


Renal cell carcinoma (RCC) is the most common renal cancer. Symptoms can include hematuria, flank pain, a palpable mass, and fever of unknown origin (FUO). However, symptoms are often absent, so the diagnosis is usually suspected based on incidental findings. Diagnosis is confirmed by CT or MRI and occasionally by biopsy. Treatment is with surgery for early disease and systemic therapy, an experimental protocol, or palliative therapy for advanced disease.
RCC, an adenocarcinoma, accounts for 90 to 95% of primary malignant renal tumors. Less common primary renal tumors include transitional cell carcinoma, Wilms tumor (most often in children), and sarcoma.
In the United States, about 81,610 new cases of RCC and other kidney tumors and 14,390 deaths (2024 estimates) occur each year (1). RCC occurs more often in men (male:female incidence is about 2:1). People with RCC are usually diagnosed between 65 and 74 years old. Risk factors include the following:
Smoking, which doubles the risk
Obesity
Excess use of phenacetin
Acquired cystic kidney disease in patients on dialysis
Exposure to certain radiopaque contrast agents, asbestos, cadmium, and leather tanning and petroleum products
Some familial syndromes, particularly von Hippel–Lindau disease and tuberous sclerosis
RCC can trigger thrombus formation in the renal vein, which occasionally propagates into the vena cava. Tumor invasion of the vein wall is uncommon. RCC metastasizes most often to the lymph nodes, lungs, adrenal glands, liver, brain, and bone.
Reference
1. American Cancer Society: Key statistics about kidney cancer. Accessed February 3, 2025.
Signs and Symptoms of Renal Cancer
Symptoms usually do not appear until late, when the tumor may already be large and metastatic. Gross or microscopic hematuria is the most common manifestation, followed by flank pain, fever of unknown origin (FUO), and a palpable mass. Other nonspecific symptoms can include fatigue, weight loss, and early satiety. Sometimes hypertension results from segmental ischemia or pedicle compression. Paraneoplastic syndromes occur in 20% of patients. Polycythemia can result from increased erythropoietin activity. However, anemia may also occur. Hypercalcemia is common and may require treatment. Thrombocytosis, cachexia, or secondary amyloidosis may develop.
Diagnosis of Renal Cancer
CT with contrast or MRI


© Springer Science+Business Media
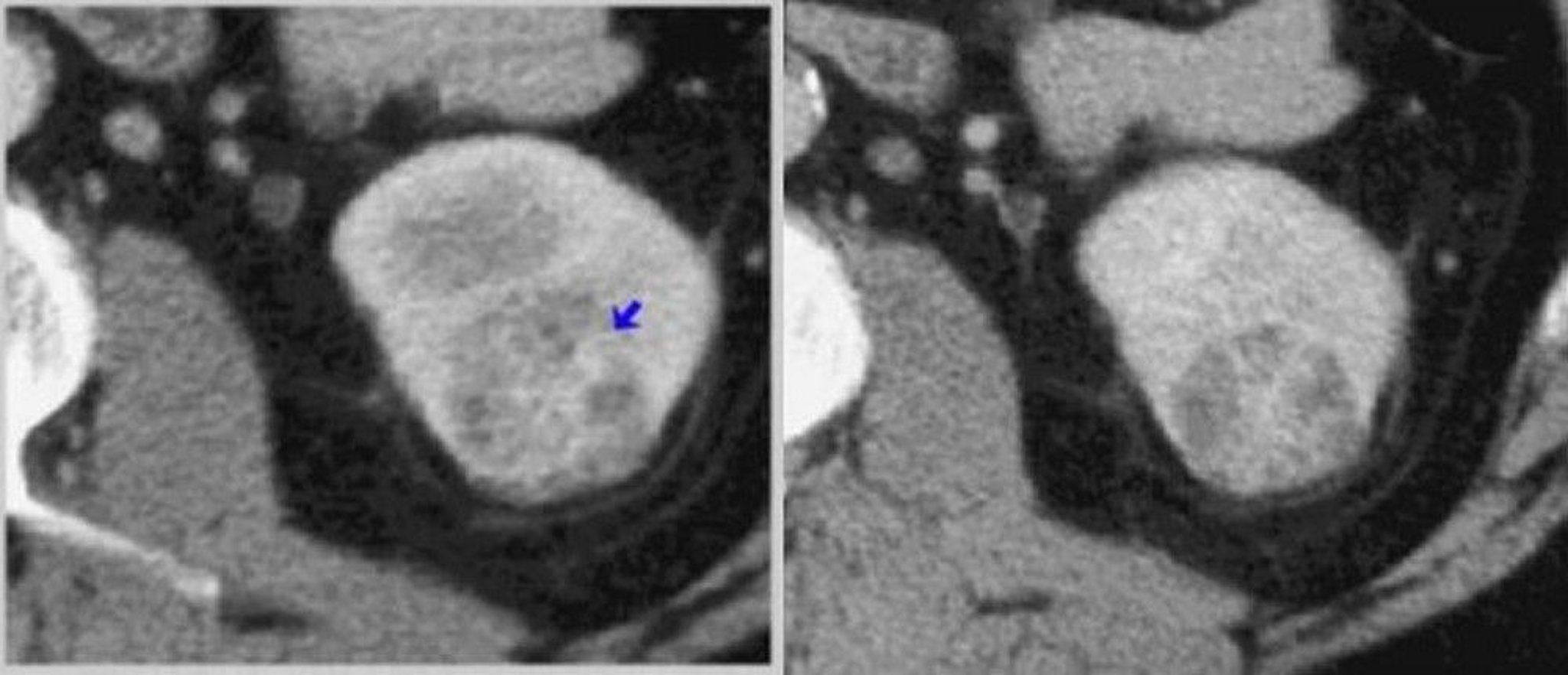
Most often, a renal mass is detected incidentally during abdominal or spinal imaging (eg, CT, ultrasonography, MRI) done for other reasons. Otherwise, diagnosis is suggested by clinical findings and confirmed by abdominal CT before and after injection of a radiocontrast agent or by MRI. (See Genitourinary Imaging Tests.) A renal mass that is enhanced by radiocontrast strongly suggests renal cell carcinoma (RCC). CT and MRI also provide information about local extension and nodal and venous involvement. MRI provides further information about extension into the renal vein and vena cava and has replaced inferior vena cavography. Ultrasonography and intravenous urography may show a mass but provide less information about the characteristics of the mass and extent of disease than do CT or MRI.
Often, nonmalignant and malignant masses can be distinguished radiographically, but sometimes biopsy or surgery is needed for confirmation. Needle biopsy does not have sufficient sensitivity when findings are equivocal; it is recommended only when the diagnosis would impact treatment choice, such as when there is an infiltrative pattern instead of a discrete mass, when the renal mass may be a metastasis from another known cancer, or sometimes to confirm a diagnosis before chemotherapy or systemic therapy for metastatic renal masses.
Three-dimensional CT, CT angiography, or magnetic resonance angiography is used before surgery, particularly before nephron-sparing surgery, to define the nature of RCC, to more accurately determine the number of renal arteries present, and to delineate the vascular pattern. (See Genitourinary Imaging Tests.) These imaging techniques have replaced aortography and selective renal artery angiography.
A chest x-ray and liver tests are essential. If chest x-ray is abnormal, chest CT is done. If alkaline phosphatase is elevated, bone scanning is needed. Serum electrolytes, blood urea nitrogen (BUN), creatinine, and calcium are measured. BUN and creatinine are unaffected unless both kidneys are diseased.
Fluorodeoxyglucose (FDG) PET/CT is not routinely done in most patients with primary RCCs, but it may be beneficial for preoperative staging in high-risk tumors and to assess the response to systemic therapies in metastatic disease. A new PET imaging agent, zirconium-89 (89Zr)-deferoxamine (DFO)-girentuximab, may identify clear cell renal cell carcinoma (ccRCC) with high sensitivity and specificity (Fluorodeoxyglucose (FDG) PET/CT is not routinely done in most patients with primary RCCs, but it may be beneficial for preoperative staging in high-risk tumors and to assess the response to systemic therapies in metastatic disease. A new PET imaging agent, zirconium-89 (89Zr)-deferoxamine (DFO)-girentuximab, may identify clear cell renal cell carcinoma (ccRCC) with high sensitivity and specificity (1).

© Springer Science+Business Media
Staging
Information from the evaluation makes preliminary staging possible. The TNM (tumor, node, metastasis) system has been refined to be precise (see tables AJCC/TNM Staging of Renal Cell Carcinoma and TNM Definitions for Renal Cell Carcinoma). At diagnosis, RCC is localized in 70%, locally invasive in about 20%, and spread to distant organs in 11% of patients (2).
AJCC/TNM* Staging of Renal Cell Carcinoma
Stage | Tumor | Regional Lymph Node Metastasis | Distant Metastasis |
|---|---|---|---|
I | T1 | N0 | M0 |
II | T2 | N0 | M0 |
III | T1–T3 | N1 | M0 |
T3 | N0 | M0 | |
IV | T4 | Any N | M0 |
Any T | Any N | M1 | |
* For AJCC/TNM definitions, see table TNM Definitions for Renal Cell Carcinoma. Data adapted from American Cancer Society, Kidney Cancer Stages and National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology. Kidney Cancer. Version 1.2024. Accessed February 3, 2025. | |||
AJCC = American Joint Commission on Cancer; TNM = tumor, node, metastasis. | |||
TNM Definitions for Renal Cell Carcinoma*
Feature | Definition |
|---|---|
Primary tumor | |
TX | No information to assess primary tumor |
T0 | No evidence of a primary tumor |
T1 | ≤ 7 cm in greatest dimension Limited to kidney |
T1a | ≤ 4 cm in greatest dimension |
T1b | > 4 cm but ≤ 7 cm in greatest dimension |
T2 | ≥ 7 cm in greatest dimension Limited to kidney |
T2a | > 7 cm but ≤ 10 cm in greatest dimension |
T2b | > 10 cm in greatest dimension |
T3 | Extends into major veins or invades perinephric tissues but not beyond Gerota fascia or into the adrenal gland |
T3a | Extends into renal veins or its segmental branches or invades perirenal and/or renal sinus fat, but not beyond Gerota fascia |
T3b | The tumor is growing into the part of the large vein leading into the heart (vena cava) that is within the abdomen |
T3c | The tumor has grown into the part of the vena cava that is within the chest or it is growing into the wall of the vena cava |
T4 | The tumor has spread beyond Gerota’s fascia (the fibrous layer that surrounds the kidney and nearby fatty tissue). The tumor may have grown into the adrenal gland (on top of the kidney). |
Regional lymph node metastasis | |
NX | Not assessable |
N0 | None |
N1 | Present |
Distant metastasis | |
M0 | None |
M1 | Distant metastasis, including spread to distant lymph nodes |
* Data adapted from American Cancer Society, Kidney Cancer Stages and National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology. Kidney Cancer. Version 1.2024 . Accessed February 3, 2025. | |
TNM = tumor, node, metastasis. | |
Diagnosis references
1. Roussel E, Capitanio U, Kutikov A, et al. Novel imaging methods for renal mass characterization: A collaborative review. Eur Urol. 81(5):476-488, 2022. doi: 10.1016/j.eururo.2022.01.040
2. Patel HD, Gupta M, Joice GA, et al. Clinical Stage Migration and Survival for Renal Cell Carcinoma in the United States. Eur Urol Oncol. 2019;2(4):343-348. doi:10.1016/j.euo.2018.08.023
Treatment of Renal Cancer
For early renal cell carcinoma (RCC), surgical treatment, active surveillance, or ablative techniques
For advanced RCC, palliative therapies or experimental protocols
Curative treatments
Radical nephrectomy (removal of kidney, perirenal fat, Gerota fascia +/- ipsilateral adrenal gland) is standard treatment for localized RCC and provides a reasonable chance for cure. Results with open or minimally invasive procedures are comparable; recovery is generally easier with minimally invasive procedures. Nephron-sparing surgery (partial nephrectomy) is possible and appropriate for many patients. Partial nephrectomy is gaining popularity because it results in a lower incidence of chronic kidney disease than radical nephrectomy. It is the standard of care for clinically staged T1a tumors (cT1a, < 4 cm) and should be considered in patients with T1b or T2 tumors and those with absolute indications for nephron preservation (eg, bilateral renal masses, CKD, solitary kidney). Radical nephrectomy should be considered in patients with a normal contralateral kidney, normal kidney function, and more advanced primary tumors (cT1b through cT4).
Nonsurgical destruction of renal tumors via freezing (cryosurgery) or thermal energy (radiofrequency ablation), often percutaneously, should be considered for tumors smaller than 3 cm. For small renal masses, active surveillance (with delayed intervention) should be considered a first-line treatment option, particularly if active treatments pose risks and/or patients have significant comorbidities. Decision-making for treatment is complex and multifactorial and typically involves shared decision-making (1).
For tumors involving the renal vein and vena cava, surgery may be curative if no nodal or distant metastases exist.
If both kidneys are affected, partial nephrectomy of one or both kidneys is preferable to bilateral radical nephrectomy if technically feasible.
Adjuvant use of targeted therapy after surgery has failed to prolong survival in multiple clinical trials, yet improvements in disease-free survival seen in patients taking adjuvant sunitinib in S-TRAC led to its approved use following resection in high-risk patients (Adjuvant use of targeted therapy after surgery has failed to prolong survival in multiple clinical trials, yet improvements in disease-free survival seen in patients taking adjuvant sunitinib in S-TRAC led to its approved use following resection in high-risk patients (2). Its use has been limited. The KEYNOTE-564 study (3) showed robust increases in disease-free survival and overall survival in patients treated with pembrolizumab as an adjuvant therapy for surgically treated clear cell RCC patients at high risk of recurrence (localized clear cell RCC with sarcomatoid features; International Society of Urological Pathology (ISUP) Grade 4 histopathology; or completely resected locally advanced or metastatic RCC).) showed robust increases in disease-free survival and overall survival in patients treated with pembrolizumab as an adjuvant therapy for surgically treated clear cell RCC patients at high risk of recurrence (localized clear cell RCC with sarcomatoid features; International Society of Urological Pathology (ISUP) Grade 4 histopathology; or completely resected locally advanced or metastatic RCC).
Palliative treatments
Palliation can include nephrectomy, tumor embolization, external beam radiation therapy and systemic therapy. Resection of metastases offers palliation and, if metastases are limited in number, prolongs life in some patients, particularly those with a long interval between initial treatment (nephrectomy) and development of metastases. Although metastatic RCC is traditionally characterized as radioresistant, radiation therapy can be palliative when RCC is oligometastatic, particularly to the bone.
Systemic therapies are the mainstay of management of patients with metastatic RCC. Drug therapy reduces tumor size and prolongs life. About 10 to 20% of patients respond to interferon alfa-2b or IL-2, although the response is long-lasting in Systemic therapies are the mainstay of management of patients with metastatic RCC. Drug therapy reduces tumor size and prolongs life. About 10 to 20% of patients respond to interferon alfa-2b or IL-2, although the response is long-lasting in< 5% (4). Many targeted therapies have shown efficacy for advanced tumors: sunitinib, sorafenib, bevacizumab, pazopanib, cabozantinib, axitinib, and lenvatinib (tyrosine kinase inhibitors) and temsirolimus and everolimus, which inhibit the mammalian target of rapamycin (mTOR) (). Many targeted therapies have shown efficacy for advanced tumors: sunitinib, sorafenib, bevacizumab, pazopanib, cabozantinib, axitinib, and lenvatinib (tyrosine kinase inhibitors) and temsirolimus and everolimus, which inhibit the mammalian target of rapamycin (mTOR) (4).
However, the newest available systemic therapies for metastatic RCC are immune checkpoint inhibitors (ICI) (4). These monoclonal antibodies against PD-1 or PD-L1 work by blocking the PD-1/PD-L1 interaction between tumor cells and infiltrating T-cells, thus blocking PD-1 pathway-mediated inhibition of the immune response, including the antitumor immune response. First-line systemic treatments for patients with metastatic RCC are combination therapies (ICI +/- targeted therapy, chemotherapy, or a second ICI); combinations include pembrolizumab + axitinib, nivolumab + cabozantinib, pembrolizumab + levantinib, and ipilimumab + cabozantonib. Choice of combination is based on determination of risk for recurrent metastatic disease (favorable, intermediate, or poor risk) as defined by the International Metastatic RCC Database Consortium risk criteria. In certain patients, complete surgical resection (including metastases) or a combination of surgery and radiation for all sites of disease can be considered in lieu of systemic therapy. Clinical trials are needed.). These monoclonal antibodies against PD-1 or PD-L1 work by blocking the PD-1/PD-L1 interaction between tumor cells and infiltrating T-cells, thus blocking PD-1 pathway-mediated inhibition of the immune response, including the antitumor immune response. First-line systemic treatments for patients with metastatic RCC are combination therapies (ICI +/- targeted therapy, chemotherapy, or a second ICI); combinations include pembrolizumab + axitinib, nivolumab + cabozantinib, pembrolizumab + levantinib, and ipilimumab + cabozantonib. Choice of combination is based on determination of risk for recurrent metastatic disease (favorable, intermediate, or poor risk) as defined by the International Metastatic RCC Database Consortium risk criteria. In certain patients, complete surgical resection (including metastases) or a combination of surgery and radiation for all sites of disease can be considered in lieu of systemic therapy. Clinical trials are needed.
Other treatments are experimental. They include stem cell transplantation, other interleukins, anti-angiogenesis therapy (eg, thalidomide), and vaccine therapy. Traditional chemotherapeutic drugs, alone or combined, and progestins are ineffective. , other interleukins, anti-angiogenesis therapy (eg, thalidomide), and vaccine therapy. Traditional chemotherapeutic drugs, alone or combined, and progestins are ineffective.
Cytoreductive nephrectomy before systemic therapy is controversial now that CARMENA (Clinical Trial to Assess the Importance of Nephrectomy), a randomized phase III trial comparing cytoreductive nephrectomy followed by sunitinib and sunitinib alone, showed survival was not worse when treating with sunitinib alone (Cytoreductive nephrectomy before systemic therapy is controversial now that CARMENA (Clinical Trial to Assess the Importance of Nephrectomy), a randomized phase III trial comparing cytoreductive nephrectomy followed by sunitinib and sunitinib alone, showed survival was not worse when treating with sunitinib alone (5); however, that trial was criticized for its patient selection (heavily enriched with poor-risk patients with minimal inclusion of intermediate-risk patients).
The current recommendations are to consider cytoreductive nephrectomy before systemic therapy in patients with any of the following criteria (4):
Higher disease burden in the kidney
Symptomatic bleeding or pain from the primary tumor
Presence of a paraneoplastic syndrome associated with the primary tumor
Excellent performance status with normal contralateral kidney function
Increased knowledge of genetic subtypes of RCC is leading to evolving management recommendations that are more specific.
Treatment references
1. Chandrasekar T, Boorjian SA, Capitanio U, et al: Collaborative review: Factors influencing treatment decisions for patients with a localized solid renal mass. Eur Urol. 80(5):575-588, 2021. doi: 10.1016/j.eururo.2021.01.021
2. Ravaud A, Motzer RJ, Pandha HS et al: Adjuvant sunitinib in high-risk renal-cell carcinoma after nephrectomy. : Adjuvant sunitinib in high-risk renal-cell carcinoma after nephrectomy.N Engl J Med. 8;375(23):2246-2254, 2016. doi: 10.1056/NEJMoa1611406
3. Choueiri TK, Tomczak P, Park SH, et al for the KEYNOTE-564 Investigators: Adjuvant pembrolizumab after nephrectomy in renal-cell carcinoma. : Adjuvant pembrolizumab after nephrectomy in renal-cell carcinoma.N Engl J Med . 385(8):683-694, 2021. doi: 10.1056/NEJMoa2106391
4. Rathmell WK, Rumble RB, Van Veldhuizen PJ, et al. Management of Metastatic Clear Cell Renal Cell Carcinoma: ASCO Guideline. J Clin Oncol. 2022;40(25):2957-2995. doi:10.1200/JCO.22.00868
5. Mejean A, Ravaud A, Thezenas S, et al: Sunitinib alone or after nephrectomy in metastatic renal-cell carcinoma. : Sunitinib alone or after nephrectomy in metastatic renal-cell carcinoma.N Eng J Med. 379:417-427, 2018. doi: 10.1056/NEJMoa1803675
Prognosis for Renal Cancer
Five-year survival rates range from over 90% for localized disease to less than 20% for those with distant metastases (1). Prognosis is poor for patients with metastatic or recurrent renal cell carcinoma (RCC) because treatments are usually ineffective for cure, although they may be useful for palliation.
Prognosis reference
1. Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024 [published correction appears in CA Cancer J Clin. 2024 Mar-Apr;74(2):203. doi: 10.3322/caac.21830]. CA Cancer J Clin. 2024;74(1):12-49. doi:10.3322/caac.21820
Key Points
RCC, an adenocarcinoma, accounts for 90 to 95% of primary malignant renal tumors.
Symptoms (most often gross or microscopic hematuria) usually do not develop until the tumor is large or metastatic, so incidental discovery is common.
Diagnose RCC by MRI or contrast-enhanced CT and do a chest x-ray, blood tests (including liver tests) to investigate staging.
Treat most localized RCC by surgery, active surveillance or thermal ablation.
Treat advanced RCC with combination immunotherapy, targeted pharmacotherapy, interferon alfa-2b or IL-2, palliative radiation, and/or surgery.Treat advanced RCC with combination immunotherapy, targeted pharmacotherapy, interferon alfa-2b or IL-2, palliative radiation, and/or surgery.







