways of apoptosis and autophagy. Expert Opin Ther Targets. 2012;16(12):1203-1214. doi:10.1517/14728222.2012.719499
4. Maiese K. Cognitive impairment and dementia: Gaining insight through circadian clock gene pathways. Biomolecules. 2021; 11(7):1002. doi: 10.3390/biom11071002
Etiology of Coma and Impaired Consciousness
Coma or impaired consciousness may result from structural disorders, which typically cause focal damage, or nonstructural disorders, which most often cause diffuse impairment of cerebral tissue (see table ).
Older age increases the risk of impaired consciousness.
Common Causes of Coma or Impaired Consciousness
Cause | Examples |
|---|---|
Focal | |
Structural disorders | Head trauma (eg, concussion, cerebral lacerations or contusions, epidural or subdural hematoma) Hydrocephalus (acute) Intraparenchymal hemorrhage Cortex or upper brain stem infarct or hemorrhage |
Nonstructural disorders | Seizures (eg, nonconvulsive status epilepticus) or a postictal state caused by an epileptogenic focus |
Diffuse | |
Metabolic, hypoxic or ischemic, and endocrine disorders | Hypercapnia Hyperglycemia Hypocalcemia (rarely) Hypoxia/ischemia Respiratory failure or heart failure Uremia |
Infections | Coronavirus disease 2019 (COVID-19) Severe acute respiratory coronavirus 2 (SARS-CoV2) Other infections including bacterial, viral, and parasitic |
Other disorders | Diffuse axonal injury Hypertensive encephalopathy |
Medications and illicit drugs | Anesthetics (eg, propofol) Antipsychotic medications if they cause neuroleptic malignant syndrome CNS stimulants (eg, cocaine) Opioid and related analgesics Other CNS depressants Selective serotonin reuptake inhibitors if they cause release of excess serotonin (serotonin syndrome) |
Toxins | |
CNS = central nervous system. | |
Psychiatric disorders (eg, psychogenic unresponsiveness) can mimic impaired consciousness, are volitional, and can be distinguished from true impaired consciousness by neurologic examination.
Symptoms and Signs of Coma and Impaired Consciousness
Consciousness is decreased to varying degrees. Repeated stimuli arouse patients only briefly or not at all.
Depending on the cause, other symptoms develop (see table ):
Eye abnormalities: Pupils may be dilated, pinpoint, or unequal. One or both pupils may be fixed in midposition. Eye movement may be dysconjugate or absent (oculomotor paresis) or involve unusual patterns (eg, ocular bobbing, ocular dipping, opsoclonus). Homonymous hemianopia (visual field loss on the same side in both eyes) may be present. Other abnormalities include loss of normal ocular reflexes: blinking in response to visual threat (almost touching the eye), the oculocephalic reflex (eye movement with head rotation), the oculovestibular reflex (eye movement with caloric stimulation), and corneal reflexes.
Autonomic dysfunction: Patients may have abnormal breathing patterns (Cheyne-Stokes or Biot respirations), sometimes with hypertension and bradycardia (Cushing reflex). Respiratory arrest and cardiac arrest may occur. Hypotension may occur if impaired consciousness is caused by severe infection, severe dehydration, major blood loss, or cardiac arrest.
Motor dysfunction: Abnormalities include flaccidity, hemiparesis, asterixis, multifocal myoclonus, decorticate posturing (elbow flexion and shoulder adduction with leg extension), and decerebrate posturing (limb extension and internal shoulder rotation).
Other symptoms: If the brain stem is compromised, nausea, vomiting, meningismus, occipital headache, ataxia, and increasing somnolence can occur.
Findings by Location*
Location | Abnormal Findings |
|---|---|
Bilateral hemispheric damage or dysfunction* | Symmetric tone and response (flexor or extensor) to pain Myoclonus (possible) Periodic cycling of breathing |
Supratentorial mass compressing the brain stem | Ipsilateral third cranial nerve palsy with unilateral dilated, fixed pupil and oculomotor paresis Sometimes contralateral homonymous hemianopia and absent blinking response to visual threat Contralateral hemiparesis |
Brain stem lesion | Early abnormal pupillary and oculomotor signs Abnormal oculocephalic reflex Abnormal oculovestibular reflex Asymmetrical motor responses Decorticate rigidity (usually due to an upper brain stem lesion) or decerebrate rigidity (usually due to a bilateral midbrain or pontine lesion) Hyperventilation (due to a midbrain or upper pontine lesion) |
Midbrain (upper brain stem) lesion | Pupils locked in midposition, often unequal in size, with loss of light reflexes (due to a structural or metabolic disorder that causes loss of both sympathetic and parasympathetic pupillary tone) |
Toxic-metabolic dysfunction | Spontaneous, conjugate roving eye movements in mild coma Fixed eye position in deeper coma Abnormal oculovestibular reflex Multifocal myoclonus Asterixis (may be considered a type of negative myoclonus) Decorticate and decerebrate rigidity or flaccidity |
* Not all of the findings occur in all cases. Brain stem reflexes and pupillary light responses may be intact in patients with bilateral hemispheric damage or dysfunction or toxic-metabolic dysfunction; however, hypothermia, sedative overdose, or use of an anesthetic can cause partial loss of brain stem reflexes. | |
Diagnosis of Coma and Impaired Consciousness
History
General physical examination
Neurologic examination, including eye examination
Laboratory tests (eg, pulse oximetry, bedside glucose measurement, blood and urine tests)
Immediate neuroimaging
Sometimes measurement of ICP
If diagnosis is unclear, lumbar puncture or electroencephalography (EEG)
Impaired consciousness is diagnosed if repeated stimuli arouse patients only briefly or not at all. If stimulation triggers primitive reflex movements (eg, decerebrate or decorticate posturing), impaired consciousness may be deepening into coma.
Diagnosis and initial stabilization (airway, breathing, and circulation) should occur simultaneously (1) . Temperature is measured to check for hypothermia or hyperthermia; if either is present, treatment is started immediately. Glucose levels are measured at the bedside to identify low levels, which should also be corrected immediately. If trauma is involved, the neck is immobilized until clinical history, physical examination, or imaging tests exclude an unstable injury and damage to the cervical spine. If drug overdose is a possibility, reversal agents (including naloxone for opioid overdose and flumazenil for benzodiazepine overdose) should be administered.
History
Medical identification bracelets or the contents of a wallet or purse (eg, hospital identification card, medications list) may provide clues to the cause. Caregivers, paramedics, police officers, and any witnesses should be questioned about the circumstances and environment in which the patient was found; containers that may have held food, alcohol, medications, or poisons should be examined and saved for identification (eg, substance identification aided by a poison center) and possible chemical analysis.
Caregivers should be asked about the following:
The onset and time course of the problem (eg, whether seizure, headache, vomiting, head trauma, or ingestion of an illicit drug, medication, or other substance was observed; how quickly symptoms appeared; whether the course has been progressive or waxing and waning)
Baseline mental status
Recent infections and possible exposure to infections
Other previous and concurrent systemic illnesses, including new-onset heart failure, arrhythmias, respiratory disorders, and metabolic, liver, or kidney disorders
Recent travel
Ingestions of unusual meals
Psychiatric problems and symptoms
Prescription medication history
Use of alcohol or illicit drugs (eg, anesthetics, stimulants, depressants)
The last time the patient was at their baseline mental status
Any hunches they may have about what might be the cause (eg, possible occult overdose, possible occult head trauma due to recent intoxication)
Medical records should be reviewed if available.
General physical examination
Physical examination should be focused and efficient and should include thorough examination of the head and face, skin, and extremities. Examination of the heart and lungs is important to assess blood flow and oxygenation to the brain.
Signs of head trauma include (raccoon eyes), (Battle sign), , instability of the maxilla, and cerebrospinal fluid (CSF) rhinorrhea and otorrhea. Scalp contusions and small bullet holes can be missed unless the head is carefully inspected.
If unstable injury and cervical spine damage have been excluded, passive neck flexion is done; passive neck flexion is strictly contraindicated in suspected acute cervical spine trauma, ligamentous instability, or patients with known structural abnormalities resulting from tumors or infectious processes Stiffness when the neck is flexed suggests subarachnoid hemorrhage or meningitis.
Findings from the physical examination may suggest a cause:
Hypothermia: Environmental exposure, drowning, sedative overdose, severe hypothyroidism, Wernicke encephalopathy, or, in older adults, sepsis
Hyperthermia: Heatstroke, infection, stimulant overdose, or neuroleptic malignant syndrome
Fever, petechial or purpuric rash, hypotension, or severe extremity infections (eg, gangrene of 1 or more toes): Sepsis or central nervous system (CNS) infection
Needle marks: Overdose of a medication (eg, insulin) or an illicit drug (eg, opioids)
A bitten tongue: Seizure
Breath odor: Toxicity due to alcohol or another substance, or diabetic ketoacidosis
Hypotension or pulse abnormalities: Cardiac dysfunction with hypoperfusion
Difficulty breathing: Acute respiratory dysfunction
Neurologic examination
The neurologic examination determines whether the brain stem is intact and location of a lesion within the CNS, if a lesion (eg tumor, abscess, bleed) is present. The examination focuses on the following:
Level of consciousness
Eyes
Motor function
Deep tendon reflexes
Level of consciousness is evaluated by attempting to wake patients first with verbal commands, then with nonnoxious stimuli (eg, clapping of hands), and finally (if necessary) with noxious stimuli (eg, pressure to the supraorbital ridge, nail bed, or sternum).
The Glasgow Coma Scale (see table ) was developed to assess patients with head trauma. For head trauma, the score assigned by the scale has prognostic value. For patients with coma or impaired consciousness of any cause, the scale is a relatively reliable, objective measure of the severity of unresponsiveness and can be used serially for monitoring. The scale assigns points based on responses to oculomotor, verbal, and motor responses. Once transition from coma into a vegetative or minimally conscious state is observed, measurements should shift to the Coma Recovery Scale–Revised (1, 2, 3).
Eye opening, facial grimacing, and purposeful withdrawal of limbs from a noxious stimulus indicate that consciousness is not greatly impaired. Asymmetric motor responses to pain or deep tendon reflexes may indicate a focal hemispheric lesion.
Glasgow Coma Scale*
Area Assessed | Response | Points |
|---|---|---|
Eye opening | Open spontaneously; open with blinking at baseline | 4 |
Open to verbal command, speech, or shout | 3 | |
Open in response to pain applied to the limbs or sternum | 2 | |
None | 1 | |
Verbal | Oriented | 5 |
Confused conversation but able to answer questions | 4 | |
Inappropriate responses; words discernible | 3 | |
Incomprehensible speech | 2 | |
None | 1 | |
Motor | Obeys commands for movement | 6 |
Responds to pain with purposeful movement | 5 | |
Withdraws from pain stimuli | 4 | |
Responds to pain with abnormal flexion (decorticate posturing) | 3 | |
Responds to pain with abnormal extension (decerebrate posturing) | 2 | |
None | 1 | |
* Combined scores < 8 are typically regarded as coma. | ||
Adapted from Teasdale G, Jennett B: Assessment of coma and impaired consciousness. A practical scale. Lancet. 2:81–84; 1974. | ||
As impaired consciousness deepens into coma, noxious stimuli may trigger stereotypic reflex posturing.
Decorticate posturing can occur in structural or metabolic disorders and indicates hemispheric damage with preservation of motor centers in the upper portion of the brain stem (eg, rubrospinal tract).
Decerebrate posturing indicates that the upper brain stem motor centers, which facilitate flexion, have been structurally damaged and that only the lower brain stem centers (eg, vestibulospinal tract, reticulospinal tract), which facilitate extension, are responding to sensory stimuli.
Decerebrate posturing may also occur, although less often, in diffuse disorders such as anoxic encephalopathy.
Flaccidity without movement is the worst possible motor response and indicates that the lower brain stem is not affecting movement, regardless of whether the spinal cord is damaged.
Asterixis and multifocal myoclonus suggest metabolic disorders such as uremia, hepatic encephalopathy, hypoxic encephalopathy, and drug toxicity.
Physical examination can distinguish psychogenic unresponsiveness from physiologically impaired consciousness. Although voluntary motor response is typically absent in psychogenic unresponsiveness, muscle tone and deep tendon reflexes remain normal, and all brain stem reflexes are preserved. Vital signs are usually not affected.

Eye examination
The following are evaluated:
Pupillary responses
Extraocular movements
Fundi
Other neuro-ophthalmic reflexes
Pupillary responses and extraocular movements provide information about brain stem function (see table ). In coma due to structural lesions, one or both pupils usually become fixed early. When coma is due to diffuse metabolic disorders (toxic-metabolic encephalopathy), pupillary responses are often preserved until very late, although responses may be sluggish. If only one pupil is dilated, other causes of anisocoria should be considered, including past ocular trauma, certain types of headache, and use of a scopolamine patch (if scopolamine comes in contact with the eyes).
Interpretation of Pupillary Response and Eye Movements
Area Assessed | Finding | Interpretation |
|---|---|---|
Pupils | Sluggish light reactivity retained until all other brain stem reflexes are lost | Diffuse cellular cerebral dysfunction (toxic-metabolic encephalopathy) |
Unilateral pupillary dilation, pupil unreactive to light | Third cranial nerve compression (eg, in transtentorial herniation), usually due to an ipsilateral lesion (see Anisocoria) | |
Pupils fixed in midposition | Midbrain dysfunction due to structural damage (eg, infarction, hemorrhage) Central herniation Severe metabolic depression by medications, illicit drugs, or toxins (all other brain stem reflexes are also absent) | |
Constricted pupils (1 mm wide) | Massive pontine hemorrhage Toxicity due to opioids or certain insecticides (eg, organophosphates, carbamates) | |
Eye movements | Early abnormal pupillary and oculomotor signs | Primary brain stem lesion |
Spontaneous, conjugate roving eye movements but intact brain stem reflexes | Early toxic-metabolic encephalopathy | |
Gaze preference to one side | Brain stem lesion on the opposite side Cerebral hemisphere lesion on the same side | |
Absent eye movements | Further testing required (eg, oculocephalic and oculovestibular reflexes) Possibly toxicity due to phenobarbital or phenytoin, Wernicke encephalopathy, botulism, or brain death |
The fundi should be examined. Papilledema, usually bilateral, may indicate increased ICP but may take many hours to appear. Increased ICP can cause earlier changes in the fundi, such as loss of retinal venous pulsations, disc hypermia, dilated capillaries, blurring of the medial disc margins, and sometimes hemorrhages. Subhyaloid hemorrhage may indicate subarachnoid hemorrhage.
The oculocephalic reflex is tested by the doll’s-eye maneuver in unresponsive patients: The eyes are observed while the head is passively rotated from side to side or flexed and extended. This maneuver should not be attempted if cervical spine instability is suspected.
If the reflex is present, the maneuver causes the eyes to move in the opposite direction of head rotation, flexion, or extension, indicating that the oculovestibular pathways in the brain stem are intact. Thus, in a supine patient, the eyes continue to look straight up when the head is turned side to side.
If the reflex is absent, the eyes do not move and thus point in whatever direction the head is turned, indicating the oculovestibular pathways are disrupted. The reflex is also absent in most patients with psychogenic unresponsiveness because visual fixation is conscious.
If the patient is unconscious and the oculocephalic reflex is absent or the neck is immobilized, oculovestibular (cold caloric) testing is done. After integrity of the tympanic membrane is confirmed, the patient’s head is elevated 30°, and with a syringe connected to a flexible catheter, the examiner irrigates the external auditory canal with 50 mL of ice water over a 30-second period.
If both eyes deviate toward the irrigated ear, the brain stem reflex is functioning normally, suggesting mildly impaired consciousness.
If nystagmus away from the irrigated ear also occurs, the patient is conscious and psychogenic unresponsiveness is likely. In conscious patients, 1 mL of ice water is often enough to induce ocular deviation and nystagmus. Thus, if psychogenic unresponsiveness is suspected, a small amount of water should be used (or caloric testing should not be done) because cold caloric testing can induce severe vertigo, nausea, and vomiting in conscious patients.
If the eyes do not move or movement is dysconjugate after irrigation, the integrity of the brain stem is uncertain and the coma is deeper.
Pearls & Pitfalls
|
Certain patterns of eye abnormalities and other findings may suggest brain herniation (see also figure and table ).
Respiratory patterns
The spontaneous respiratory rate and pattern should be documented unless emergency airway intervention is required. It may suggest a cause.
Periodic cycling of breathing (Cheyne-Stokes or Biot respiration) may indicate dysfunction of both cerebral hemispheres or of the diencephalon.
Hyperventilation (central neurogenic hyperventilation) with respiratory rate > 25 breaths/minute may indicate midbrain or upper pontine dysfunction.
An inspiratory gasp with respiratory pauses of about 3 seconds after full inspiration (apneustic breathing) typically indicates pontine or medullary lesions; this type of breathing often progresses to respiratory arrest.
Testing
Initially, pulse oximetry, fingerstick plasma glucose measurements, and cardiac monitoring are done. If the cause is not immediately clear, further testing is done.
Blood tests should include a comprehensive metabolic panel (including at least serum electrolytes, blood urea nitrogen [BUN], creatinine, and calcium levels), complete blood count (CBC) with differential and platelets, liver tests, and ammonia level.
Arterial blood gases (ABGs) are measured, and if carbon monoxide toxicity is suspected, carboxyhemoglobin level is measured.
Blood and urine should be obtained for culture and routine toxicology screening; serum ethanol level is also measured. Other toxicology screening panels and additional toxicology tests (eg, serum drug levels) are done based on clinical suspicion.
ECG (12-lead) is also done to check for myocardial infarction and arrhythmias.
Chest radiograph should be done to check for new lung disease that may affect brain oxygenation.
If the cause is still not immediately apparent, noncontrast head CT should be done as soon as possible to check for masses, hemorrhage, edema, evidence of bone trauma, and hydrocephalus. Initially, Noncontrast CT, rather than contrast CT, is preferred as the initial exam to exclude brain hemorrhage; CT detects cerebral bleeding and bone injuries (eg, skull fractures) best within 72 hours of injury. Alternatively, MRI can be done if immediately available, but it is not as quick as newer-generation CT scanners and may not be as sensitive for traumatic bone injuries. MRI is now as sensitive as CT for detecting blood early as well as late. If noncontrast CT is not diagnostic, MRI or contrast CT can then be done; either may detect isodense subdural hematomas, multiple metastases, sagittal sinus thrombosis, herpes encephalitis, or other causes missed by noncontrast CT. MRI provides greater detail than CT when done > 72 hours after symptom onset, but logistically, MRI is difficult if the patient is intubated.

Classic lentiform (lens)-shaped hyperdensity that does not extend across suture lines.
Classic lentiform (lens)-shaped hyperdensity that does not extend across suture lines.
© 2017 Elliot K. Fishman, MD.


Classic lentiform (lens)-shaped hyperdensity that does not extend across suture lines.
Classic lentiform (lens)-shaped hyperdensity that does not extend across suture lines.
© 2017 Elliot K. Fishman, MD.

Classic crescent-shaped hyperdensity extending across suture lines.
Classic crescent-shaped hyperdensity extending across suture lines.
© 2017 Elliot K. Fishman, MD.

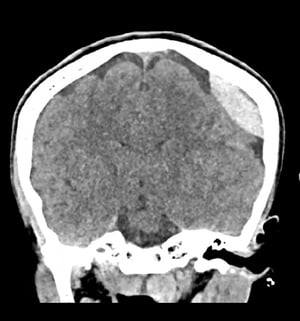
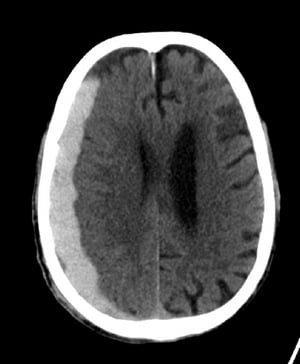
Subfalcine herniation is the most common type of cerebral herniation. In this image, the left brain has herniated under the free edge of the falx cerebri (arrow) because hemorrhage from an infarct in the middle cerebral artery has increased intracerebral pressure.
Subfalcine herniation is the most common type of cerebral herniation. In this image, the left brain has herniated under
© 2017 Elliot K. Fishman, MD.
Classic lentiform (lens)-shaped hyperdensity that does not extend across suture lines.
Classic lentiform (lens)-shaped hyperdensity that does not extend across suture lines.
© 2017 Elliot K. Fishman, MD.
Classic lentiform (lens)-shaped hyperdensity that does not extend across suture lines.
Classic lentiform (lens)-shaped hyperdensity that does not extend across suture lines.
© 2017 Elliot K. Fishman, MD.
Classic crescent-shaped hyperdensity extending across suture lines.
Classic crescent-shaped hyperdensity extending across suture lines.
© 2017 Elliot K. Fishman, MD.
Subfalcine herniation is the most common type of cerebral herniation. In this image, the left brain has herniated under the free edge of the falx cerebri (arrow) because hemorrhage from an infarct in the middle cerebral artery has increased intracerebral pressure.
Subfalcine herniation is the most common type of cerebral herniation. In this image, the left brain has herniated under
© 2017 Elliot K. Fishman, MD.
If coma is unexplained after MRI or CT and other tests, lumbar puncture (spinal tap) is done to check opening pressure and to exclude infection, subarachnoid hemorrhage, and other abnormalities. Prior to lumbar puncture, MRI or CT images should be reviewed for abnormalities that would contraindicate lumbar puncture: intracranial masses, obstructive hydrocephalus, and other abnormalities that could obstruct CSF flow or the ventricular system and thus significantly increase ICP. Suddenly lowering CSF pressure, as can occur during lumbar puncture in patients with increased ICP, could trigger brain herniation; however, this outcome is uncommon.
CSF analysis includes cell and differential counts, protein, glucose, Gram staining, cultures and, based on clinical suspicion, specific tests (eg, cryptococcal antigen test, cytology, measurement of tumor markers, Venereal Disease Research Laboratory [VDRL] tests, polymerase chain reaction [PCR] for herpes simplex, visual or spectrophotometric analysis for xanthochromia).
In settings where lumbar puncture is contraindicated because of suspected increased ICP (eg, the patient is exhibiting clinical or radiographic signs of a mass effect and is at risk for central herniation), obstructive hydrocephalus, or unusual conditions such a diffuse leptomeningeal carcinomatosis, CSF pressure is directly measured (4). If ICP is increased, continuous ICP monitoring is done and measures to decrease the ICP are taken.
If seizures may be the cause of coma, particularly if nonconvulsive status epilepticus (recurrent seizures without prominent motor symptoms) is possible or if the diagnosis remains uncertain, EEG may be done. In most comatose patients, EEG shows slowing and reductions in wave amplitude; such findings are nonspecific but often occur in toxic-metabolic encephalopathy. In some patients with nonconvulsive status epilepticus, the EEG may show a combination of spikes, sharp waves, or spike and slow complexes (5). If psychogenic unresponsiveness or seizure activity (pseudoseizure) that results from a behavior disorder is possible, video EEG monitoring can differentiate pseudoseizure from nonconvulsive seizures or eliminate uncertainty; if a clear psychiatric history or examination feature make psychogenic unresponsiveness highly likely, video EEG monitoring is not required but it remains the diagnostic standard (6).
A history of recent travel to selected locations with endemic diseases should prompt testing for bacterial, viral, and parasitic infections that may lead to coma.
Clinicians can consider evoked potentials such as brain stem auditory evoked potentials to assess brain stem function or somatosensory evoked potentials to assess the cortex, thalamic, brain stem, and spinal cord pathways (eg, after cardiac arrest).
Diagnosis references
1. Giacino JT, Katz DI, Schiff ND, et al. Practice guideline update recommendations summary: Disorders of consciousness: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology; the American Congress of Rehabilitation Medicine; and the National Institute on Disability, Independent Living, and Rehabilitation Research. Neurology. 2018;91(10):450-460. doi:10.1212/WNL.0000000000005926
2. Giacino JT, Kalmar K, Whyte J. The JFK Coma Recovery Scale-Revised: measurement characteristics and diagnostic utility. Arch Phys Med Rehabil. 2004;85(12):2020-2029. doi:10.1016/j.apmr.2004.02.033
3. Bodien YG, Vora I, Barra A, et al. Feasibility and Validity of the Coma Recovery Scale-Revised for Accelerated Standardized Testing: A Practical Assessment Tool for Detecting Consciousness in the Intensive Care Unit. Ann Neurol. 2023;94(5):919-924. doi:10.1002/ana.26740
4. Le Roux P, Menon DK, Citerio G, et al. Consensus summary statement of the International Multidisciplinary Consensus Conference on Multimodality Monitoring in Neurocritical Care: a statement for healthcare professionals from the Neurocritical Care Society and the European Society of Intensive Care Medicine. Neurocrit Care. 2014;21 Suppl 2(Suppl 2):S1-S26. doi:10.1007/s12028-014-0041-5
5. Zafar A, Aljaafari D. EEG criteria for diagnosing nonconvulsive status epilepticus in comatose - An unsolved puzzle: A narrative review. Heliyon. 2023 Nov 17;9(11):e22393. doi: 10.1016/j.heliyon.2023.e22393
6. LaFrance WC Jr, Baker GA, Duncan R, Goldstein LH, Reuber M. Minimum requirements for the diagnosis of psychogenic nonepileptic seizures: a staged approach: a report from the International League Against Epilepsy Nonepileptic Seizures Task Force. Epilepsia. 2013;54(11):2005-2018. doi:10.1111/epi.12356
Treatment of Coma and Impaired Consciousness
Immediate stabilization (airway, breathing, circulation, or ABCs)
Admission to an intensive care unit (ICU)
Supportive measures, including control of ICP if present
Treatment of underlying disorder
Airway, breathing, and circulation must be ensured immediately. Patients with impaired consciousness are admitted to the ICU so that respiratory and neurologic status can be monitored. Hypotension must be corrected. If hypertension is present, blood pressure should be reduced carefully; lowering blood pressure below the patient's usual level can lead to brain ischemia.
Because some patients in coma are undernourished and susceptible to Wernicke encephalopathy, thiamine 100 mg IV or IM should be given routinely. If plasma glucose is low, patients should be given 50 mL of 50% dextrose IV, but only after they have been given thiamine.
If trauma is involved, the neck is immobilized until CT is done to exclude damage to the cervical spine.
Neurostimulant medications have been used in patients in a stupor or coma in the acute setting after head trauma with evidence of some treatment benefit (1). Multidisciplinary guidelines specifically recommend amantadine for 4 weeks of treatment after TBI to hasten functional recovery (1).
If opioid overdose is suspected, naloxone 0.4 to 2 mg IV is given and repeated as necessary. If benzodiazepine overdose is suspected, flumazenil 0.2 mg IV is given for 30 seconds, with additional doses up to cumulative dose of 3 mg as needed.
If a recent (within about 1 hour) overdose of life-threatening volumes of certain medications (eg, proarrhythmic or hypotensive agents) or other substances (particularly toxins not effectively neutralized or bound by activated charcoal or similar agents such as elemental metals) is possible, gastric lavage (with airway protection) can be done through a large-bore orogastric tube (eg, ≥ 32 Fr) after endotracheal intubation; however, gastric lavage is now done only rarely.
Coexisting disorders and abnormalities are treated as indicated. For example, metabolic abnormalities are corrected. Core body temperature may need to be corrected (eg, cooling for severe hyperthermia, warming for hypothermia).
Endotracheal intubation
Endotracheal intubation is indicated for comatose patients with:
Respiratory distress
Hypoxia not responsive to supplemental oxygen provided
Elevated ICP
Seizure
Vomiting
Hemodynamic instability or shock
In a randomized trial, routine intubation in comatose patients without the above indications and with suspected overdose resulted in prolonged hospital and ICU stays and increased in-hospital death (2).
However, in a randomized trial of comatose patients with suspected overdose, withholding intubation (except when respiratory distress, seizure, vomiting, or shock was present) resulted in lower rates of in-hospital death and shorter hospital and ICU stays (2).
When done for suspected increased ICP, intubation should be done via rapid-sequence oral intubation (using a paralytic medication, typically succinylcholine) rather than via nasotracheal intubation; nasotracheal intubation in a patient who is breathing spontaneously causes coughing and gagging, thus increasing ICP.
To minimize the increase in ICP that may occur when the airway is manipulated, some clinicians recommend giving lidocaine 1.5 mg/kg IV 1 to 2 minutes before giving the paralytic to prevent increases in heart rate, cardiac output, and systolic blood pressure (3). Patients are sedated before the paralytic is given. Etomidate has minimal effects on blood pressure and thus is a good anesthetic choice in hypotensive or trauma patients; alternatively, propofol may be used if hypotension is absent.
Paralytics should be used only when they are deemed necessary for intubation. If the patient has no spontaneous respiration and nasotracheal intubation is appropriate, paralytics should be avoided. Rarely, succinylcholine can lead to malignant hyperthermia and also can mask changes in neurologic function. It must be emphasized that if paralytics are used with intubation, post-intubation sedation is required: studies identify a significant prevalence (approximately 5%) of awareness in the emergency setting with use of neuromuscular blockade agents (4).
Pulse oximetry and ABGs (if possible, end-tidal CO2) should be used to assess adequacy of oxygenation and ventilation.
Intracranial pressure control
If intracranial pressure (ICP) is increased, clinicians should monitor intracranial and cerebral perfusion pressure, and pressures should be controlled. The goal is to maintain ICP at ≤ 20 mm Hg and cerebral perfusion pressure at 50 to 70 mm Hg. ICP is usually lower in children than in adults. In neonates, ICP can be below the atmospheric pressure. Thus, children are evaluated independently from adult guidelines.
Control of increased ICP involves several strategies (5):
Sedation: Sedatives may be necessary to control agitation, excessive muscular activity (eg, due to delirium), or pain, which can increase ICP. However, because sedatives can mask neurologic findings, their use should be minimized and avoided whenever possible.
Propofol is often used in adults (contraindicated in children) because its onset and duration of action are quick. The most common adverse effect is hypotension. Prolonged use at high doses can cause pancreatitis or, rarely, propofol infusion syndrome (6). Benzodiazepines (eg, midazolam, lorazepam) can also be used. Antipsychotics should be avoided if possible because they can delay recovery.
Sedatives are not used to treat agitation and delirium due to hypoxia; oxygen is used instead.
Hyperventilation: Hyperventilation causes hypocapnia, which causes vasoconstriction, thus decreasing cerebral blood flow globally. Reduction in PCO2 from 40 mm Hg to 30 mm Hg can reduce ICP about 30%. However, hyperventilation decreases ICP for only about 30 minutes and thus is used as a temporary measure until other treatments take effect. Aggressive hyperventilation to < 25 mm Hg should be avoided because it may reduce cerebral blood flow excessively and result in cerebral ischemia.
Hydration: Isotonic fluids are used. Providing free water through IV fluids (eg, 5% dextrose, 0.45% saline) should be avoided since hypotonic fluids can aggravate cerebral edema. Patients should be kept euvolemic. If patients have no signs of dehydration or fluid overload, IV fluids with normal saline can be started at 50 to 75 mL/hour with the rate adjusted based on serum sodium, osmolality, urine output, and signs of fluid retention (eg, edema).
Diuretics: Serum osmolality should be kept at 295 to 320 mOsm/kg. For selected patients, osmotic diuretics (eg, mannitol) may be given IV to lower ICP and maintain serum osmolality. They should be reserved for patients whose condition is deteriorating (eg, those with acute brain herniation) or used preoperatively for patients with hematomas. Since osmotic diuretics do not cross the blood-brain barrier, they pull water from brain tissue across an osmotic gradient into plasma, eventually leading to equilibrium. However, the effectiveness of these diuretics decreases after a few hours. Mannitol must be used cautiously in patients with severe coronary artery disease, heart failure, renal insufficiency, or pulmonary vascular congestion because mannitol rapidly expands intravascular volume. Because osmotic diuretics increase renal excretion of water relative to sodium, prolonged use may result in water depletion and hypernatremia. Fluid and electrolyte balance should be monitored closely while osmotic diuretics are used. A 3% saline solution is often used as an alternative osmotic agent to control ICP (7). Furosemide intravenously can be used to decrease total body water, particularly when transient hypervolemia associated with mannitol is to be avoided.
Blood pressure (BP) control: Systemic antihypertensives are used only when hypertension is severe (> 180/95 mm Hg). The target blood pressure depends on the clinical context. Systemic BP needs to be high enough to maintain cerebral perfusion pressure even when ICP increases. Hypertension can be managed by titrating nicardipine as a continuous IV infusion (8) or by boluses of labetalol.
Glucocorticoids: Glucocorticoids are useful for treating vasogenic brain edema. Vasogenic edema results from disruption of the blood-brain barrier, which may occur in patients with a brain tumor. Cytotoxic edema results from cell death and breakdown, which may occur in patients with stroke, cerebral hemorrhage, or trauma or after hypoxic brain damage due to cardiac arrest. Glucocorticoids are effective only when vasogenic edema is present. They are ineffective for cytotoxic edema and can increase plasma glucose, exacerbating cerebral ischemia and complicating management of diabetes mellitus. When indicated for patients without brain ischemia, dexamethasone can be given IV or orally.
Removal of cerebrospinal fluid (CSF): CSF can be slowly removed through a shunt inserted into the ventricles to help lower increased ICP. CSF is removed at a rate of 10 to 15 mL/minute (9). Continuous drainage of CSF (eg, through a lumbar drain) should be avoided because it may lead to brain herniation.
Position: Positioning the patient to maximize venous outflow from the head can help minimize increases in ICP. The head of the bed can be elevated to 30° (with the head above the heart) as long as cerebral perfusion pressure remains at the desired range. The patient’s head should be kept in a midline position, and neck rotation and flexion should be minimized. Tracheal suctioning, which can increase ICP, should be limited.
If ICP continues to increase despite other measures to control it, the following may be used:
Titrated hypothermia: When ICP is increased after head trauma or cardiac arrest, hypothermia in the range of 32 to 35° C has been used to reduce ICP to < 20 mm Hg. While several studies conflict about the benefit of hypothermia, a meta-analysis of over 50 trials suggests likely benefit for therapeutic hypothermia in adults but does not recommend its use in children (10).
Pentobarbital coma: Pentobarbital can reduce cerebral blood flow and metabolic demands. However, its use is controversial because the effect on clinical outcome is not consistently beneficial, and treatment with pentobarbital can lead to complications (eg, hypotension, arrhythmias, myocardial depression). In some patients with refractory intracranial hypertension that does not respond to standard hyperventilation and hyperosmolar therapy, pentobarbital given as a last resort may improve functional outcome (8).
Decompressive craniotomy: Craniotomy with duraplasty can be done to provide room for brain swelling. This procedure can prevent deaths, but overall functional outcome may not improve much, and it may lead to complications such as hydrocephalus (11). It may be most useful for large cerebral infarcts with impending herniation, particularly in patients < 50 years.
Long-term care
Patients require meticulous long-term care. Stimulants, sedatives, and opioids should be avoided.
Enteral feeding is started with precautions to prevent aspiration (eg, elevation of the head of the bed); a percutaneous endoscopic jejunostomy tube is placed if necessary.
Early, vigilant attention to skin care, including checking for breakdown especially at pressure points, is required to prevent pressure ulcers. Patients require frequent turning and position changes to prevent pressure ulcers, but the head should be kept elevated. Special air mattresses may help manage pressure ulcers.
Topical ointments to prevent desiccation of the eyes are beneficial.
Passive range-of-motion exercises done by physical therapists and taping or dynamic flexion splitting of the extremities may prevent contractures. Initiating physical therapy early can improve functional outcome in patients with polyneuropathy and myopathy.
Measures are also taken to prevent urinary tract infections and deep venous thrombosis.
Treatment references
1. Giacino JT, Katz DI, Schiff ND, et al. Practice guideline update recommendations summary: Disorders of consciousness: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology; the American Congress of Rehabilitation Medicine; and the National Institute on Disability, Independent Living, and Rehabilitation Research. Neurology. 2018;91(10):450-460. doi:10.1212/WNL.0000000000005926
2. Freund Y; Viglino D, Cachanado M, et al. Effect of noninvasive airway management of comatose patients with acute poisoning: A randomized clinical trial. JAMA. 2023; 330(23):2267–2274. doi: 10.1001/jama.2023.24391
3. Mostafa HM, Ibrahim RW, Hasanin A, et al. Intravenous lidocaine for attenuation of pressor response after endotracheal intubation. A randomized, double-blinded dose-finding study. Egypt J Anaesthesia. 2023;39:1:241-248, 2023. doi: 10.1080/11101849.2023.2187142
4. Hwang C, Michaels B, Park K, et al. Impact of paralytic choice on postintubation sedation and analgesia in the emergency department. Am J Health Syst Pharm. 2025;82(Supplement_3):S2929-S2936. doi:10.1093/ajhp/zxaf037
5. Cook AM, Jones GM, Hawryluk GWJ, et al. Guidelines for the acute treatment of cerebral edema in neurocritical care patients. Neurocrit Care. 32 (3):647–666 2020. doi: 10.1007/s12028-02-00959-7
6. Singh A, Anjankar AP. Propofol-Related Infusion Syndrome: A Clinical Review. Cureus. 2022;14(10):e30383. Published 2022 Oct 17. doi:10.7759/cureus.30383
7. Shi J, Tan L, Ye J, Hu L. Hypertonic saline and mannitol in patients with traumatic brain injury: A systematic and meta-analysis. Medicine (Baltimore). 2020;99(35):e21655. doi:10.1097/MD.0000000000021655
8. Ragland J, Lee K. Critical Care Management and Monitoring of Intracranial Pressure. J Neurocrit Care. 9(2):105-112, 2016. doi: 10.18700/jnc.160101
9. Bertuccio A, Marasco S, Longhitano Y, et al. External Ventricular Drainage: A Practical Guide for Neuro-Anesthesiologists. Clin Pract. 2023;13(1):219-229. Published 2023 Jan 31. doi:10.3390/clinpract13010020
10. Crompton EM, Lubomirova I, Cotlarciuc I, Han TS, Sharma SD, Sharma P. Meta-Analysis of Therapeutic Hypothermia for Traumatic Brain Injury in Adult and Pediatric Patients. Crit Care Med. 2017;45(4):575-583. doi:10.1097/CCM.0000000000002205
11. Su TM, Lan CM, Lee TH, et al. Risk factors for the development of posttraumatic hydrocephalus after unilateral decompressive craniectomy in patients with traumatic brain injury. J Clin Neurosci. 63:62–67, 2019. doi: 10.1016/j.jocn.2019.02.006
Prognosis for Coma and Impaired Consciousness
Prognosis for patients with impaired consciousness depends on the cause, duration, and depth of the impairment of consciousness. For example, absent pupillary responses indicates a poor prognosis after cardiac arrest, but not always after a sedative overdose. In general, prognosis is more favorable if unresponsiveness lasts < 6 hours.
The prognosis for coma recovery becomes progressively more difficult to formulate as each level of function is restored (eg, eye opening indicating transition to vegetative state, emergent behaviors signaling transition to minimally conscious state). Accordingly, establishing prognosis requires careful serial examinations and increasingly widening time intervals as new levels of function emerge.
After coma, the following prognostic signs are considered favorable (1):
Early return of speech (even if incomprehensible)
Spontaneous eye movements that can track objects
Normal resting muscle tone
Ability to follow commands
If the cause is a reversible condition (eg, sedative overdose, some metabolic disorders such as uremia), patients may lose all brain stem reflexes and all motor response and yet recover fully. After trauma, a score of 3 to 5, especially if pupils are fixed or oculovestibular reflexes are absent, may indicate fatal brain damage. However, structural imaging assessments are always required, and possible confounding factors to the examination (eg, local tissue damage causing cranial nerve dysfunction while central nervous system tissue/function is preserved) need to be taken into consideration.
After cardiac arrest, clinicians must exclude major confounders of coma, including sedatives, neuromuscular blockade, hypothermia, metabolic derangements, and severe liver or kidney failure. If brain stem reflexes are absent at day 1 or lost later, testing for brain death is indicated. Prognosis is poor if patients have any of the following (2):
No pupillary light reflexes 24 to 72 hours after cardiac arrest
No corneal reflexes 72 hours after cardiac arrest
Extensor posturing or no response elicited by painful stimuli 72 hours after cardiac arrest (if no targeted temperature management has been instituted)
No response 20 milliseconds after stimulation of somatosensory evoked potential (SEP)
Serum neuron-specific enolase level of > 33 mcg/L with escalating concentrations in serial testing over 72 hours (in the absence of confounders such as hemolysis or hemorrhage elevating the marker)
Preexisting disorders such as coronary artery disease, hypertension, and diabetes mellitus
If patients who are unresponsive after cardiac arrest have been treated with hypothermia, strict prevention of fever temperatures ≥ 37.5° C (also known as targeted temperature management [TTM]), or targeted normothermia (often for about 24 to 48 hours after arrest), at least 72 hours should be added to the above times because TTM has been associated with delayed recoveries.
If any of the above criteria is met, outcome is usually (but not always) poor; thus, whether to withdraw life support may be a difficult decision.
Depending on the cause and duration of impaired consciousness, medical complications beyond the coma itself may affect prognosis. For example, a medication or disorder causing metabolic coma may also cause hypotension, arrhythmias, myocardial infarction, or pulmonary edema. Prolonged hospitalization in an ICU may also result in polyneuropathy, myopathy, and other complications (eg, pulmonary embolism, pressure ulcers, urinary tract infection).
Prognosis references
1. Levy DE, Caronna JJ, Singer BH, Lapinski RH, Frydman H, Plum F. Predicting outcome from hypoxic-ischemic coma. JAMA. 1985;253(10):1420-1426.
2. Sandroni C, Cariou A, Cavallaro F, et al. Prognostication in comatose survivors of cardiac arrest: an advisory statement from the European Resuscitation Council and the European Society of Intensive Care Medicine. Intensive Care Med. 2014;40(12):1816-1831. doi:10.1007/s00134-014-3470-x
Geriatrics Essentials: Coma and Impaired Consciousness
Older patients may be more susceptible to coma, altered consciousness, and delirium because of many factors, including the following:
Less cognitive reserve due to age-related brain effects and/or preexisting brain disorders
Higher risk of drug interactions affecting the brain due to polypharmacy
Higher risk of drug accumulation and drug effects on the brain due to age-related decreased function of organs responsible for drug metabolism and elimination
Higher risk of incorrect drug dosing due to polypharmacy with complex dosing regimens
Presence of comorbid disorders (eg, diabetes mellitus, hypertension, renal disease)
Higher risk of subdural hematoma due to traumatic rupture of veins crossing the growing subdural space between the dura and surface of the aging atrophic brain
Relatively minor problems, such as dehydration and urinary tract infections, can alter consciousness in older adults.
In older patients, mental status and communications skills may be compromised, making lethargy and obtundation harder to recognize.
Age-related decreases in cognitive reserve and neuroplasticity can impair recovery from brain injury.
Key Points
Coma and impaired consciousness require dysfunction of both cerebral hemispheres or dysfunction of the reticular activating system.
Manifestations include abnormalities of the eyes (eg, abnormal conjugate gaze, pupillary responses, and/or oculocephalic or oculovestibular reflexes), vital signs (eg, abnormal respirations), and motor function (eg, flaccidity, hemiparesis, asterixis, multifocal myoclonus, decorticate or decerebrate posturing).
Taking a complete history of prior events is critical; ask witnesses and caregivers about the time course for the change in mental status and about possible causes (eg, recent travel, ingestion of unusual meals, exposure to possible infections, medication, illicit drug or alcohol use, possible trauma).
Do a general physical examination, including thorough examination of the head and face, skin, and extremities and a complete neurologic examination (focusing on level of consciousness, the eyes, motor function, and deep tendon reflexes), followed by appropriate blood and urine tests, toxicology screening, and fingerstick plasma glucose measurements.
As soon as the patient has been stabilized, do noncontrast CT or, if immediately available, MRI to check for masses, hemorrhage, edema, hydrocephalus, or evidence of bone trauma (particularly on a CT scan); overall, MRI provides greater detail for diagnostic purposes when it is done 72 hours or more after symptom onset.
Ensure adequate airway, breathing, and circulation.
Give IV or IM thiamine and IV glucose if plasma glucose is low and IV naloxone if opioid overdose is suspected.
Control ICP using various strategies, which may include sedatives (as needed) to control agitation, temporary hyperventilation, fluids and diuretics to maintain euvolemia, and antihypertensives to control blood pressure.
Treat the cause.
Drug Information for the Topic





