

Pelvic examinations should be done when indicated based on a woman's medical history or symptoms. The patient and the clinician who provides gynecologic care should discuss and decide together whether a pelvic examination is needed. For patients who decline a pelvic examination, a self-collected vaginal swab to test for gonorrhea and chlamydia should be discussed if the patient is < 25 years old.
A pelvic examination may be performed to assess a specific issue, such as pelvic pain, abnormal vaginal bleeding, vaginal discharge, or vulvovaginal symptoms (eg, pruritus), as part of preventive care, or as part of a gynecologic procedure.
The clinician should explain what will happen before each step of the examination. The American College of Obstetricians and Gynecologist (ACOG) recommends that a chaperone be present for all breast, genital, and rectal examinations (1).
Reference
1. American College of Obstetricians and Gynecologists (ACOG): ACOG Committee Opinion, Number 796: Sexual Misconduct. Obstet Gynecol. 2020;135(1):e43-e50. doi:10.1097/AOG.0000000000003608
Pelvic Examination Procedure
The examiner should have adequate light and should have the speculum and any other instruments or supplies readily available.
For the female pelvic examination, the patient lies supine on an examination table with her feet in stirrups (dorsal lithotomy position) and is usually draped.
The pelvic examination includes the following:
External examination of mons pubis and vulva
Speculum examination
Bimanual examination
Rectovaginal examination (sometimes)
A pelvic examination is indicated for
Symptomatic patients (eg, those with pelvic pain or abnormal uterine bleeding)
Asymptomatic patients with specific indications (eg, need for cervical cancer screening)
Before beginning the pelvic examination, the patient should be asked to void to empty the bladder. An empty bladder is important for the accurate assessment of uterovaginal prolapse, because increased bladder volume may reduce the extent of prolapse. Also, a full bladder may add further discomfort to the pelvic examination in some patients. Prior to the examination, many clinicians collect a urine sample if needed for analysis, culture, or sexually transmitted infection (STI) testing.
A pelvic examination has not been found to be an effective screening test for ovarian cancer (see ACOG Committee Opinion No. 754: The Utility of and Indications for Routine Pelvic Examination).

External examination
The external examination is a visual inspection and palpation to assess the pubic and groin areas and the external genitals.
The mons pubis and the hair-bearing areas of the labia majora are inspected for lesions or other findings based on symptoms (eg, folliculitis, lice). The skin of the groin and the perineum are inspected for erythema, abnormal pigmentation, and skin lesions (eg, warts, excoriations, erosions, ulcers, fissures, pustules, nodules, tumors).
The complete external examination includes examination of the entire vulva from the clitoris to the area below the anus to confirm any architectural changes in the skin. Clinicians should be familiar with normal vulval anatomy and variation. The clitoral hood should be mobile and easily retracted. The urethral meatus is inspected for lesions (eg, urethral carbuncle). The labia minora and majora are examined. Vulval skin disorders can cause changes in color, texture, and architecture of the vulval anatomy. Structural abnormalities due to prior procedures (eg, episiotomy, female genital mutilation) are noted.
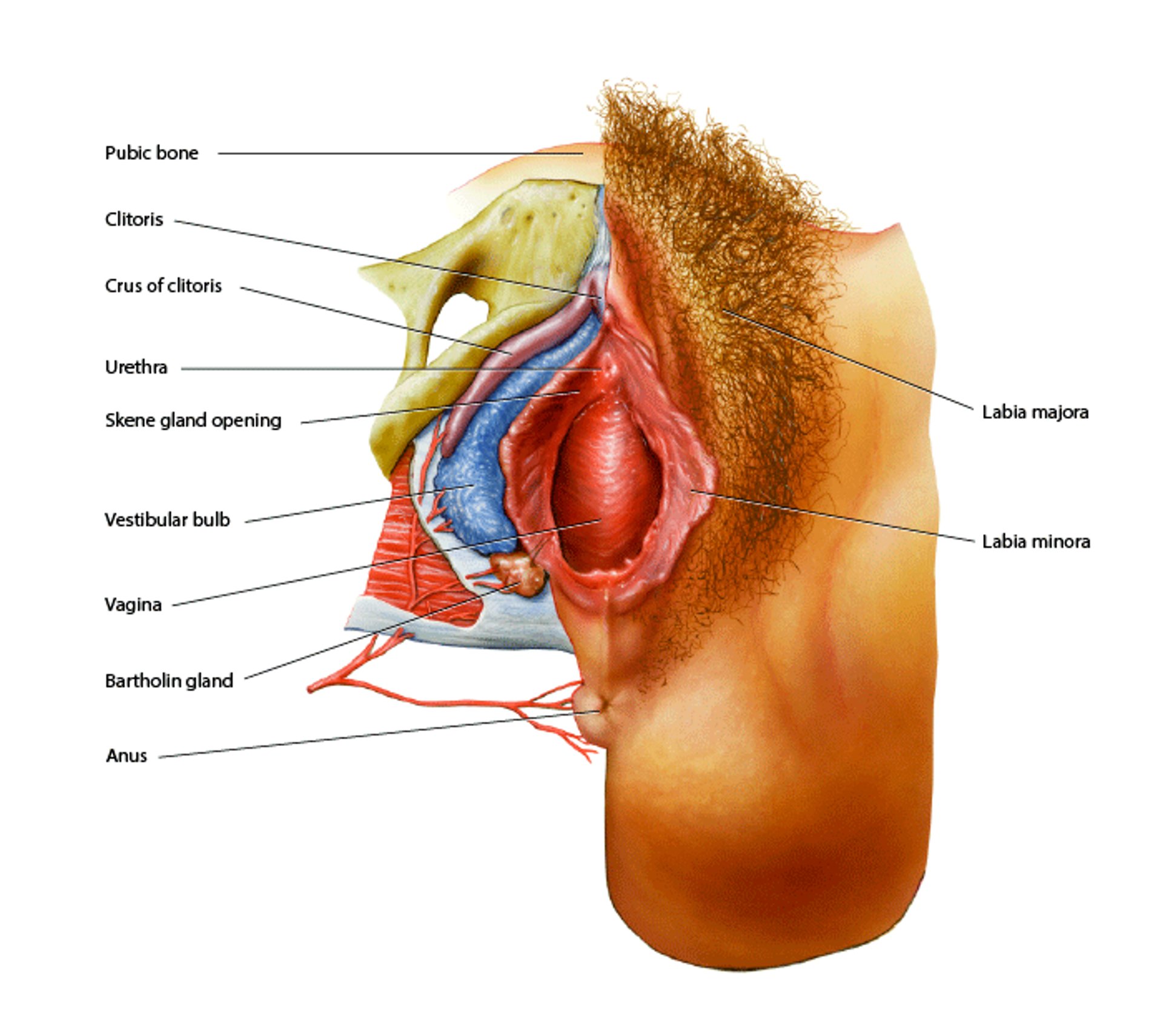
Vulvar Anatomy
The vagina is composed of smooth muscle lined by glandular and squamous epithelium. The urethral meatus is located in the anterior portion of the vaginal introitus. The Skene gland openings are located on both sides of the urethra. The tissue surrounding the vagina is the vulva, which includes the labia minora, labia majora, and the glans and hood of the clitoris (most anteriorly and in the midline, anterior to the urethra). Anterior to the clitoris is the mons pubis (tissue that covers the pubic bone). Posterior to the vagina is the perineum, an area of skin in between the vagina and anus. The crura of the clitoris (purple) extend subcutaneously and are composed of erectile tissue. The bulb of the vestibule (blue) also consists of erectile tissue. Below the bulb is a Bartholin gland, which secretes mucus to lubricate the vagina. BO VEISLAND/SCIENCE PHOTO LIBRARY |

Patients reporting symptoms of vulvovaginal pain during sexual activity or daily activities should be evaluated for conditions, including vulvodynia, vestibulitis, bladder tenderness, or vaginismus (spasm of pelvic floor muscles). A cotton swab can be touched gently to several points on the vulva to identify the location and severity of the pain. Cotton swab tests are done to assess the spasm of the muscle in cases of vaginismus. A moistened cotton swab is used to press lightly from lateral to medial area from groin to vestibule in clockwise fashion. Focal pain to light touching of the vulvar vestibule is characteristic of vulvodynia.
If a patient has anal incontinence or other pelvic floor neurologic issues, sensory function of the pudendal nerve can be tested by eliciting the anocutaneous reflex (anal wink sign). This is done by using a cotton swab to stroke the perianal skin, which should cause the external anal sphincter to contract.
Next, the introitus is inspected. If the patient has symptoms or a history of a Bartholin gland cyst or abscess, the gland is palpated between the thumb and index finger.
Pelvic organ prolapse is assessed by asking the patient to bear down. The examiner checks the vaginal opening for signs of pelvic organ prolapse: an anterior bulge (suggesting cystocele), a posterior bulge (suggesting rectocele), and displacement of the cervix toward the introitus (suggesting prolapsed uterus).
Speculum examination
The speculum is a metal or plastic instrument used to retract the vaginal walls to enable the clinician to examine the vagina and cervix. There are 2 main types of speculum: Graves (curved blades) and Pederson (straight blades). Both come in different sizes; the Pederson has a narrow and a pediatric size. A smaller speculum should be used if needed based on the patient's anatomy or discomfort.
Before the speculum examination, the patient is asked to relax the legs and hips. The speculum is sometimes warmed prior to the examination and lubricated with water-based lubricant before insertion. Lubricant is avoided if collecting a sample for cervical cytology. If water-based lubricant is not available, the speculum can be rinsed with the warm water prior to insertion.
A gloved finger may be inserted into the vagina first to determine the position of the cervix. The speculum is inserted with the blades nearly in the vertical plane (at about 1 and 7 o’clock).

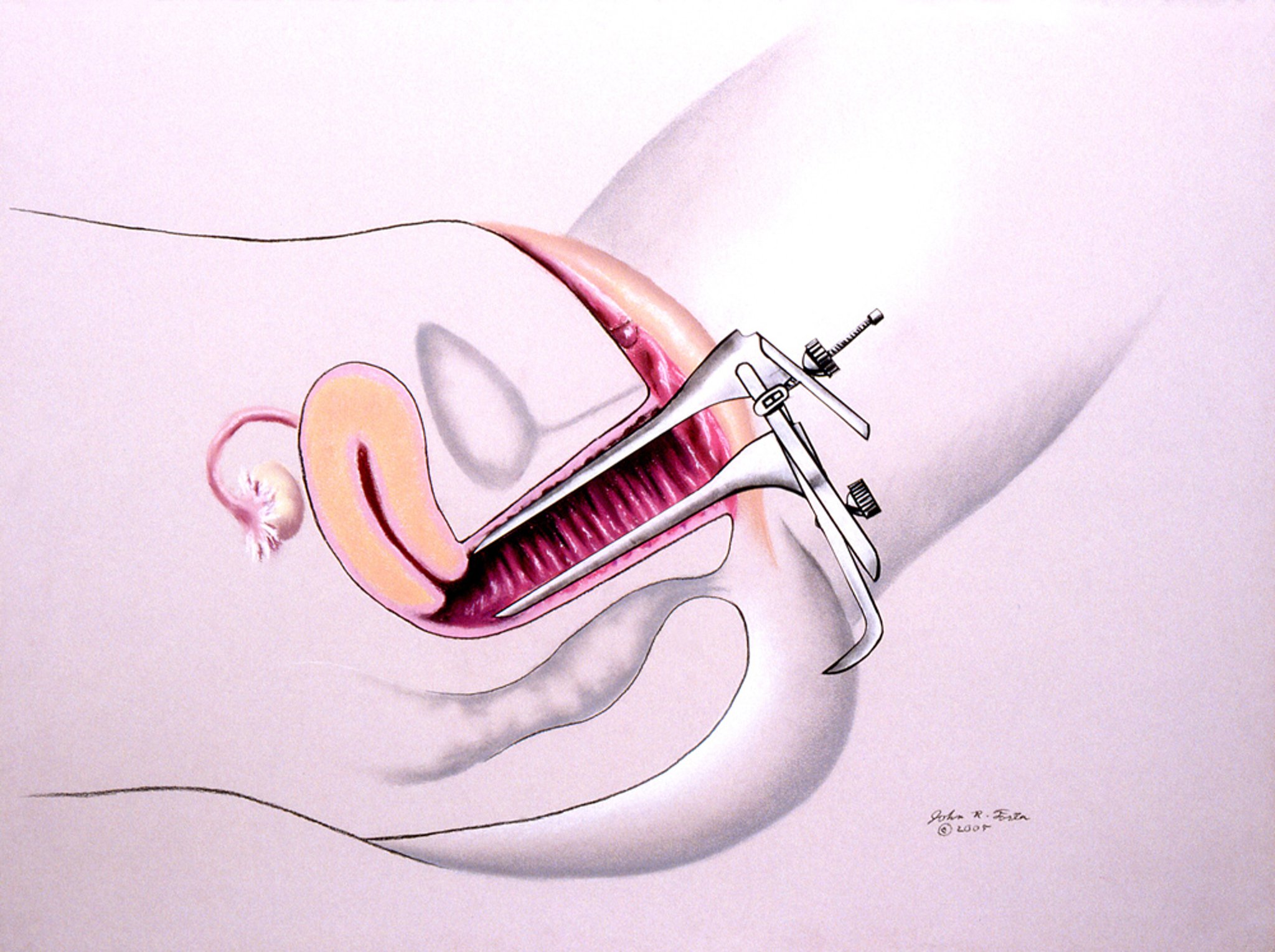
JOHN FOSTER/SCIENCE PHOTO LIBRARY
The speculum is fully inserted toward the cervix, then rotated so that the handle is down, and gently opened; it is pulled back as needed to visualize the cervix. When the cervix is seen, the blades are positioned so that the posterior blade is deeper than the cervix (in the posterior vaginal fornix) and the anterior blade is allowed to rise gently and rest anterior to the cervix (in the anterior fornix). The examiner should take care to open and close the speculum slowly and gently to avoid causing unnecessary discomfort.
If it is difficult to visualize the cervix, hyperflexion of both hip joints to bring both thighs close to the abdominal wall in the dorsal lithotomy position may aid the examination. This position and a longer or wider speculum may be useful for the examination of patients with morbid obesity.
The cervix is visually inspected for erythema, lesions, or discharge or bleeding from the cervical os. In cases of trichomonas vaginitis, the exocervix may show punctuations or petechiae. Any cervical lesion can be biopsied using cervical punch biopsy forceps or Allis clamps, including polyps, ulcers, fungating masses, and warts.


SCIENCE PHOTO LIBRARY
While inserting or removing the speculum, the clinician should look for any vaginal erythema, erosions, ulcerations, synechiae, or discharge. Normal vaginal discharge is commonly white or clear and odorless, and the amount is minimal. Abnormal vaginal discharge may have a fishy odor and be thin and gray, frothy and yellow-green, or thick and white, resembling cheese curds. Additional tests such as pH tests, the whiff test, microscopy examination, fungal cultures, gonorrhea/chlamydia PCR test, or a commercially available vaginitis swab test can be done for the abnormal vaginal discharge.
A specimen for the Papanicolaou (Pap) test is taken from the endocervix and external cervix with a brush and plastic spatula or with a cervical sampler that can simultaneously collect cells from the cervical canal and the transition zone. The specimen is placed in a liquid medium, producing a cell suspension to be analyzed for cytology and human papillomavirus testing, and sometimes for gonorrhea, chlamydia, and trichomoniasis. Any menstrual or other blood, discharge, or other substances (eg, vaginal medications) that are covering the cervix, can be wiped off using a long cotton swab before collecting the Pap test sample.
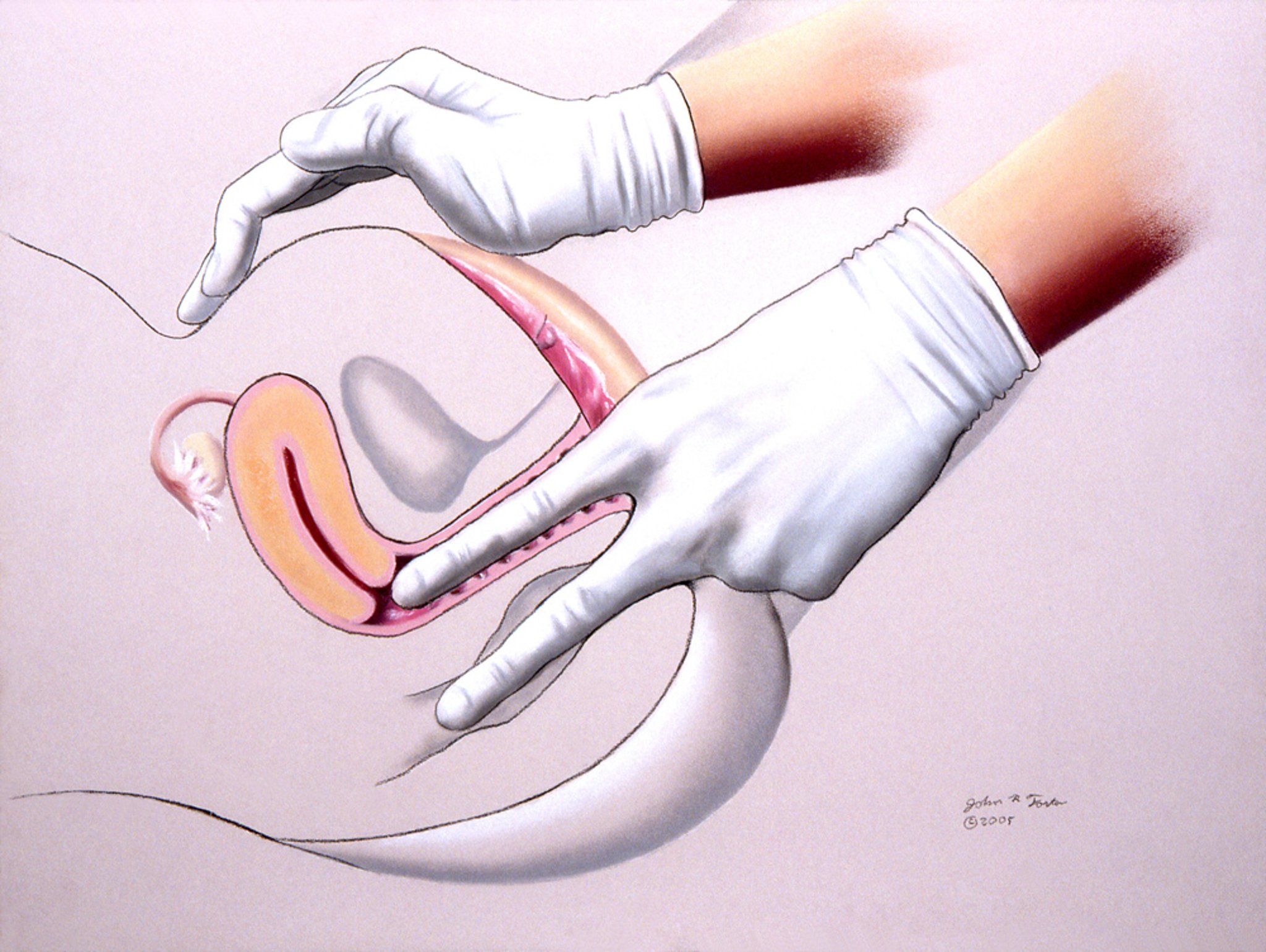
Bimanual examination
The bimanual examination is done with 2 fingers in the vagina and the other hand on the lower abdomen to palpate the vagina, cervix, uterus, and ovaries. The fallopian tubes are only palpable if there is a tubal mass.
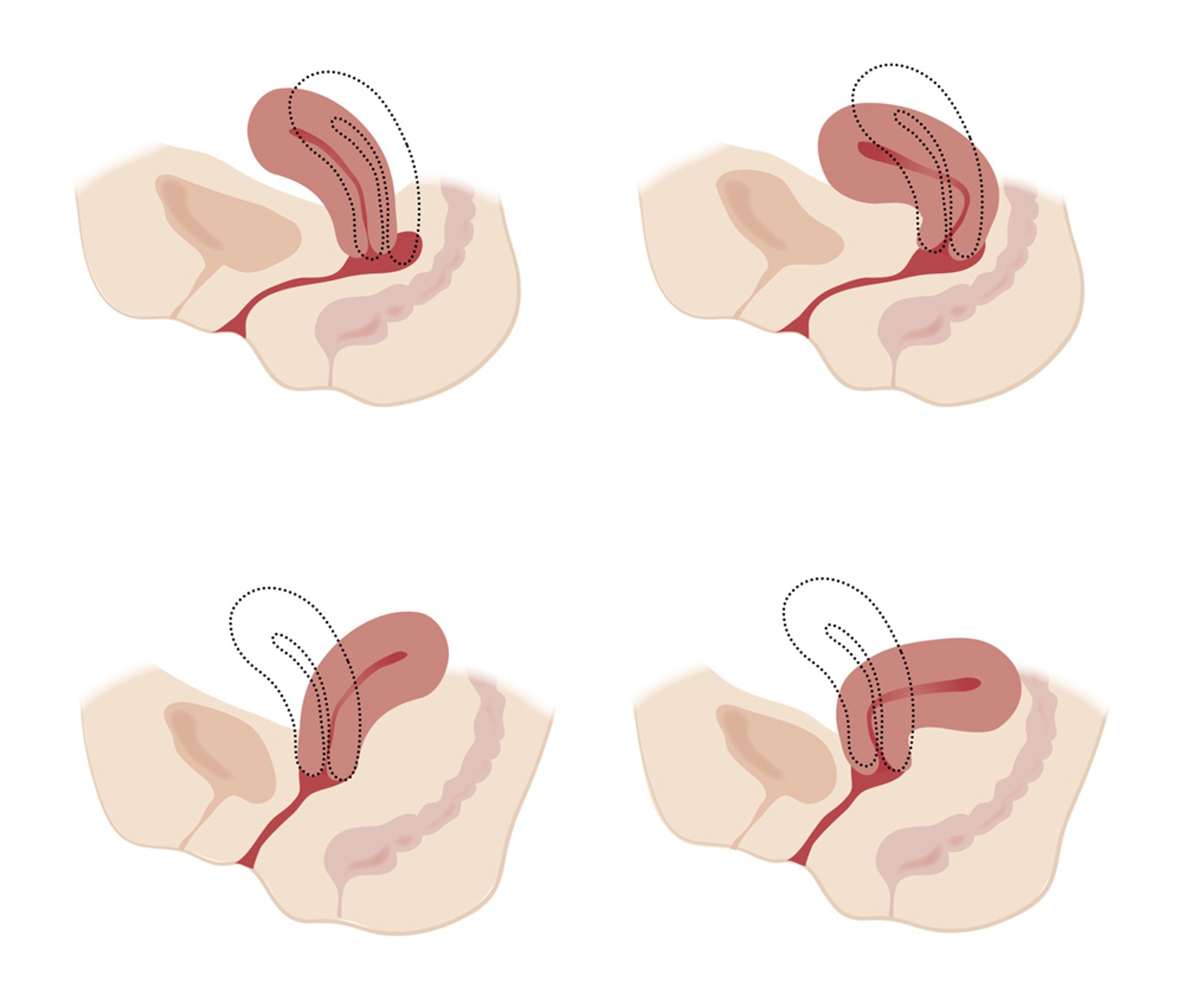
The index and middle fingers of the dominant hand are inserted into the vagina to just below the cervix. The other hand is placed just above the pubic symphysis and gently presses down to determine the size, position, consistency, and mobility of the uterus and, if possible, the ovaries. Normally, the uterus is about 7 cm by 5 cm by 3 cm and tilts anteriorly (anteversion), but it may tilt posteriorly (retroversion) to various degrees. The uterus may also be bent at an angle anteriorly (anteflexion) or posteriorly (retroflexion).

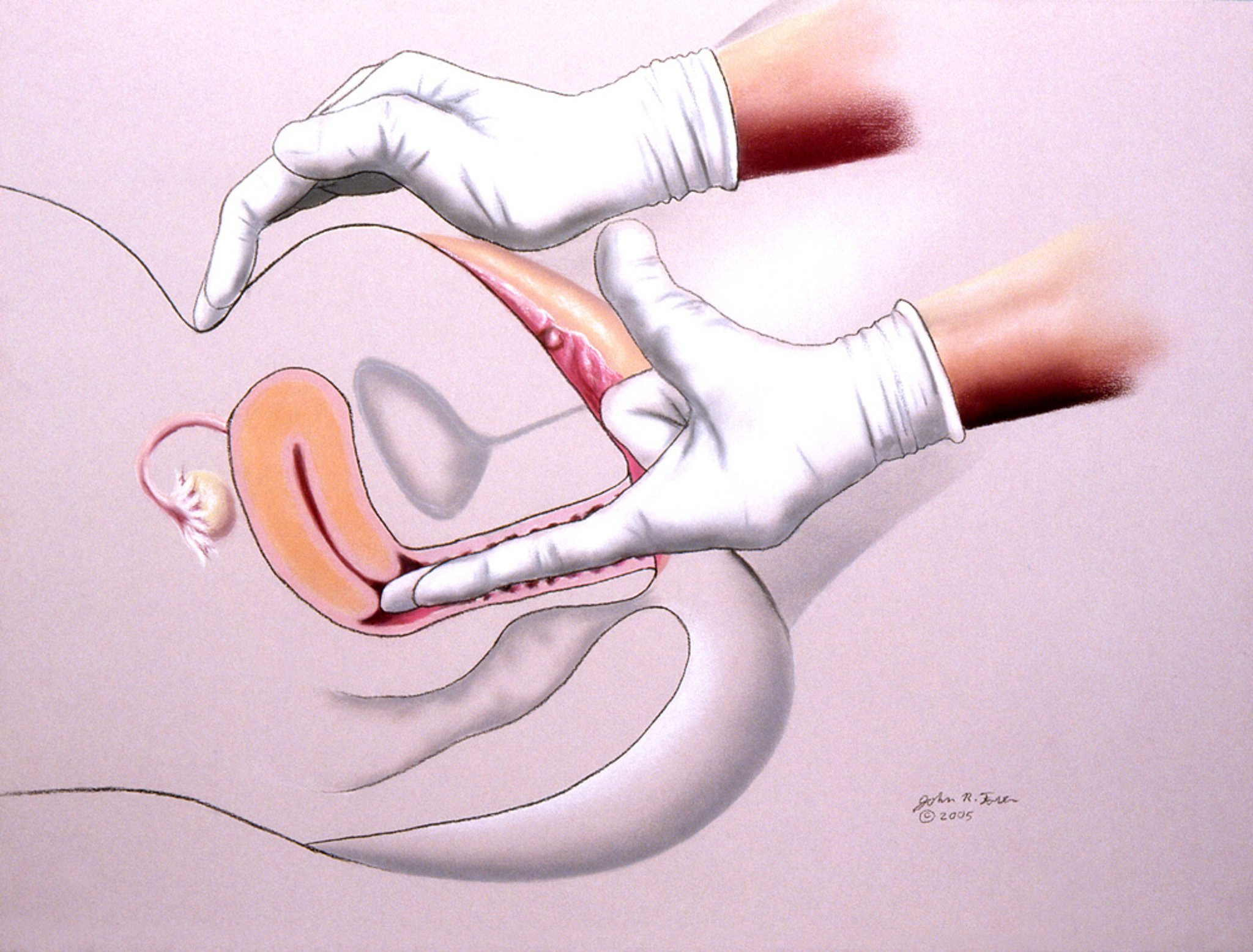
JOHN FOSTER/SCIENCE PHOTO LIBRARY

JEANETTE ENGQVIST/SCIENCE PHOTO LIBRARY
The uterus is normally mobile, firm, and smooth; irregularity suggests uterine fibroids (leiomyomas). A fixed uterus may suggest adhesions from endometriosis, prior surgeries, or infections. Any palpable nodules along the cul-de-sac or uterosacral ligament posteriorly may suggest endometriosis.
Normally, the ovaries are about 2 cm by 3 cm in young women and are not palpable in postmenopausal women. Any enlargement of ovaries or adnexal masses may be palpated. Adnexal tenderness may be present in patients with a ruptured hemorrhagic ovarian cyst, ectopic pregnancy, ovarian or adnexal torsion, tubo-ovarian abscess, acute or chronic pelvic inflammatory disease, and rare cases of retrocecal appendicitis on the right side. An ovarian cyst or tumors or pedunculated fibroids may be tender if there are hemorrhagic changes.
Significant pain when the cervix is gently moved from side to side (cervical motion tenderness) suggests pelvic inflammation and is one of the diagnostic criteria for pelvic inflammatory disease.
Rectovaginal examination
After bimanual palpation, if indicated, the examiner palpates the rectovaginal septum by inserting the index finger in the vagina and the middle finger in the rectum. The rectovaginal examination may detect an ovarian mass.

JOHN FOSTER/SCIENCE PHOTO LIBRARY





