




AMD is the leading cause of permanent, irreversible vision loss in older adults. It is more common among White people (1).
General reference
1. Klein R, Chou CF, Klein BE, et al: Prevalence of age-related macular degeneration in the US population. Arch Ophthalmol 129(1):75-80, 2011. doi: 10.1001/archophthalmol.2010.318
Etiology of Age-Related Macular Degeneration
Risk factors include the following:
Age
Genetic variants (eg, abnormal complement factor H)
Family history
Smoking
Sun exposure
A diet low in omega-3 fatty acids and dark green leafy vegetables
Pathophysiology of Age-Related Macular Degeneration
Two different forms occur:
Dry (nonexudative or atrophic): All age-related macular degeneration (AMD) starts as the dry form. About 85% of people with AMD have only dry AMD (1).
Wet (exudative or neovascular): Wet AMD occurs in about 15% of people.

Image provided by Sunir Garg, MD.


Image provided by Sunir Garg, MD.
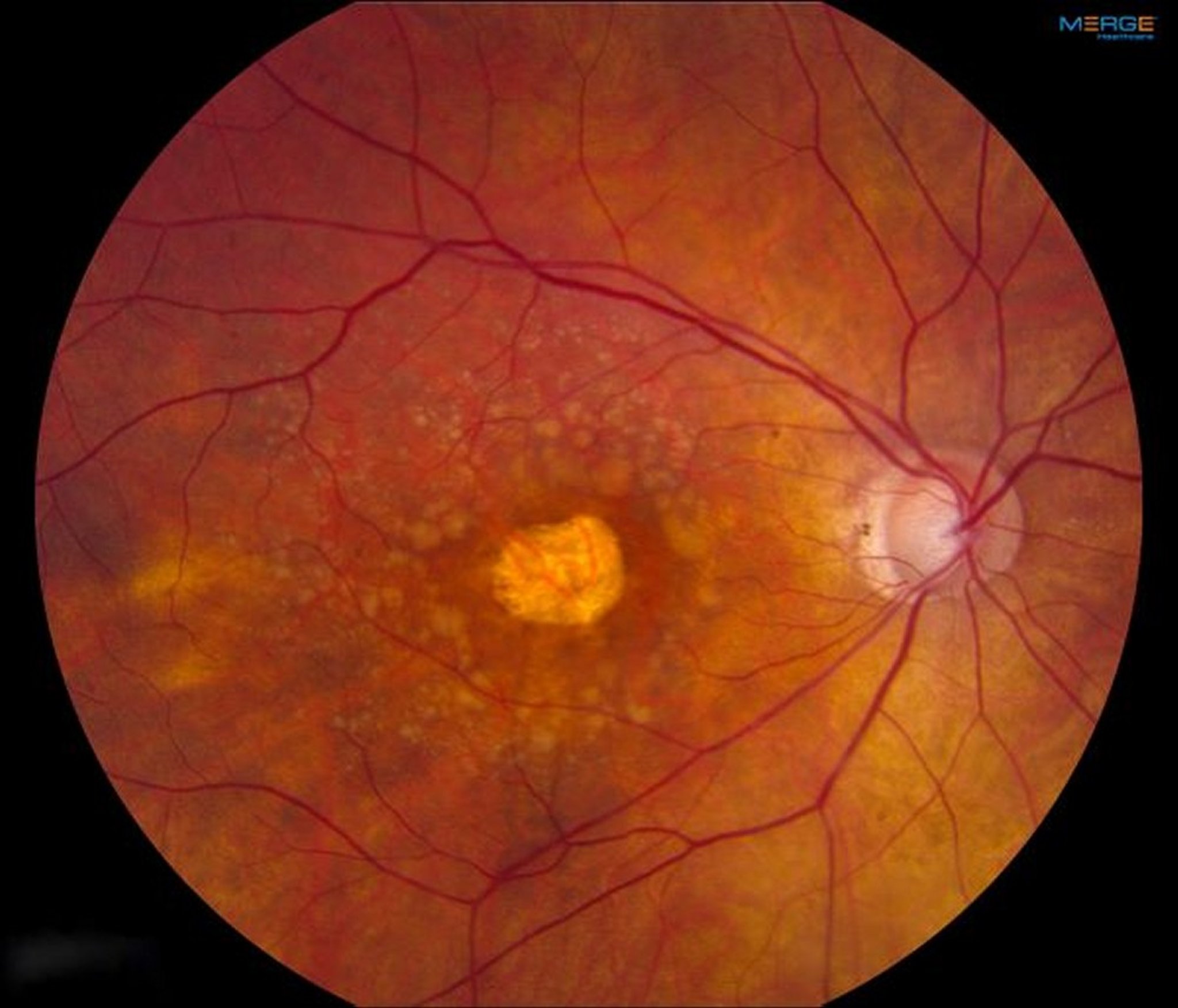
Image provided by Sunir Garg, MD.
Although only 15% of patients with AMD have the wet form, 80 to 90% of the severe vision loss caused by AMD results from wet AMD (1).

PAUL WHITTEN/SCIENCE PHOTO LIBRARY
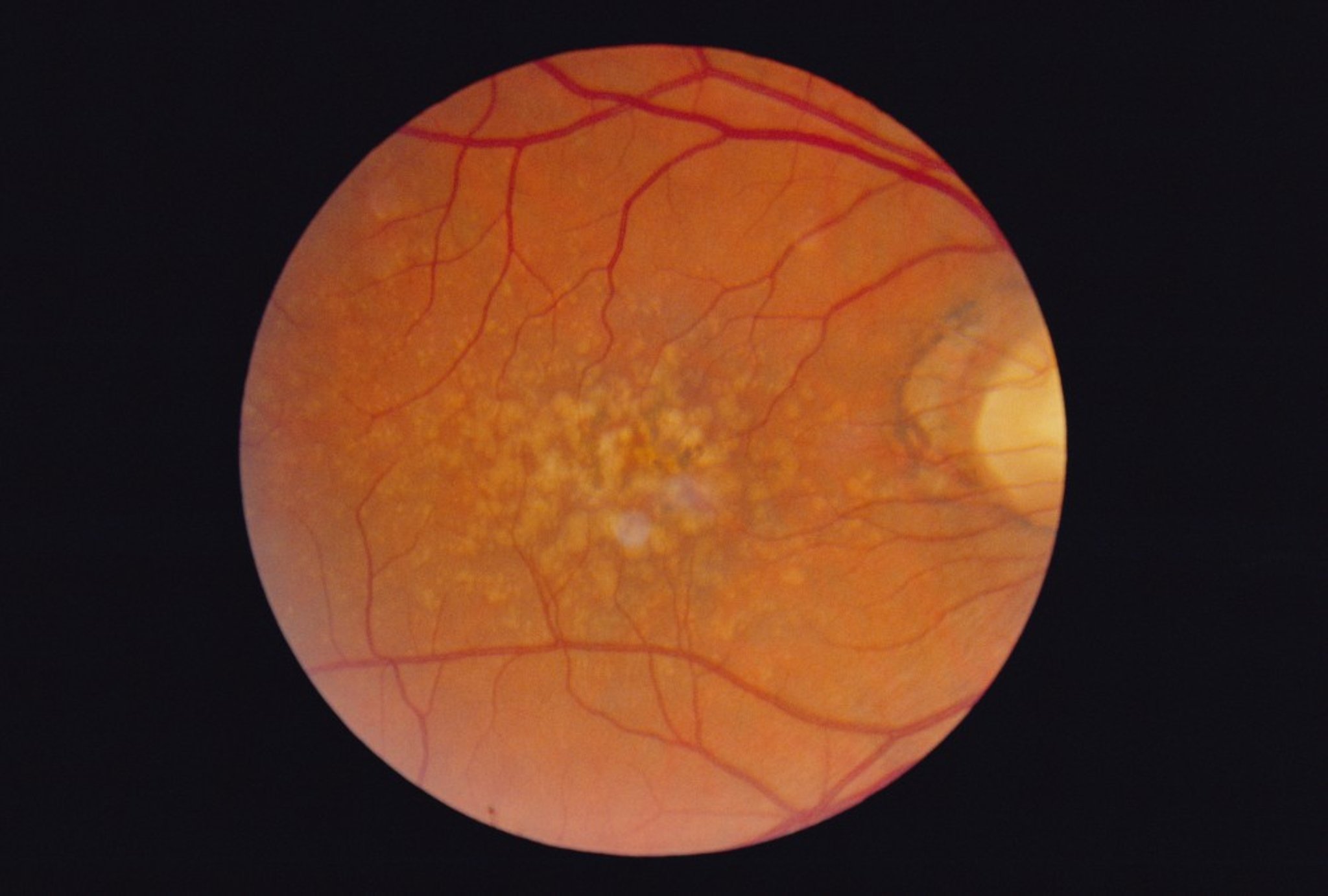
Dry AMD causes changes of the retinal pigment epithelium, typically visible as dark pinpoint areas. The retinal pigment epithelium plays a critical role in keeping the cones and rods healthy and functioning well. Accumulation of waste products from the rods and cones can result in drusen, which appear as yellow spots. Areas of chorioretinal atrophy (referred to as geographic atrophy) occur in more advanced cases of dry AMD. There is no elevated macular scar (disciform scar), edema, hemorrhage, or exudation.
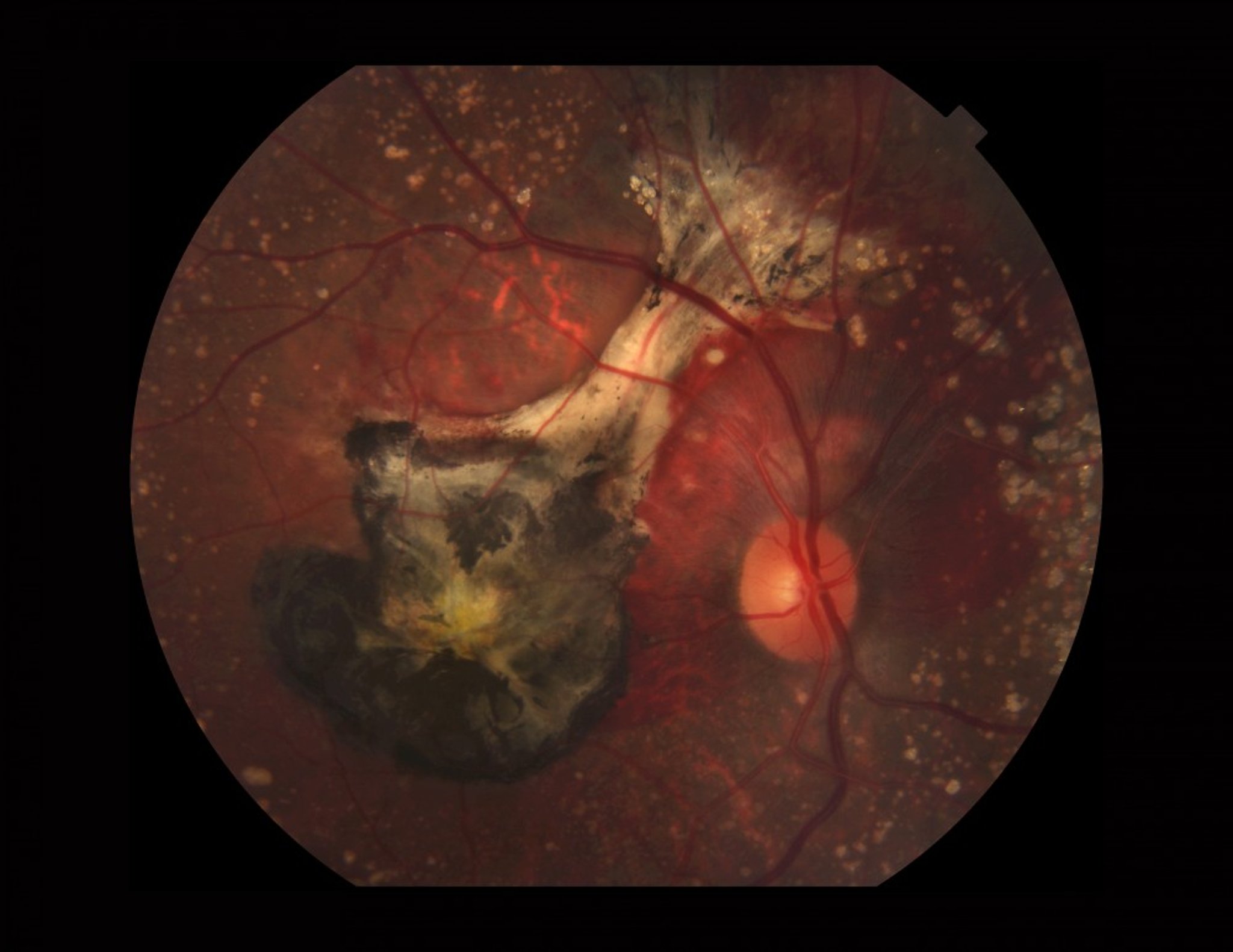
Wet AMD occurs when new abnormal blood vessels develop under the retina in a process called choroidal neovascularization (abnormal new vessel formation). Localized macular edema or hemorrhage may elevate an area of the macula or cause a localized retinal pigment epithelial detachment. Eventually, untreated neovascularization causes a disciform scar under the macula.
Pathophysiology reference
1. Ferris FL 3rd, Fine SL, Hyman L: Age-related macular degeneration and blindness due to neovascular maculopathy. Arch Ophthalmol 102(11):1640-1642, 1984. doi: 10.1001/archopht.1984.01040031330019
Symptoms and Signs of Age-Related Macular Degeneration
Dry AMD
The loss of central vision occurs over years and is painless, and most patients retain enough vision to read and drive. Central blind spots (scotomas) usually occur late in the disease and can sometimes become severe. Symptoms are usually bilateral.
Funduscopic changes include the following:
Changes in the retinal pigment epithelium
Drusen
Areas of chorioretinal atrophy
Wet AMD
Rapid vision loss, usually over days to weeks, is more typical of wet AMD. The first symptom is usually visual distortion, such as a central blind spot (scotoma) or curving of straight lines (metamorphopsia). Peripheral vision and color vision are generally unaffected; however, the patient may become legally blind (< 20/200 vision) in the affected eye, particularly if AMD is not treated. Wet AMD usually affects one eye at a time; thus, symptoms of wet AMD are often unilateral.
Funduscopic changes include the following:
Subretinal fluid, appearing as localized retinal elevation
Retinal edema
Gray-green discoloration under the macula
Exudates in or around the macula
Detachment of retinal pigment epithelium (visible as an area of retinal elevation)
Subretinal hemorrhage in or around the macula

PAUL PARKER/SCIENCE PHOTO LIBRARY
Diagnosis of Age-Related Macular Degeneration
Funduscopic examination
Color fundus photography
Optical coherence tomography
Both forms of age-related macular degeneration (AMD) are diagnosed by funduscopic examination. Visual changes can often be detected with an Amsler gridOptical coherence tomography (OCT) aids in identifying intraretinal and subretinal fluid and can help assess response to treatment.
Treatment of Age-Related Macular Degeneration
Dietary supplements for high-risk dry or unilateral wet age-related macular degeneration (AMD)
Intravitreal antivascular endothelial growth factor (anti-VEGF) medications or laser treatments for wet AMD
Supportive measures
In general, the management of dry AMD focuses on nutritional supplementation to slow disease progression, whereas wet AMD is also treated with intravitreal anti-VEGF or laser therapy.
Dry AMD
There is no way to reverse damage caused by dry AMD. Patients with extensive drusen, pigment changes, and/or geographic atrophy can reduce the risk of developing advanced AMD by 25% by taking daily supplements of the following:
Vitamin C 500 mg
In patients who currently or formerly smoked, beta-carotene can increase the risk of lung cancer. Substitution of beta-carotene with lutein plus zeaxanthin has been shown to have comparable efficacy (1). Therefore, such a substitution should be considered in patients who currently or formerly smoked. Beta-carotene yellows the skin in some patients. The zinc component of these supplements increases risk of hospitalization for genitourinary tract disorders. Reducing cardiovascular risk factors as well as regularly eating foods high in omega-3 fatty acids and dark green leafy vegetables may help slow disease progression (2); however, randomized trials have not shown that taking supplements of omega-3 fatty acids reduces disease progression (3).
4, 5). The primary outcome used in these studies was preservation of retinal tissue, not visual acuity outcomes (the outcome used in studies of wet AMD). These intravitreal medications can be administered every 1 to 2 months.
Wet AMD
6).
10); however, early reports (11) suggest a higher incidence of adverse events with this medication than with other intravitreal anti-VEGF injections, including intraocular inflammation, retinal artery occlusion, and vasculitis.
Treatment references
1. Age-Related Eye Disease Study 2 Research Group: Lutein + zeaxanthin and omega-3 fatty acids for age-related macular degeneration: The age-related eye disease study 2 (AREDS2) randomized clinical trial. JAMA 309(19):2005-2015, 2013. doi: 10.1001/jama.2013.4997. Clarification and additional information. JAMA 310(2):208, 2013. doi:10.1001/jama.2013.6403
2. Hogg RE, Woodside JV, McGrath A, et al: Mediterranean diet score and its association with age-related macular degeneration: The European Eye Study. Ophthalmology 124(1):82-89, 2017. doi: 10.1016/j.ophtha.2016.09.019
3. Christen WG, Cook NR, Manson JE, et alJAMA Ophthalmol 138(12):1280-1289, 2020. doi: 10.1001/jamaophthalmol.2020.4409
4. Heier JS, Lad EM, Holz FG, et al Lancet 402(10411):1434-1448, 2023. doi: 10.1016/S0140-6736(23)01520-9
5. Khanani AM, Patel SS, Staurenghi G, et alLancet 402(10411):1449-1458, 2023. doi: 10.1016/S0140-6736(23)01583-0
6. Finger RP, Puth MT, Schmid M, Barthelmes D, et al: Lifetime outcomes of anti-vascular endothelial growth factor treatment for neovascular age-related macular degeneration. JAMA Ophthalmol 138(12):1234-1240, 2020. doi: 10.1001/jamaophthalmol.2020.3989
7. Wykoff CC, Brown DM, Reed K, et alJAMA Ophthalmol 141(9):834–842, 2023. doi: 10.1001/jamaophthalmol.2023.2421
8. Heier JS, Khanani AM, Quezada Ruiz C, et alLancet 399(10326):729-740, 2022. doi: 10.1016/S0140-6736(22)00010-1
9. Holekamp NM, Campochiaro PA, Chang MA, all Archway InvestigatorsOphthalmology S0161-6420(21)00734-X, 2021
10. Dugel PU, Koh A, Ogura Y, HAWK and HARRIER Study InvestigatorsOphthalmology 127(1):72-84, 2020. doi: 10.1016/j.ophtha.2019.04.017
11. Haug SJ, Hien DL, Uludag G, et alAm J Ophthalmol Case Rep 18:100680, 2020. doi: 10.1016/j.ajoc.2020.100680
Supportive measures
For patients who have lost central vision, low-vision devices such as magnifiers, high-power reading glasses, large computer monitors, and telescopic lenses are available. Also, certain types of software can display computer data in large print or read information aloud in a synthetic voice. Low-vision counseling is advised.
Key Points
AMD is more common among White people and is the leading cause of permanent vision loss in older adults.
AMD can be dry (nonexudative or atrophic) or wet (exudative or neovascular).
Although 85% of AMD is dry, 80 to 90% of severe vision loss caused by AMD results from the wet type.
Funduscopic changes in dry AMD include drusen, areas of chorioretinal atrophy, and changes to the retinal pigment epithelium.
Funduscopic changes in wet AMD include retinal edema and localized elevation, detachment of the retinal pigment epithelium, a gray-green discoloration under the macula, and exudates in and around the macula.
Prescribe dietary supplements for unilateral wet or high-risk dry AMD.
Treat wet AMD with anti-VEGF medications as an intravitreal injection or through the port delivery system or with laser therapy.
Treat wet AMD with photodynamic therapy or laser therapy in select cases.






