

Dizziness is an imprecise term patients often use to describe various related sensations, including
Faintness (a feeling of impending syncope)
Light-headedness
Feeling of imbalance or unsteadiness
A vague spaced-out or swimmy-headed feeling
A spinning sensation
Dizziness may be temporary or chronic. Chronic dizziness, defined as lasting > 1 month, is more common among older adults.
Vertigo is a sensation of movement of the self or the environment when there is no actual movement. Usually the perceived movement is rotary—a spinning or rolling sensation—but some patients simply feel pulled to one side. Vertigo is not a diagnosis—it is a description of a sensation.
Vertigo is typically categorized as peripheral or central.
Peripheral vertigo is generally caused by dysfunction within the peripheral vestibular system.
Central vertigo is usually caused by dysfunction within the brain stem or cerebellum.
Both dizziness and vertigo may be accompanied by nausea and vomiting or difficulty with balance, gait, or both.
Patients often use “dizziness,” “vertigo,” and other terms interchangeably and inconsistently, in part because these sensations can be difficult to describe. Patients with the same underlying disorder may describe their symptoms very differently. A patient may even provide differing descriptions of the same “dizzy” event, depending on how the question is phrased. Thus, clinicians must often consider the 2 symptoms together.
However they are described, dizziness and vertigo may be disturbing and even incapacitating, particularly when accompanied by nausea and vomiting. Symptoms pose significant challenges for people doing an exacting or dangerous task, such as driving, flying, or operating heavy machinery. Importantly, dizziness and vertigo are potent risk factors for falling, especially in older adults (1).
The one-year prevalence of dizziness in U.S. adults is 11% based on national health survey data (1). In a large cohort study, vertigo and dizziness accounted for 2.5% of emergency department visits over a 10-year period (2).
General references
1. Lin HW, Bhattacharyya N. Impact of dizziness and obesity on the prevalence of falls and fall-related injuries. Laryngoscope 2014;124(12):2797-2801. doi:10.1002/lary.24806
2. Kerber KA, Meurer WJ, West BT, Fendrick AM. Dizziness presentations in U.S. emergency departments, 1995-2004. Acad Emerg Med 2008;15(8):744-750. doi:10.1111/j.1553-2712.2008.00189.x
Pathophysiology of Dizziness and Vertigo
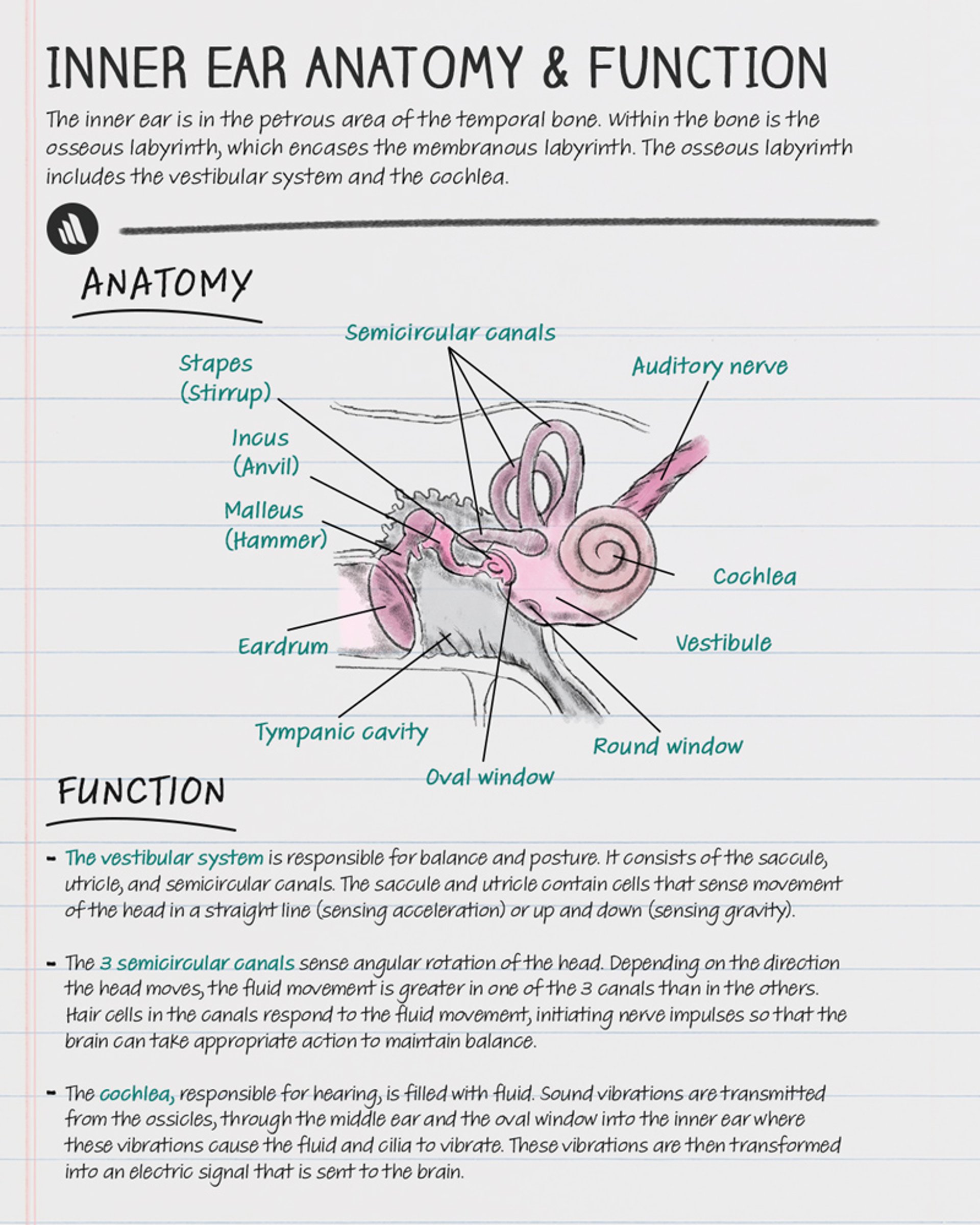
The vestibular system is the main neurologic system involved in balance. This system includes

Copyright © 2023 Merck & Co., Inc., Rahway, NJ, USA and its affiliates. All rights reserved.
The vestibular apparatus of the inner ear
The 8th (vestibulocochlear) cranial nerve, which conducts signals from the vestibular apparatus to the central components of the system
The vestibular nuclei in the brain stem and cerebellum
Disorders of the inner ear and 8th cranial nerve are considered peripheral disorders. Those of the vestibular nuclei and their pathways in the brain stem and cerebellum are considered central disorders.
The sense of balance also incorporates visual input from the eyes and proprioceptive input from the peripheral nerves (via the spinal cord). The cerebral cortex receives output from the lower centers and integrates the information to produce the perception of motion.

Vestibular apparatus
Perception of stability, motion, and orientation to gravity originates in the vestibular apparatus, which consists of
The 3 semicircular canals
The 2 otolith organs—the saccule and utricle
Rotary motion causes flow of endolymph in the semicircular canal oriented in the plane of motion. Depending on the direction of flow, endolymph movement either stimulates or inhibits neuronal output from hair cells lining the canal. Similar hair cells in the saccule and utricle are embedded in a matrix of calcium carbonate crystals (otoliths). Deflection of the otoliths by gravity stimulates or inhibits neuronal output from the attached hair cells.
Etiology of Dizziness and Vertigo
There are numerous structural (trauma, tumors, degenerative), vascular, infectious, toxic (including medication-related), and idiopathic causes of dizziness and vertigo (see table ), but only a small percentage of cases are caused by a serious disorder. It is helpful to use a framework that specifies peripheral versus central causes of dizziness and vertigo. Peripheral vertigo or dizziness refers to symptoms arising due to dysfunction in the middle ear, inner ear (cochlea, vestibule, semicircular canals, utricle, saccule), or vestibular nerve. Central vertigo or dizziness implies dysfunction at the level of the central nervous system or brain. It is common for patients with dizziness or vertigo to have more than one diagnosis. In particular, vestibular migraine (a central cause of vertigo and dizziness) is more common in patients with benign paroxysmal positional vertigo (1) and Meniere disease (2).
The most common causes of peripheral dizziness or vertigo are listed in decreasing order of frequency (3):
Presbyvestibulopathy
The most common causes of central dizziness or vertigo, in decreasing order of frequency, include the following:
Vestibular migraine (4)
Medication side effects, especially antihypertensives such as beta-blockers or when multiple antihypertensives are used concurrently (5)
Functional dizziness (persistent postural perceptual dizziness [PPPD], formerly known as visual vertigo or chronic subjective dizziness, motion sickness, mal de debarquement syndrome) (6)
Presbyvestibulopathy(7)
In the United States, vestibular migraine has a 1-year prevalence of 2.7%, making it likely the most common cause of dizziness (4).
Other less common causes of central vertigo include disorders with a more global effect on cerebral function (eg, brain stem hemorrhage or infarction, multiple sclerosis, dementia, Parkinson disease), cerebellar dysfunction brain tumor (specifically posterior fossa tumor), a psychiatric disorder, or a disorder affecting visual or proprioceptive input. Oftentimes, no definitive cause can be found.
As with hearing, there is a natural decline in both the peripheral and central centers for controlling balance in the inner ear and brain (presbyvestibulopathy) (7).
Regardless of the diagnosis, dizziness, vertigo, or imbalance of any kind significantly increases the risk for falls and falls-related injuries, and should be taken seriously (8). Balance physical therapy (also known as vestibular physical therapy) is helpful for nearly all patients with chronic dizziness, except for patients with extreme motion sickness.
The most common causes of dizziness without vertigo are less clear cut, but they are usually not otologic and probably are
Medication effects, especially antihypertensives
Multifactorial or idiopathic
Functional dizziness
Nonneurologic disorders with a more global effect on cerebral function sometimes manifest as dizziness and rarely as vertigo. These disorders typically involve inadequate substrate (eg, oxygen, glucose) delivery caused by hypotension, hypoxemia, anemia, or hypoglycemia; when severe, some of these disorders may manifest as syncope. Additionally, certain hormonal changes (eg, as with thyroid disease, menstruation, pregnancy) can cause dizziness. Numerous central nervous system-active medications can cause dizziness independent of any toxic effect on the vestibular system.
Occasionally, dizziness and vertigo may be psychogenic. Patients with panic disorder, hyperventilation syndrome, anxiety, or depression may have dizziness. Depression, anxiety, or both, are present in up to 50% of patients with chronic dizziness (9).
Persistent perceptual postural dizziness (PPPD), sometimes described as chronic internal swaying that goes away when lying flat and lasting for over 3 months with no clinical explanation for its persistence, is classified as a chronic functional disorder. It can be precipitated by other acute conditions, such as BPPV or vestibular migraine, or can be a manifestation of an anxiety disorder.
Uncompensated peripheral vestibular weakness causes dysequilibrium rather than vertigo and often visual blurring with head turning. It can be the result of vestibular neuronitis, migraine with vertigo, Meniere disease, head trauma, or inner ear surgery.
In older patients, dizziness is often multifactorial secondary to medication adverse effects and age-diminished visual, vestibular, and proprioceptive abilities. Two of the most common specific causes are disorders of the inner ear: BPPV and Meniere disease.
Selected Causes of Dizziness and Vertigo
Cause | Suggestive Findings | Diagnostic Approach |
|---|---|---|
Peripheral vestibular system disordersa,b | ||
Severe, brief (< 2 minute) spinning produced by moving head in a specific direction Nystagmus that has a latency of 0 to 30 seconds, is fatigable, and is torsional, beating toward the undermost ear Frenzel goggles often needed to prevent visual fixation and reveal nystagmus Hearing and neurologic examination normal | Dix-Hallpike maneuver to assess characteristic positional nystagmus | |
Spinning sensation, most times with nausea and vomiting, lasting 20 minutes to 12 hours Recurrent episodes of unilateral tinnitus, hearing loss, ear fullness during episodes of vertigo | Audiometry Gadolinium-enhanced MRI to exclude other causes | |
Vestibular neuronitis (viral cause suspected) | Sudden, incapacitating, severe vertigo with no hearing loss or other findings Lasts up to 1 week, with gradual lessening of symptoms Positional vertigo may result | Sometimes history and physical examination alone (if early, spontaneous nystagmus can be observed; if examination done days later, weakness observed with head impulse test) Sometimes gadolinium-enhanced MRI Positional vertigo in neuronitis can be differentiated from BPPV by a Dix-Hallpike maneuver |
Labyrinthitis (viral or bacterial) | Hearing loss, tinnitus | Audiometry Temporal bone CT if purulent infection suspected Gadolinium-enhanced MRI if unilateral hearing loss and tinnitus |
Otitis media (acute or chronic, sometimes with cholesteatoma) | Ear pain, abnormal ear examination, including discharge if chronic otitis History of infection | Audiometry With cholesteatoma, CT to exclude semicircular canal fistula formation |
Trauma (eg, tympanic membrane rupture, labyrinthine contusion, perilymphatic fistula, temporal bone fracture, postconcussion) | Trauma obvious on history Other findings depending on location and extent of damage | Sometimes history and physical examination alone Sometimes CT |
Vestibular schwannoma or meningioma of the posterior fossa or internal auditory canal | Slowly progressive unilateral hearing loss, tinnitus, dizziness, dysequilibrium Rarely, facial numbness, weakness, or both | Audiometry Gadolinium-enhanced MRI if significant hearing asymmetry or unilateral tinnitus |
Treatment with aminoglycosides (eg, gentamycin) recently instituted, usually with bilateral hearing loss and vestibular loss | Audiometry Sometimes vestibular evaluation with electronystagmography and rotary chair tests | |
Also affects geniculate ganglion, so facial weakness and taste loss on the side of the tongue of the facial weakness often manifest along with hearing loss Vertigo possible but not typical Vesicles present on pinna and in ear canal | History and physical examination alone | |
Chronic motion sickness | Persistent symptoms after acute motion sickness | History and physical examination alone |
Central vestibular system disordersd | ||
Brain stem hemorrhage or infarction | Sudden onset Involvement of cochlear artery possibly causing hearing loss and tinnitus | Immediate imaging (gadolinium-enhanced MRI if available, otherwise CT) |
Cerebellar hemorrhage or infarction | Sudden onset, with ataxia and other cerebellar findings, often headache Deteriorates rapidly | Immediate imaging (gadolinium-enhanced MRI if available, otherwise CT) |
Episodic, recurrent vertigo or dizziness, sometimes with unilateral auditory symptoms such as ear fullness and pressure, may have tinnitus that is usually bilateral Need to have prior history of migraine headaches, with ≥ 1 migraine featurese in at least 50% of dizziness/vertigo episodes to diagnose In those without personal history of migraine headaches, family history of migraines is highly suggestive and can make the diagnosis of "probable" vestibular migraine | Usually history and physical examination but with brain imaging as needed to exclude other causes Sometimes trial of migraine prophylaxis | |
Varied CNS motor and sensory deficits, with remissions and recurring exacerbations | Gadolinium-enhanced MRI of brain and spine | |
Vertebral artery dissection | Often head and neck pain and acute, severe imbalance or ataxia | Magnetic resonance angiography |
Vertebrobasilar insufficiency | Intermittent brief episodes, sometimes with drop attacks or extreme imbalance episodes, visual disturbance, confusion | Magnetic resonance angiography |
Global disturbance of CNS functionf | ||
Pallor, weakness, sometimes heme-positive stool | Complete blood count | |
CNS-active medicationsg (not ototoxic) | Medication recently instituted or dose increased; multiple medications, particularly in an older patient Symptoms unrelated to movement or position | Sometimes history and physical examination alone Sometimes medications levels (certain antiseizure medications) Sometimes trial of withdrawal |
Hypoglycemia (usually caused by medications for diabetes) | Recent dose increase Sometimes sweating | Fingerstick glucose test (during symptoms if possible) |
Hypotension (caused by cardiac disorders, antihypertensives, blood loss, dehydration, or orthostatic hypotension syndromes including postural orthostatic tachycardia syndrome and other dysautonomias) | Symptoms on rising from seated or supine, sometimes with vagal stimulation (eg, urination) but not with head motion or while recumbent Manifestation possibly dominated by cause (eg, blood loss, diarrhea) | Orthostatic vital signs, sometimes with tilt table test, ECG |
Tachypnea Often history of lung disease | Pulse oximetry Chest radiograph | |
Other causesf | ||
Persistent perceptual postural dizziness (PPPD) | Chronic non-spinning dizziness (an internal sensation of swaying) persisting for > 3 months, on most days Symptoms worse when standing still, especially while in line, with active (head movement) or passive motion (eg, driving past street lights at night, cars passing while the patient is stopped) or with visual stimulation (eg,, when entering a grocery store) Often precipitated by other acute conditions such as BPPV or vestibular migraine Can be a manifestation of anxiety disorder | History and physical examination alone |
Pregnancy | May be unrecognized | Pregnancy test |
Psychiatric (eg, panic attack, hyperventilation syndrome, anxiety, depression) | Symptoms chronic, brief, recurrent Unrelated to movement or position but may occur with stress or upset Neurologic and otologic examinations normal Initially, patient may be diagnosed with peripheral vestibular dysfunction and fail to respond to appropriate management | History and physical examination alone |
Chronic symptoms with bilateral hearing loss, fluctuating, with episodic vertigo | Audiometry Syphilis serology | |
Weight change Heat or cold intolerance | Thyroid function testing | |
Uncompensated peripheral vestibular weakness | Dysequilibrium Visual blurring (an internal sensation of swaying) with head turning Can follow episodes of vestibular neuronitis, migraine with vertigo, Meniere disease or after head trauma or inner ear surgery | Vestibular testing |
a Symptoms are typically paroxysmal, severe, and episodic rather than continuous. Ear symptoms (eg, tinnitus, fullness, hearing loss) usually indicate a peripheral disorder. Loss of consciousness is not associated with dizziness due to peripheral vestibular pathology. | ||
b Peripheral vestibular system disorders are listed in rough order of frequency of occurrence. | ||
c Numerous medications, including aminoglycosides, chloroquine, furosemide, and quinine. Many other medications are ototoxic but have more effect on the cochlea than the vestibular apparatus.Numerous medications, including aminoglycosides, chloroquine, furosemide, and quinine. Many other medications are ototoxic but have more effect on the cochlea than the vestibular apparatus. | ||
d Ear symptoms are rarely present, but gait/balance disturbance is common. Nystagmus is not inhibited by visual fixation. | ||
e Migraine features include photophobia, phonophobia, visual or other auras, unilateral pulsating or throbbing headache, or severity of headache that limits normal activity. | ||
f These causes should not cause otic symptoms (eg, hearing loss, tinnitus) or focal neurologic deficits (sometimes occurs with hypoglycemia). Vertiginous symptoms are rare but have been reported. | ||
g There are numerous medications, including most antianxiety, antiseizure, antidepressant, antipsychotic, and sedative medications. Medications used to treat vertigo are also included. | ||
BPPV = benign paroxysmal positional vertigo; CNS = central nervous system; CT = computed tomography; ECG = electrocardiography; MRI = magnetic resonance imaging; URI = upper respiratory infection. | ||
Etiology references
1. Çakır S, Sahin A, Gedik-Soyuyuce O, et al. Assessing the impact of migraine on benign paroxysmal positional vertigo symptoms and recovery. BMC Neurol 24(1):148, 2024. https://doi.org/10.1186/s12883-024-03606-2
2. Kim SY, Lee CH, Yoo DM, et al. Association Between Meniere Disease and Migraine. JAMA Otolaryngol Head Neck Surg 148(5):457–464, 2022. doi:10.1001/jamaoto.2022.0331
3. Neuhauser HK. Chapter 5. The epidemiology of dizziness and vertigo. In: Handbook of Clinical Neurology, 2016 Vol. 137 (3rd series), Neuro-Otology J.M. Furman and T. Lempert, Editors http://dx.doi.org/10.1016/B978-0-444-63437-5.00005-4
4. Formeister EJ, Rizk HG, Kohn MA, Sharon JD. The Epidemiology of Vestibular Migraine: A Population-based Survey Study. Otol Neurotol 39(8):1037-1044, 2018. doi:10.1097/MAO.0000000000001900
5. Shoair OA, Nyandege AN, Slattum PW. Medication-Related Dizziness in the Older Adult. Otolaryngol Clin North Am 44(2):455-471, 2011. doi:10.1016/j.otc.2011.01.014
6. Popkirov S, Staab JP, Stone J. Persistent postural-perceptual dizziness (PPPD): a common, characteristic and treatable cause of chronic dizziness. Pract Neurol 18(1):5-13, 2018. doi:10.1136/practneurol-2017-001809
7. Davalos-Bichara M, Agrawal Y. Normative Results of Healthy Older Adults on Standard Clinical Vestibular Tests. Otol Neurotol 35(2):297-300, 2014. doi:10.1097/MAO.0b013e3182a09ca8
8. Lin HW, Bhattacharyya N. Impact of dizziness and obesity on the prevalence of falls and fall-related injuries. Laryngoscope 124(12):2797-2801, 2014. doi:10.1002/lary.24806
9. Feng S, Zang J. The effect of accompanying anxiety and depression on patients with different vestibular syndromes. Front Aging Neurosci 15:1208392, 2023. doi:10.3389/fnagi.2023.1208392
Evaluation of Dizziness and Vertigo
History
History of present illness should cover the sensations felt; an open-ended question is best (eg, “Different people use the word ‘dizziness’ differently. Can you please describe as thoroughly as you can what you feel?”). Brief, specific questioning as to whether the feeling is faintness, light-headedness, loss of balance, or vertiginous may bring some clarity, but persistent efforts to categorize a patient’s sensations are unnecessary. Other elements are more valuable and clear-cut:
Severity of initial episode
Severity and characteristics of subsequent episodes
Symptoms continuous or episodic
If episodic, frequency and duration
Triggers and relievers (ie, caused by head/body position change)
Associated aural symptoms (eg, hearing loss, ear fullness, tinnitus)
Severity and related disability
Is the patient having a single, sudden, acute event, or has dizziness been chronic and recurrent? Was the first episode the most severe (vestibular crisis)? How long do episodes last, and what seems to trigger and worsen them? The patient should be asked specifically about movement of the head, arising, being in anxious or stressful situations, and menses. Important associated symptoms include headache, hearing loss, tinnitus, nausea and vomiting, impaired vision, focal weakness, and difficulty walking. The severity of impact on the patient’s life should be estimated: Has the patient fallen? Is the patient reluctant to drive or leave the house? Has the patient missed work days?
Symptoms of disorders that cause dizziness have a high degree of overlap; thus, identifying the exact timing, frequency, duration, and characteristics of episodes is necessary to establish the diagnosis. Most disorders that cause dizziness are diagnosed clinically. More than one dizziness diagnosis is often present, particularly in chronic dizziness. For example, Meniere disease and BPPV are much more common in patients with migraine compared to the general population (1, 2).
Review of systems should seek symptoms of causative disorders, including symptoms of upper respiratory infection (inner ear disorders); chest pain, palpitations, or both (heart disease); dyspnea (lung disease); dark stools (anemia caused by gastrointestinal blood loss); and weight change or heat or cold intolerance (thyroid disease).
Past medical history should note presence of recent head trauma (usually obvious by history), migraine, diabetes, heart or lung disease, anxiety or depression, and drug or alcohol use disorders. In addition to identifying all current medications, medication history should assess recent changes in medications, doses, or both.
Physical examination
Examination begins with a review of vital signs, including presence of fever, rapid or irregular pulse, and supine and standing blood pressure, noting any drop in blood pressure on standing up (orthostatic hypotension) and whether standing provokes symptoms. If standing does provoke symptoms, postural symptoms should be distinguished from those caused by head movement by returning the patient supine until symptoms dissipate and then rotating the head.
The otologic and neurologic examinations are fundamental. Specifically, with the patient supine, the eyes are checked for presence, direction, and duration of spontaneous nystagmus. Direction and duration of nystagmus and development of vertigo are noted. The Dix-Hallpike maneuver is used to diagnose posterior canal BPPV (by far the most common canal affected) or anterior canal BPPV while the supine roll test can be used to diagnose horizontal canal BPPV.
A gross bedside hearing test is done, the ear canal is inspected for discharge and foreign body, and the tympanic membrane is checked for signs of infection or perforation.
Cerebellar function is tested by assessing gait and doing a finger-nose test and the Romberg test (see How to Assess Sensation). The Fukuda stepping test (marching in place with eyes closed) may be done by specialists to help detect a unilateral vestibular lesion. The remainder of the neurologic examination is done, including testing the rest of the cranial nerves. Use of the HINTS exam (Head Impulse, Nystagmus, Test of Skew exam) is a highly sensitive and specific bedside examination that can differentiate a central cause from a peripheral vestibular cause (3). Specifically, a normal horizontal head impulse test, direction changing nystagmus in eccentric gaze, or vertical skew deviation are all highly suggestive of a central (cerebrovascular, brain tumor, structural lesion) as opposed to a peripheral etiology.
Red flags
The following findings are of particular concern:
Head or neck pain
Ataxia
Loss of consciousness
Focal neurologic deficit
Severe, continuous symptoms for > 1 hour
Interpretation of findings
Differential diagnosis is often based on the exact nature of the chief problem (ie, distinguishing dizziness from light-headedness from vertigo). However, the inconsistency of patients’ descriptions and the poor specificity of symptoms make this approach unreliable. A better approach places more weight on the onset and timing of symptoms, the factors that induce symptoms, and associated symptoms and findings, particularly otologic and neurologic ones.
Some constellations of findings are highly suggestive (see table ), particularly those that help differentiate peripheral from central vestibular disorders.
Peripheral: Ear symptoms (eg, tinnitus, fullness, hearing loss) usually indicate a peripheral disorder. They are typically associated with vertigo and not generalized dizziness (unless caused by uncompensated peripheral vestibular weakness). Symptoms are usually paroxysmal, severe, and episodic; continuous dizziness is rarely due to peripheral vertigo. Loss of consciousness is not associated with dizziness due to peripheral vestibular pathology, and another diagnosis must be sought if this is the symptom described.
Central: Ear symptoms are rarely present, but gait/balance disturbance is common. Nystagmus is not inhibited by visual fixation.
Testing
Patients with a sudden, ongoing attack should have pulse oximetry and fingerstick glucose test. Female patients should have a pregnancy test. Most clinicians also do electrocardiography (ECG). Other tests are done based on findings (see table ), but generally gadolinium-enhanced magnetic resonance imaging (MRI) is indicated for patients with acute symptoms who have headache, neurologic abnormalities, or any other findings suggestive of a central nervous system etiology.
Patients with chronic symptoms of central vestibular pathology should have gadolinium-enhanced MRI to look for evidence of stroke, multiple sclerosis, or other central nervous system lesions.
Patients for whom results of bedside tests of hearing and vestibular function are abnormal or equivocal should undergo formal testing with audiometry and electronystagmography.
ECG, Holter monitoring for heart rhythm abnormalities, echocardiography, and exercise stress testing may be done to evaluate heart function.
Laboratory tests are rarely helpful, except for patients with chronic vertigo and bilateral hearing loss, for whom syphilis serology is indicated.
Evaluation references
1. Kim SK, Hong SM, Park IS, Choi HG. Association Between Migraine and Benign Paroxysmal Positional Vertigo Among Adults in South Korea. JAMA Otolaryngol Head Neck Surg 2019;145(4):307-312. doi:10.1001/jamaoto.2018.4016
2. Radtke A, Lempert T, Gresty MA, Brookes GB, Bronstein AM, Neuhauser H. Migraine and Ménière's disease: is there a link? Neurology 2002;59(11):1700-1704. doi:10.1212/01.wnl.0000036903.22461.39
3. Kattah JC, Talkad AV, Wang DZ, Hsieh YH, Newman-Toker DE. HINTS to diagnose stroke in the acute vestibular syndrome: three-step bedside oculomotor examination more sensitive than early MRI diffusion-weighted imaging. Stroke 2009;40(11):3504-3510. doi:10.1161/STROKEAHA.109.551234
Treatment of Dizziness and Vertigo
Treatment of dizziness and vertigo is directed at the cause, including stopping, reducing, or switching any causative medications.
If a vestibular disorder is present and thought to be secondary to active Meniere disease or vestibular neuronitis or labyrinthitis, the most effective vestibular nerve suppressants are oral antihistamine/anticholinergic medications (eg, meclizine, promethazine) or benzodiazepines (eg, diazepam, clonazepam). All of these medications can cause drowsiness, thereby limiting their use for certain patients. These medications should only be used during acute vertigo episodes (Meniere disease) or during the first few days of symptoms (vestibular neuronitis or labyrinthitis), as chronic use of these vestibular suppressants inhibit central compensation and can prolong symptoms. , the most effective vestibular nerve suppressants are oral antihistamine/anticholinergic medications (eg, meclizine, promethazine) or benzodiazepines (eg, diazepam, clonazepam). All of these medications can cause drowsiness, thereby limiting their use for certain patients. These medications should only be used during acute vertigo episodes (Meniere disease) or during the first few days of symptoms (vestibular neuronitis or labyrinthitis), as chronic use of these vestibular suppressants inhibit central compensation and can prolong symptoms.
Nausea can be treated with prochlorperazine or ondansetron . Nausea can be treated with prochlorperazine or ondansetron .
Vertigo associated with benign paroxysmal positional vertigo is treated with the Epley maneuver (otolith repositioning) done by an experienced professional (eg, a vestibular physical therapist). Sometimes patients are taught self-treatment maneuvers. Medications are not indicated for patients with isolated BPPV.
Meniere disease is best managed by an otolaryngologist with training in management of this chronic disorder, but initial management typically consists of a low-salt diet and a potassium-sparing diuretic, or betahistine (1).
Patients with vestibular migraine should be referred to a neurologist for management. Calcitonin gene-related peptide (CGRP) inhibitors may be effective at treating vestibular symptoms in vestibular migraine (2).
If a component of underlying anxiety or depression is suspected, patients should be appropriately treated, either through their primary care provider or through a psychiatrist.
Patients with persistent or recurrent vertigo secondary to unilateral vestibular weakness (such as secondary to vestibular neuronitis) benefit from vestibular rehabilitation therapy done by an experienced vestibular physical therapist. Most patients compensate well, although some, especially older patients, have more difficulty. Physical therapy can also provide important safety information for older patients or particularly disabled patients. Vestibular rehabilitation therapy is also highly effective for other chronic dizziness disorders, including non-peripheral etiologies such as vestibular migraine (3) and PPPD (4).
Treatment references
1. Basura GJ, Adams ME, Monfared A, et al. Clinical Practice Guideline: Ménière's Disease. Otolaryngol Head Neck Surg 162(2_suppl):S1-S55, 2020. doi: 10.1177/0194599820909438
2. Russo CV, Saccà F, Braca S, et al. Anti-calcitonin gene-related peptide monoclonal antibodies for the treatment of vestibular migraine: A prospective observational cohort study. Cephalalgia p43(4):3331024231161809, 2023. doi: 10.1177/03331024231161809
3. Balci B, Akdal G. Outcome of vestibular rehabilitation in vestibular migraine. J Neurol 269(12):6246-6253, 2022. doi:10.1007/s00415-022-11250-4
4. Ibrahim NMK, Hazza NMA, Yaseen DM, Galal EM. Effect of vestibular rehabilitation games in patients with persistent postural perceptual dizziness and its relation to anxiety and depression: prospective study. Eur Arch Otorhinolaryngol 281(6):2861-2869, 2024. doi: 10.1007/s00405-023-08369-z
Geriatrics Essentials: Dizziness and Vertigo
As people age, organs involved in balance function less well. For example, seeing in dim light becomes more difficult, inner ear structures deteriorate, proprioception becomes less sensitive, and mechanisms that control blood pressure become less responsive (eg, to postural changes, postprandial demands). Older adults also are more likely to have cardiac or cerebrovascular disorders that can contribute to dizziness. They also are more likely to be taking medications that can cause dizziness, including those for hypertension, angina, heart failure, seizures, and anxiety, as well as certain antibiotics, antihistamines, and sleep aids. Thus, dizziness in older patients usually has more than one cause.
Although unpleasant at any age, the consequences of dizziness and vertigo are a particular problem for older patients. Patients with frailty are at significant risk of falling with consequent fractures; their fear of moving and falling often significantly decreases their ability to do daily activities.
In addition to treatment of specific causes, older patients with dizziness or vertigo may benefit from physical therapy and exercises to strengthen muscles and help maintain independent ambulation as long as possible.
Key Points
Vague or inconsistently described symptoms may still be associated with a serious condition.
Cerebrovascular disease and medication effects should be sought, particularly in older patients.
Peripheral vestibular system disorders should be differentiated from central vestibular system disorders.
Immediate neuroimaging should be done when symptoms are accompanied by headache, focal neurologic abnormalities, or both.
Drug Information for the Topic





