

Ventricular tachycardia is ≥ 3 consecutive ventricular beats at a rate ≥ 120 beats/minute. Symptoms depend on duration and vary from none to palpitations to hemodynamic collapse and death. Diagnosis is by electrocardiography. Treatment of more than brief episodes is with cardioversion or antiarrhythmics, depending on symptoms. If necessary, long-term treatment is with an implantable cardioverter defibrillator.
(See also Overview of Arrhythmias.)
Some experts use a cutoff rate of ≥ 100 beats/minute for ventricular tachycardia (VT). Repetitive ventricular rhythms at slower rates are called accelerated idioventricular rhythms or slow VT; they are usually benign and are not treated unless patients have hemodynamic symptoms.
Most patients with VT have a significant heart disorder, particularly prior myocardial infarction or a cardiomyopathy. Electrolyte abnormalities (particularly hypokalemia or hypomagnesemia), acidemia, hypoxemia, and adverse medication effects contribute (1). The long QT syndrome (congenital or acquired) is associated with a particular form of VT, torsades de pointes.
Ventricular tachycardia may be monomorphic or polymorphic and nonsustained or sustained.
Monomorphic VT: Single abnormal focus or reentrant pathway and thus regular, identical-appearing QRS complexes
Polymorphic VT: Several different foci or pathways and thus irregular, varying QRS complexes
Nonsustained VT: Lasts < 30 seconds
Sustained VT: Lasts ≥ 30 seconds or is terminated sooner because of hemodynamic collapse
Right and left ventricular outflow tract ventricular tachycardia (RVOT-VT and LVOT-VT) are idiopathic ventricular tachycardias that occur in the absence of an evident underlying structural heart disorder (2). They are due to cAMP-mediated delayed after-depolarizations and usually occur with exercise or emotional stress (2). They typically have a morphology that is similar to left bundle branch block (LBBB) and a vertical downward axis (positive QRS in lead V1, negative QRS in lead AVL, and near-isoelectric QRS in lead I) (see Ventricular Premature Beats).
Verapamil-sensitive left fascicular VT (Belhassen VT, left septal VT) is an idiopathic ventricular tachycardia that occurs in the absence of an evident underlying structural heart disorder (Verapamil-sensitive left fascicular VT (Belhassen VT, left septal VT) is an idiopathic ventricular tachycardia that occurs in the absence of an evident underlying structural heart disorder (3). It is due to a slow conduction section of abnormal Purkinje tissue that can support macro-reentry using ventricular myocardium and part of the left (usually posterior) hemifascicle of the left bundle branch. It is typically induced by a critical heart rate either spontaneously or by rapid atrial pacing and usually has a morphology similar to that of right bundle branch block with left axis deviation (3).
Bundle branch reentry VT is a ventricular tachycardia that occurs in patients with advanced cardiomyopathy or isolated conduction system disease (3). It is due to macro-reentry using the bundle branches, usually the antegrade limb is the right bundle branch and the retrograde limb is the left bundle branch. Accordingly, this ventricular tachycardia usually has a LBBB-like QRS morphology (3).
Catecholaminergic polymorphic ventricular tachycardia is a genetic disorder affecting intracellular calcium regulation in cardiac tissue. Patients are predisposed to atrial and/or ventricular tachyarrhythmias and sudden cardiac death, particularly during increased adrenergic activity. (See also Arrhythmogenic Cardiac Disorders.)
VT frequently deteriorates to ventricular fibrillation and thus cardiac arrest.
General references
1. Al-Khatib SM, Stevenson WG, Ackerman MJ, et al: 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol 72:e91–e220, 2018. doi: 10.1016/j.jacc.2017.10.054
2. Lerman BB: Mechanism, diagnosis, and treatment of outflow tract tachycardia. Nat Rev Cardiol 12(10):597–608, 2015. doi: 10.1038/nrcardio.2015.121
3. Sung RK, Boyden PA, Scheinman M: Cellular Physiology and Clinical Manifestations of Fascicular Arrhythmias in Normal Hearts. JACC Clin Electrophysiol 3(12):1343–1355, 2017. doi: 10.1016/j.jacep.2017.07.011
Symptoms and Signs of Ventricular Tachycardia
Ventricular tachycardia of short duration or slow rate may be asymptomatic. Sustained VT is almost always symptomatic, causing palpitations, symptoms of hemodynamic compromise, or sudden cardiac death.
Diagnosis of Ventricular Tachycardia
Electrocardiography (ECG)
Diagnosis of ventricular tachycardia is by ECG (see figure ). Any wide QRS complex tachycardia (QRS ≥ 0.12 second) should be considered VT until proved otherwise.
Pearls & Pitfalls
|
Diagnosis is supported by ECG findings of
Dissociated P-wave activity
Fusion beats (a conducted sinus beat fusing with a ventricular beat creating a QRS complex with morphology, duration, and axis in-between those of normally conducted beats and those of the wide QRS complex ventricular beats)
Capture beats (normally conducted sinus beat interrupting a wide-complex tachycardia)
Uniformity of QRS vectors in the V leads (concordance) with discordant T-wave vector (opposite QRS vector)
A frontal-plane QRS axis in the northwest quadrant
Differential diagnosis includes fast supraventricular rhythms conducted with bundle branch block or via an accessory pathway (see figure ) (1). Because some patients tolerate VT surprisingly well, concluding that a well-tolerated wide QRS complex tachycardia must be of supraventricular origin is a mistake. Using medications appropriate for supraventricular tachycardia (eg, verapamil, diltiazem) in patients with VT may cause hemodynamic collapse and death (). Because some patients tolerate VT surprisingly well, concluding that a well-tolerated wide QRS complex tachycardia must be of supraventricular origin is a mistake. Using medications appropriate for supraventricular tachycardia (eg, verapamil, diltiazem) in patients with VT may cause hemodynamic collapse and death (2). Still, because of its very brief half-life, IV adenosine may be used as a diagnostic maneuver (and possibly treatment, if the arrhythmia is supraventricular) in a patient who is stable and has a regular, monomorphic wide QRS complex tachycardia (). Still, because of its very brief half-life, IV adenosine may be used as a diagnostic maneuver (and possibly treatment, if the arrhythmia is supraventricular) in a patient who is stable and has a regular, monomorphic wide QRS complex tachycardia (3), albeit with a small risk of converting stable VT to unstable ventricular fibrillation.
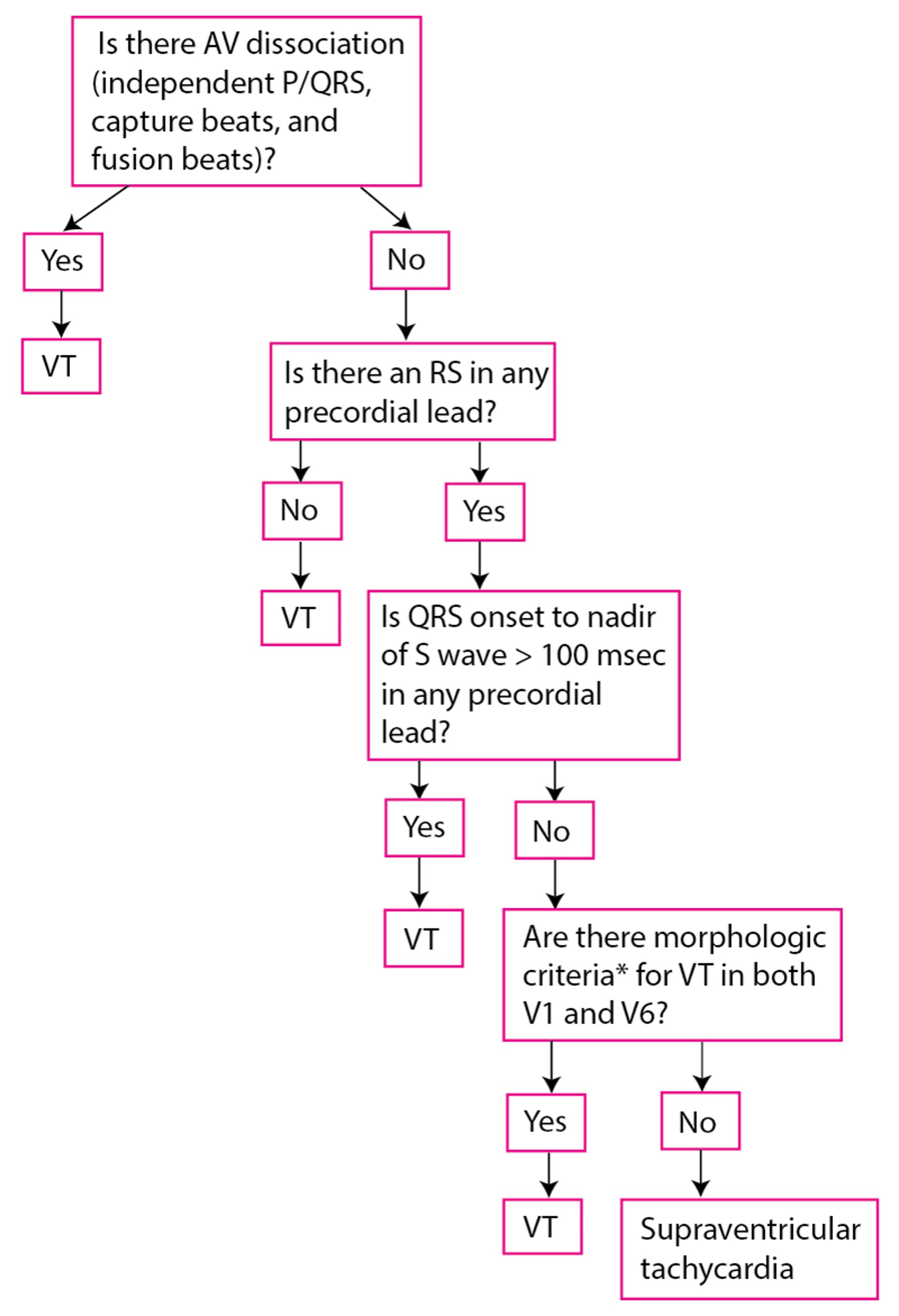
Modified Brugada Criteria for Ventricular Tachycardia
*With RBBB QRS:
*With LBBB QRS:
|
AV = atrioventricular; LBBB = left bundle branch block; msec = millisecond; RBBB = right bundle branch block; VT = ventricular tachycardia. Data from Brugada P, Brugada J, Mont L, Smeets J, Andries EW. A new approach to the differential diagnosis of a regular tachycardia with a wide QRS complex. Circulation. 1991;83(5):1649-1659. doi:10.1161/01.cir.83.5.1649 |

Pearls & Pitfalls
|
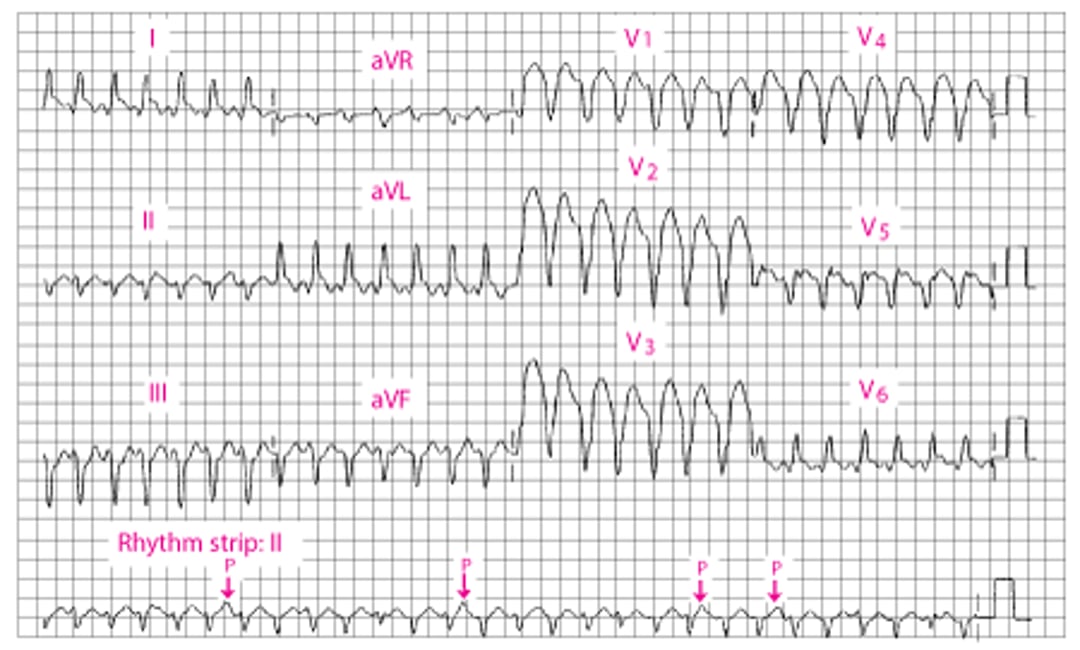
Broad QRS Ventricular Tachycardia
The QRS duration is 160 millisecond. An independent P wave can be seen in II (arrows). There is a leftward mean frontal axis shift. |

Diagnosis references
1. Vereckei A, Simon A, Szénási G, et al: The Application of a New, Modified Algorithm for the Differentiation of Regular Ventricular and Pre-Excited Tachycardias. Heart Lung Circ 32(6):719–725, 2023. doi: 10.1016/j.hlc.2023.03.016
2. Al-Khatib SM, Stevenson WG, Ackerman MJ, et al: 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol 72:e91–e220, 2018. doi: 10.1016/j.jacc.2017.10.054
3. Marill KA, Wolfram S, Desouza IS, et al: Adenosine for wide-complex tachycardia: efficacy and safety. Crit Care Med 37:2512–2518, 2009. doi: 10.1097/CCM.0b013e3181a93661
Treatment of Ventricular Tachycardia
Acute: Sometimes synchronized direct current cardioversion, sometimes class I or class III antiarrhythmics
Long-term: Usually an implantable cardioverter-defibrillator
Acute
Treatment of acute ventricular tachycardia depends on symptoms and duration of VT.
Pulseless VT requires defibrillation beginning with biphasic 120 to 200 joules (or monophasic 360 joules).
Stable sustained VT can be treated with synchronized direct current cardioversion with ≥100 joules using conscious sedation or transient general anesthesia.
Stable sustained VT can be treated with intravenous class I or class III antiarrhythmics (1) (see table ). Lidocaine acts quickly but is frequently ineffective. If ). Lidocaine acts quickly but is frequently ineffective. Iflidocaine is ineffective, IV procainamide may be given, but it may take up to 1 hour to work. IV amiodarone is frequently used but does not usually work quickly. Failure of IV is ineffective, IV procainamide may be given, but it may take up to 1 hour to work. IV amiodarone is frequently used but does not usually work quickly. Failure of IVprocainamide or IV amiodarone is an indication for cardioversion. Right and left ventricular outflow tract ventricular tachycardias (RVOT-VT and LVOT-VT) respond to IV adenosine. Verapamil-sensitive left fascicular ventricular tachycardia responds to IV verapamil (is an indication for cardioversion. Right and left ventricular outflow tract ventricular tachycardias (RVOT-VT and LVOT-VT) respond to IV adenosine. Verapamil-sensitive left fascicular ventricular tachycardia responds to IV verapamil (1).
Nonsustained VT does not require immediate treatment unless the runs are frequent or long enough to cause symptoms. In such cases, antiarrhythmics are used as for sustained VT.
Long-term
The primary goal is preventing sudden death, rather than simply suppressing the arrhythmia. It is best accomplished by use of an implantable cardioverter-defibrillator (ICD). However, the decision about whom to treat is complex and depends on the estimated probability of life-threatening VTs and the severity of underlying heart disorders (1) (see table ).
Long-term treatment is not required when the index episode of ventricular tachycardia resulted from a transient cause (eg, during the 48 hours after onset of myocardial infarction) or a reversible cause (acid-base disturbances, electrolyte abnormalities, proarrhythmic medication effect).
In the absence of a transient or reversible cause, patients who have had an episode of sustained VT typically require an ICD (1). Most patients with sustained VT and a significant structural heart disorder should also receive a beta-blocker. If an ICD cannot be used, amiodarone may be the preferred antiarrhythmic for prevention of sudden death.). Most patients with sustained VT and a significant structural heart disorder should also receive a beta-blocker. If an ICD cannot be used, amiodarone may be the preferred antiarrhythmic for prevention of sudden death.
Because nonsustained VT is a marker for increased risk of sudden death in patients with a structural heart disorder, such patients (particularly those with an ejection fraction < 0.35) require further evaluation. Such patients should receive an ICD.
When prevention of VT is important (usually in patients who have an ICD and are having frequent episodes of VT), antiarrhythmics or transcatheter or surgical ablation of the arrhythmogenic substrate is required (1). Any class Ia, Ib, Ic, II, or III antiarrhythmic can be used. Because beta-blockers (class II) are safe, they are the first choice unless contraindicated. If an additional medication is required, sotalol is commonly used, then amiodarone (can be used. Because beta-blockers (class II) are safe, they are the first choice unless contraindicated. If an additional medication is required, sotalol is commonly used, then amiodarone (1).
Transcatheter ablation is particularly successful in patients who have VT with well-defined syndromes (eg, right or left ventricular outflow tract VT, verapamil-sensitive left fascicular VT, or bundle branch reentrant VT (is particularly successful in patients who have VT with well-defined syndromes (eg, right or left ventricular outflow tract VT, verapamil-sensitive left fascicular VT, or bundle branch reentrant VT (1).

Treatment reference
1. Al-Khatib SM, Stevenson WG, Ackerman MJ, et al: 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol 72:e91–e220, 2018. doi: 10.1016/j.jacc.2017.10.054
Key Points
Any wide-complex (QRS ≥ 0.12 second) tachycardia should be considered ventricular tachycardia (VT) until proved otherwise.
Patients who do not have a pulse should be cardioverted.
Synchronized cardioversion or antiarrhythmic medications may be tried if the patient is stable.
Patients who had an episode of sustained VT without a transient or reversible cause typically require an implantable cardioverter-defibrillator (ICD).





