


Cervical cancer is usually squamous cell carcinoma; adenocarcinoma is less common. The cause of most cervical cancers is human papillomavirus (HPV) infection. Cervical neoplasia is often asymptomatic; the first symptom of cervical cancer is usually irregular, often postcoital, vaginal bleeding. Diagnosis is by a cervical Papanicolaou test and biopsy. Staging is clinical, combined with imaging and pathology results when available. Treatment usually involves surgical resection for early-stage disease or chemoradiation therapy for locally advanced disease. If the cancer has widely metastasized, chemotherapy is often used alone or, sometimes, followed by pelvic radiation.
(See also Cervical Cancer Screening and Prevention.)
In the United States, cervical cancer is the 3rd most common gynecologic cancer and the 15th most common cancer among women (1) . Mean age at diagnosis is 50; it is frequently diagnosed in women aged 35 to 44 years. The National Cancer Institute estimates that in 2023, there will be 13,960 new cases of invasive cervical cancer and 4310 deaths (2). Worldwide, almost 85% of new cases and almost 90% of deaths from cervical cancer occur in low- and middle-resource countries. Cervical cancer is the most common cancer in 23 countries and the leading cause of cancer death in 36 countries (3, 4).
Risk factors associated with cervical cancer include
Cervical intraepithelial neoplasia
Increased potential exposure to sexually transmitted diseases (eg, early age at first sexual activity or first childbirth, multiple sex partners, high-risk sex partners)
History of vulvar or vaginal squamous intraepithelial neoplasia or cancer
Anal intraepithelial neoplasia or cancer
Oral contraceptive use
Cigarette smoking
Immunodeficiency
The precursor to cervical cancer is cervical intraepithelial neoplasia (CIN). The great majority of cases of CIN and invasive cervical cancer are caused by persistent infection with human papillomavirus (HPV), transmitted mainly through sexual activity. Most (70%) of precancerous and invasive disease can be directly attributed to HPV types 16 or 18; however, 99% of cervical cancer specimens contain DNA from one of more than 14 high-risk HPV genotypes (5, 6). The incidence of cervical cancer has decreased steadily over the past several decades because of HPV vaccination, cervical cancer screening, and treatment of CIN.
General references
1. National Cancer Institute's Surveillance, Epidemiology, and End Results (SEER) Program: Cancer Stat Facts: Common Cancer Sites. Table: How Do Cancer Rates Compare? National Cancer Institute. Bethesda, MD. Accessed July 14, 2023.
2. National Cancer Institute: Cancer Stat Facts: Cervical Cancer. Accessed July 14, 2023.
3. Sung H, Ferlay J, Siegel RL, et al: Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 71 (3):209–249, 2021. doi: 10.3322/caac.21660
4. Bhatla N, Aoki D, Sharma DN, Sankaranarayanan R: Cancer of the cervix uteri: 2021 update. Int J Gynaecol Obstet 155 Suppl 1(Suppl 1):28-44, 2021. doi:10.1002/ijgo.13865
5. Joste NE, Ronnett BM, Hunt WC, et al: Human papillomavirus genotype-specific prevalence across the continuum of cervical neoplasia and cancer. Cancer Epidemiol Biomarkers Prev 24 (1): 230–240, 2015. doi: 10.1158/1055-9965.EPI-14-0775
6. Walboomers JMM, Jacobs MV, Manos MM, et al: Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. J Pathol 189 (1):12–19, 1999. doi: 10.1002/(SICI)1096-9896(199909)189:1<12::AID-PATH431>3.0.CO;2-F
Pathology of Cervical Cancer
The cervix is composed of stroma and epithelium. The ectocervix protrudes into the vagina and is lined with squamous epithelium. The endocervix (a canal that passes from the internal os to the external os) is lined with columnar epithelium. Nearly all cervical carcinomas originate in the transformation zone, which surrounds the external os; the transformation zone is an area of squamous metaplasia between the original and current squamocolumnar junction (1).
Cervical intraepithelial neoplasia (CIN) is graded as
1: Mild cervical dysplasia
2: Moderate dysplasia
3: Severe dysplasia and carcinoma in situ
CIN3 is unlikely to regress spontaneously; if untreated, it may, over months or years, penetrate the basement membrane, becoming invasive carcinoma.
About 80 to 85% of all cervical cancers are squamous cell carcinoma; most of the rest are adenocarcinomas. Sarcomas and small cell neuroendocrine tumors are rare.
Invasive cervical cancer usually spreads by direct extension into surrounding tissues or via the lymphatics to the pelvic and para-aortic lymph nodes. Hematogenous spread is possible but rare.
If cervical cancer spreads to the pelvic or para-aortic lymph nodes, the prognosis is worse, and the location and size of the radiation therapy field is affected.
Pathology reference
1. Bhatla N, Aoki D, Sharma DN, et al: Cancer of the cervix uteri: 2021 update. Int J Gynaecol Obstet 155 Suppl 1:28-44, 2021. doi: 10.1002/ijgo.13865
Symptoms and Signs of Cervical Cancer
Early cervical cancer is often asymptomatic. When symptoms occur, they usually include irregular vaginal bleeding, which is most often postcoital, but may occur spontaneously between menses. Larger cancers are more likely to bleed spontaneously and may cause a foul-smelling vaginal discharge or pelvic pain. More widespread cancer may cause obstructive uropathy, back pain, and leg swelling due to venous or lymphatic obstruction.
Diagnosis of Cervical Cancer
Papanicolaou (Pap) test (cervical cytology)
Biopsy
Cervical cancer may be suspected during a routine gynecologic examination. Further evaluation is required for patients with
A visible cervical lesion
Abnormal vaginal bleeding
Cervical cancer is usually diagnosed when cervical cytology and/or HPV testing detects abnormalities. Findings are usually microscopic, but in some cases there is a cervical lesion. A large tumor may be exophytic and necrotic, but a lesion may also be smaller and less distinctive. Biopsy should be performed for any cervical lesion for which there is a suspicion of malignancy.
Reporting of cervical cytology results is standardized (see table Bethesda Classification of Cervical Cytology [1]). Further evaluation with cytology, HPV testing, or colposcopy is indicated if atypical or cancerous cells are found and/or HPV testing is positive. Colposcopy (examination of the vagina and cervix with a magnifying lens) is used to identify areas that require biopsy; endocervical curettage is also often performed.
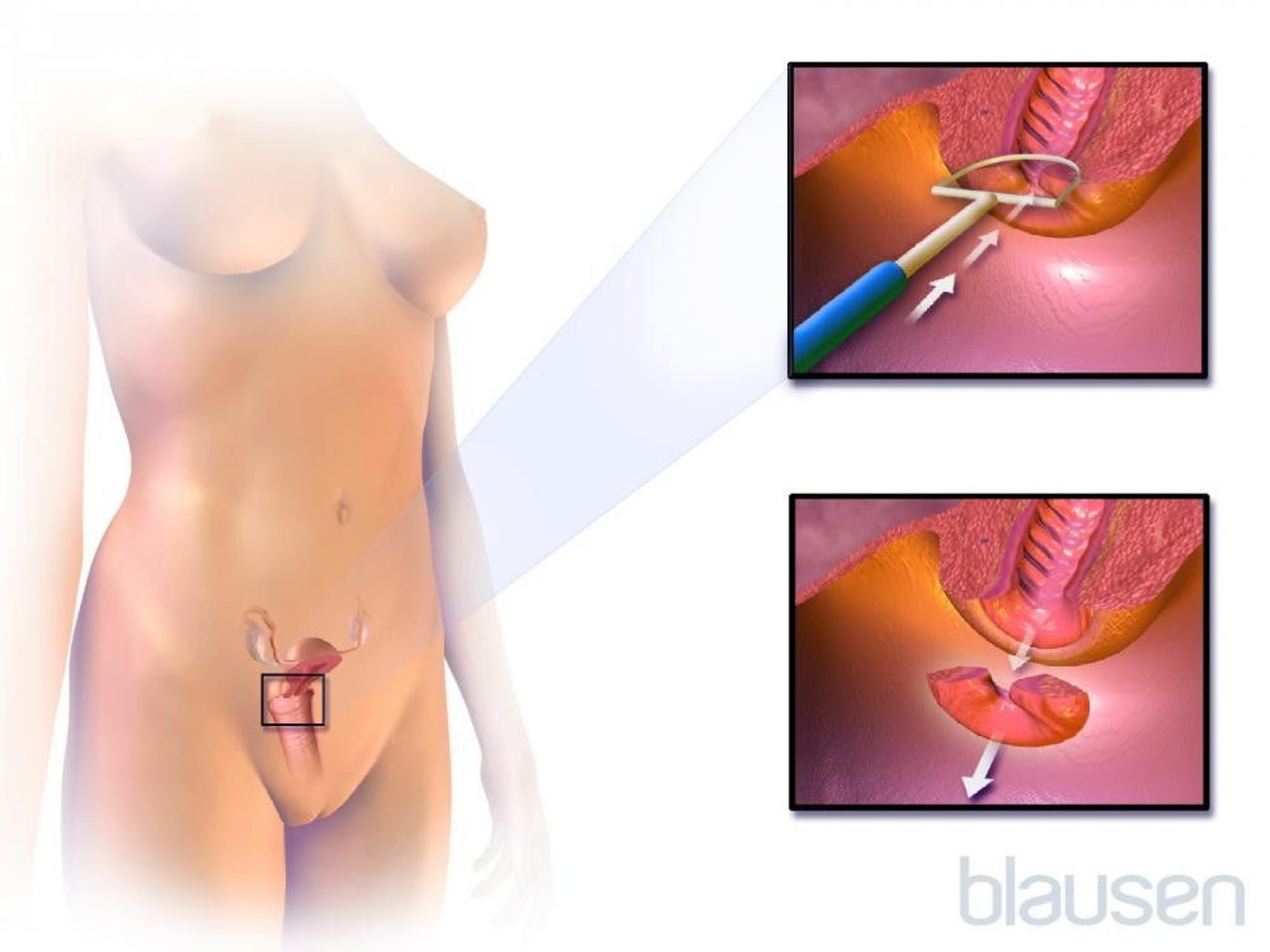
Cone biopsy (conization) is required if the diagnosis is uncertain and high-grade CIN or invasive cancer is suspected; a cone of tissue is removed using a loop electrical excision procedure (LEEP), laser, or scalpel (cold knife).

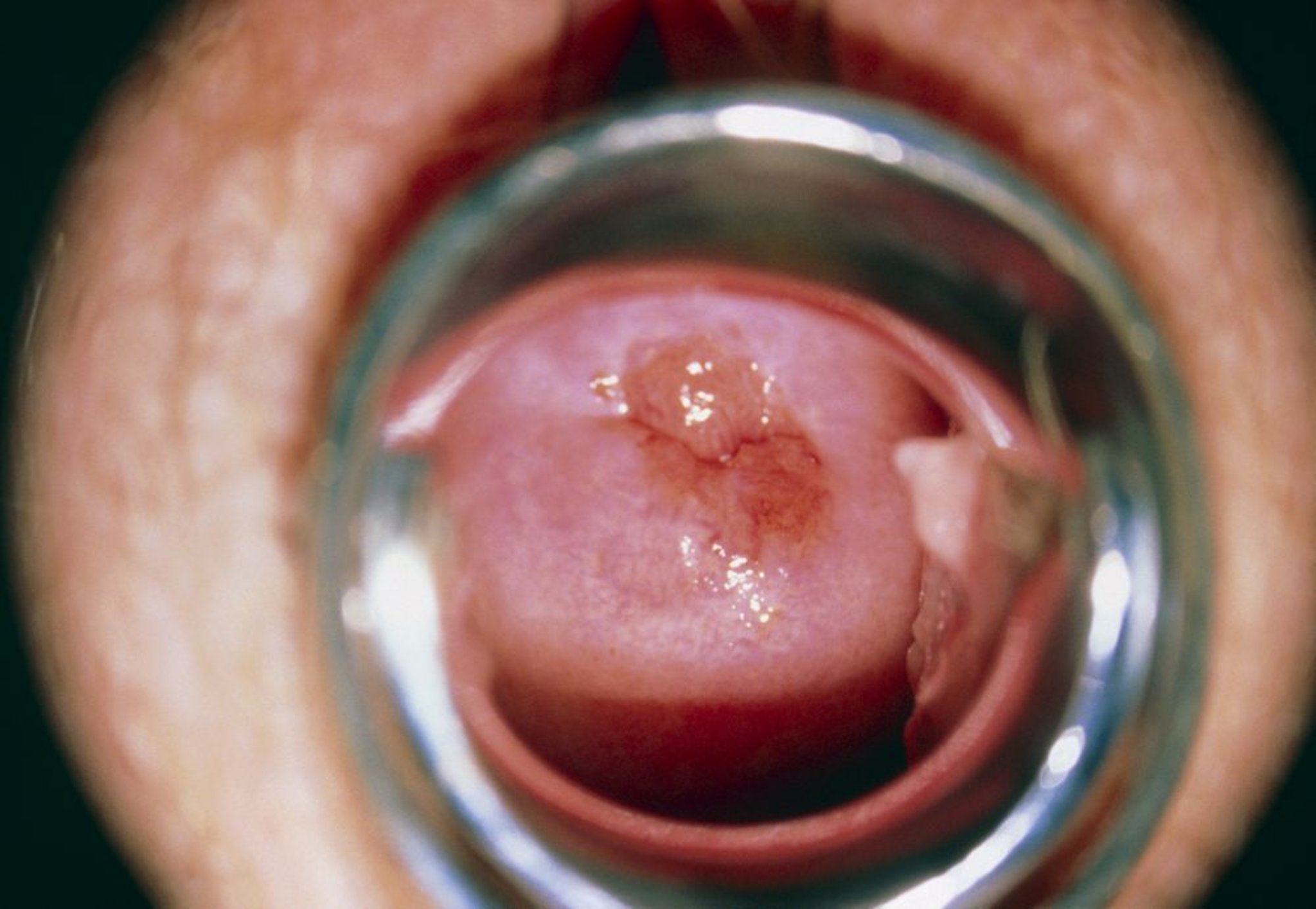
SCIENCE PHOTO LIBRARY

Staging
Cervical cancer staging underwent a major revision in 2018. The previous International Federation of Obstetrics and Gynecology (Federation Internationale de Gynecologie et d'Obstetrique, or FIGO) 2009 staging system allowed only clinical examination, cervical biopsy, and a few additional tests to assign the stage. The FIGO 2018 staging system allows, when available, cross-sectional imaging (eg, ultrasonography, CT, MRI, positron emission tomography [PET], PET-CT, MRI-PET), and surgical pathology results to supplement clinical findings in all stages. Imaging and pathology results are optional because they may be not available in low- and middle-resource countries, where cervical cancer is more common (2, 3, 4).
Other changes in the 2018 staging system include the following:
Horizontal spread of the tumor is no longer considered part of stage IA1 and IA2.
Stage I is subdivided into 3 subgroups according to tumor size (IB1 ≤ 2 cm, IB2> 2 to ≤ 4 cm, and IB3 > 4 cm) instead of 2 subgroups (stages IB1 and IB2, which used only 4 cm as a cutoff value).
Lymph node status is now part of the staging system. Positive pelvic nodes are now stage IIIC1 and positive paraortic nodes are stage IIIC2. Micrometastases in the lymph nodes are considered positive; however, these isolated tumor cells do not change the stage to III, but they should be recorded. If lymph nodes are classified as positive by imaging studies, an "r" is added to the stage (eg, IIIC1r, IIIC2r); if they are classified as positive by pathology results, a "p" is added(IIIC1p, IIIC2p [2, 3, 4]).
If the stage is higher than A2, CT or MRI of the abdomen and pelvis is typically done to better determine tumor size, parametrial involvement, vaginal compromise, and nodal metastases. PET with CT (PET/CT) is often used to check for spread beyond the cervix. If PET/CT, MRI, or CT is not available, cystoscopy, sigmoidoscopy, chest x-ray, and IV urography, when clinically indicated, may be used for staging.
When imaging tests suggest that pelvic or para-aortic lymph nodes are grossly enlarged (> 2 cm), surgical exploration, typically with a retroperitoneal approach, may be indicated. Its sole purpose is to remove enlarged lymph nodes so that radiation therapy can be more precisely targeted and more effective.
Diagnosis references
1. Nayar R, Wilbur DC: The Pap test and Bethesda 2014. Cancer Cytopathology, 123: 271–281, 2015. doi:10.1002/cncy.21521
2. Bhatla N, Berek JS, Cuello Fredes M, et al: Revised FIGO Staging for Carcinoma of the Cervix Uteri. Int J Gynaecol Obstet 145 (1):129–135, 2019. doi: 10.1002/ijgo.12749
3. Bhatla N, Berek JS, Cuello Fredes M, et al: Corrigendum to “Revised FIGO staging for carcinoma of the cervix uteri” [Int J Gynecol Obstet 145(2019) 129–135]. Int J Gynaecol Obstet 147(2):279-280, 2019. doi: 10.1002/ijgo.12969
4. Bhatla N, Aoki D, Sharma DN, Sankaranarayanan R: Cancer of the cervix uteri: 2021 update. Int J Gynaecol Obstet 155 Suppl 1(Suppl 1):28-44, 2021. doi:10.1002/ijgo.13865
Treatment of Cervical Cancer
Surgery alone for microinvasive disease
Surgery or curative radiation therapy if there is no spread to parametria or beyond
Radiation therapy and chemotherapy (chemoradiation) if there is spread to parametria or beyond
Chemotherapy for metastatic and recurrent cancer
Treatment of cervical cancer may include surgery, radiation therapy, and chemotherapy. If radical hysterectomy is indicated but patients are not ideal candidates for it, chemoradiation is used and has similar oncologic outcomes.
Stage IA1 (no lymphovascular space invasion)
Treatment of stage IA1 involves
Conization or simple hysterectomy
Microinvasive cervical cancer, defined as FIGO stage IA1 with no lymphovascular space invasion (LVSI), has a < 1% risk of lymph node metastases and may be managed conservatively with conization using loop electrosurgical excision procedure (LEEP), laser, or cold knife. Conization is indicated for patients who are interested in preserving fertility (to obtain, if possible, a nonfragmented specimen with a 3-mm margin). A cold knife preserves the margins for pathology evaluation but cannot always be used.
Simple hysterectomy should be done if patients are not interested in preserving fertility or if margins are positive after conization. If margins are positive, sentinel lymph node (SLN) mapping should be considered, and if patients are interested in preserving fertility, repeat conization is an alternative.
Sentinel lymph node mapping for cervical cancer
Sentinel lymph node (SLN) mapping is an alternative to full pelvic lymphadenectomy for patients with early-stage (IA1 with lymphovascular space invasion, IB1, IB2, or IIA1) cervical cancer (1) because only 15 to 20% of these patients have positive nodes. SLN mapping therefore decreases the number of full pelvic lymphadenectomies, which can have adverse effects (eg, lymphedema, nerve damage).
Ultrastaging of all SLNs is done to detect micrometastasis and isolated tumor cells (low-volume disease). Any grossly suspicious node must be removed regardless of mapping. If there is no mapping on a hemipelvis, a side-specific lymphadenectomy is done. In the 2018 FIGO staging system, only macrometastases and micrometastases are considered when classifying cases as IIIC; isolated tumor cells do not change the stage, they are considered pN0.
Detection rates for SLN mapping are best for tumors < 2 cm.
Stage IA1 (with lymphovascular space invasion) and stage IA2
For stage IA1 with LVSI or stage IA2, recommended treatments include
Modified radical hysterectomy and pelvic lymphadenectomy (with or without SLN mapping)
External pelvic radiation therapy with brachytherapy
Criteria for radiation therapy after radical hysterectomy
Criteria used to determine whether pelvic radiation with concurrent chemotherapy should be done after radical hysterectomy include the following (see table Sedlis Criteria for External Pelvic Radiation After Radical Hysterectomy):
Presence of lymphovascular space invasion
Depth of invasion
Tumor size
Patients with a combination of risk factors, such as large tumor size (> 4 cm), deep (> 1/3) stromal invasion, and/or lymphovascular space invasion (LVSI), have a risk of recurrence and death of up to 30% after surgery alone (2, 3).
Risk factors such as positive margins and/or pathologically confirmed positive pelvic lymph nodes and/or microscopic involvement of the parametrium are considered higher risk. In a randomized trial, the estimated 4-year survival rates for patients with stage IB cervical cancer and high-risk factors were 81% for those treated with combined chemotherapy and radiation therapy and 71% for those treated with radiation therapy alone (4, 5).
Stages IB1, IB2, and IIA1
For stages IB1, IB2, and IIA1, the standard recommendation is
Open radical hysterectomy with bilateral pelvic lymphadenectomy (with or without SLN mapping)
Radical hysterectomy includes resection of the uterus (including the cervix), parts of the cardinal and uterosacral ligaments, the upper 1 to 2 cm of the vagina, the pelvic lymph nodes and parametrium. The Querleu & Morrow classification system describes four types of radical hysterectomy based on the lateral extent of resection; a few subtypes take nerve preservation and paracervical lymphadenectomy into account (6).
Results from a randomized trial showed that minimally invasive surgery (laparoscopy or robot-assisted laparoscopy) resulted in a lower overall survival rate and a higher recurrence rate than total abdominal radical hysterectomy (7). Therefore, open radical hysterectomy is recommended as the appropriate approach.
When patients are not considered ideal candidates for surgery because of comorbidities, another valid option is external pelvic radiation therapy and brachytherapy with or without concurrent platinum-based chemotherapy.
Another treatment option is radical hysterectomy and bilateral pelvic lymphadenectomy (with or without para-aortic lymphadenectomy), sometimes with adjuvant radiation therapy (see table Sedlis Criteria for External Pelvic Radiation After Radical Hysterectomy).
If extracervical spread is noted during radical hysterectomy, the procedure should be aborted, and postoperative radiation therapy with concurrent chemotherapy is recommended to prevent local recurrence (8).
Stages IB3, IIA2, IIB, III, and IVA
The standard therapy for stages IB3, IIA2, IIB, III, and IVA cancer is
External pelvic radiation therapy with brachytherapy and concurrent platinum-based chemotherapy
To determine the extent of the radiation field, clinicians may evaluate spread to para-aortic lymph nodes clinically (abdominal CT and/or MRI) or surgically (pelvic and para-aortic lymphadenectomy). In a randomized trial, oncologic outcomes did not differ significantly in patients with stage IIB through IVA staged clinically compared with those staged surgically before chemoradiation. In this study, laparoscopic staging appeared to be safe, did not delay primary treatment, and resulted in upstaging in 33% of patients with locally advanced cervical cancer (9).
When cancer is limited to the cervix and/or pelvic lymph nodes, the standard recommendation is
External beam radiation therapy, followed by brachytherapy (local radioactive implants, usually using cesium) to the cervix
Radiation therapy may cause acute complications (eg, radiation proctitis and cystitis) and, occasionally, late complications (eg, vaginal stenosis, intestinal obstruction, rectovaginal and vesicovaginal fistula formation).
Although stage IVA cancers are usually treated with radiation therapy initially, pelvic exenteration (excision of all pelvic organs) may be considered. If after radiation therapy, cancer remains but is confined to the central pelvis, exenteration is indicated and cures up to 40% of patients. The procedure may include continent or incontinent urostomy, low anterior rectal anastomosis without colostomy or with an end-descending colostomy, omental carpet to close the pelvic floor (J-flap), and vaginal reconstruction with gracilis or rectus abdominis myocutaneous flaps.
Stage IVB and recurrent cancer
Chemotherapy is the primary treatment for stage IVB cervical cancer. Response rates are approximately 38% (10).
11).
Metastases outside the radiation field appear to respond better to chemotherapy than does previously irradiated cancer or metastases in the pelvis.
A systematic review of observational studies included 2424 patients with stage IVB squamous cell, adenocarcinoma, or adenosquamous carcinoma of the cervix and found improved overall survival associated with definitive (≥ 45 Gy) pelvic radiotherapy compared with systemic chemotherapy (with or without palliative pelvic radiation) (12).
Clinicians should consider testing for mismatch repair (MMR) and microsatellite instability (MSI), PD-L1 (programmed cell death-ligand 1) expression, and/or NTRK gene fusion if patients have recurrent, progressive, or metastatic cervical cancer. Results can help predict responses to immunotherapies such as PD-L1 inhibitors.
Few effective second-line treatments exist for women with recurrent or metastatic cervical cancer.
13).
14).
Fertility-sparing surgery
Fertility-sparing surgery is an option in some patients who have early-stage cervical cancer (IA1 with LVSI, IA2, IB1, some cases of IB2) and who wish to preserve fertility.
Surgical treatment of cervical cancer does not include oophorectomy unless ovaries appear abnormal. In young patients having surgery, ovarian preservation is particular important to avoid premature menopause. Before pelvic radiation, ovaries may be moved outside the radiation field (oophoropexy) to avoid toxic exposure. Patients should be counseled about the benefit of preserving ovary function versus the risk of potential ovarian metastases. In a study of 3471 patients who had stage Ib through IIb cervical cancer treated with a radical hysterectomy, the cancer metastasized to the ovaries in 1.5% of patients (15). Ovarian metastasis was more common among patients with adenocarcinoma (5.31%) than among those with squamous cell carcinoma (0.79%).
Surgical options for uterine conservation include
Radical trachelectomy with nodal evaluation
Cervical conization
Radical trachelectomy is removal of the cervix, parametria immediately adjacent to the cervix, upper 2 cm of the vagina, and pelvic lymph nodes. The uterus is conserved and is reattached to the upper vagina, preserving the potential for fertility. Candidates for this procedure are patients with the following:
Histologic subtypes such as squamous cell carcinoma, adenocarcinoma, or adenosquamous carcinoma (not neuroendocrine or small cell carcinoma or sarcoma)
Stage IA1/grade 2 or 3 with lymphovascular space invasion
Stage IA2
Stage IB1
Invasion of the upper cervix and lower uterine segment should be excluded by MRI before surgery. Rates of recurrence and death are similar to those after radical hysterectomy. If patients who have this procedure plan to have children, delivery must be cesarean. After a radical trachelectomy, fertility rates range from 50 to 70%, and the recurrence rate is about 5 to 10%.
Radical trachelectomy can be performed via vaginal surgery, laparotomy, laparoscopy, or robotic-assisted surgery. There has been concern about the safety of radical trachelectomy using minimally invasive approaches (laparoscopy or robotic-assisted surgery) compared with laparotomy. In one retrospective study of patients with early-stage cervical cancer (≤ 2 cm), laparotomy compared with minimally invasive approaches had comparable 4.5-year disease-free survival rates (16).
For patients with low-risk, early-stage cervical cancer, conization with pelvic nodal evaluation may be an alternative to radical trachelectomy. In a single-arm, prospective study, conservative surgery (cervical conization or simple hysterectomy with nodal evaluation) appeared to be safe and feasible in women with low-risk, early-stage cervical cancer; the 2-year recurrence rate was 3.5% (17). Studies to determine the optimal treatment for patients with early-stage cervical cancer are ongoing (eg, SHAPE trial) (18).
An ongoing prospective study (CONTESSA) is evaluating the role of neoadjuvant chemotherapy followed by fertility-sparing surgery in patients who have tumors 2 to 4 cm and who wish to preserve fertility (19).
Treatment references
1. National Comprehensive Cancer Network (NCCN): NCCN Clinical Practice Guidelines in Oncology: Cervical Cancer. Version 1.2023. October 26, 2021. Accessed July 14, 2023.
2. Sedlis A, Bundy BN, Rotman MZ, et al: A randomized trial of pelvic radiation therapy versus no further therapy in selected patients with stage IB carcinoma of the cervix after radical hysterectomy and pelvic lymphadenectomy: A Gynecologic Oncology Group Study. Gynecol Oncol 73 (2):177–183, 1999. doi: 10.1006/gyno.1999.5387
3. Rotman M, Sedlis A, Piedmonte MR, et al: A phase III randomized trial of postoperative pelvic irradiation in stage IB cervical carcinoma with poor prognostic features: Follow-up of a Gynecologic Oncology Group Study. Int J Radiat Oncol Biol Phys 65 (1):169–176, 2006. doi: 10.1016/j.ijrobp.2005.10.019
4. Peters WA, Liu PY, Barrett RJ, et al: Concurrent chemotherapy and pelvic radiation therapy compared with pelvic radiation therapy alone as adjuvant therapy after radical surgery in high-risk early-stage cancer of the cervix. J Clin Oncol 18 (8):1606–1613, 2000. doi: 10.1200/JCO.2000.18.8.1606
5. Monk BJ, Wang J, Im S, et al: Rethinking the use of radiation and chemotherapy after radical hysterectomy: a clinical-pathologic analysis of a Gynecologic Oncology Group/Southwest Oncology Group/Radiation Therapy Oncology Group trial. Gynecol Oncol 96 (3):721–728, 2005. doi: 10.1016/j.ygyno.2004.11.007
6. Querleu D, Morrow CP: Classification of radical hysterectomy. Lancet Oncol 9 (3):297–303, 2008. doi: 10.1016/S1470-2045(08)70074-3
7. Ramirez PT, Frumovitz M, Pareja R, et al: Minimally invasive versus abdominal radical hysterectomy for cervical cancer. N Engl J Med 379 (20): 1895–1904, 2018. doi: 10.1056/NEJMoa1806395
8. Cibula D, Dostalek L, Hillemanns P, et al: Completion of radical hysterectomy does not improve survival of patients with cervical cancer and intraoperatively detected lymph node involvement: ABRAX international retrospective cohort study. Eur J Cancer 143:88–100, 2021. doi: 10.1016/j.ejca.2020.10.037
9. Marnitz S, Tsunoda AT, Martus P, et al: Surgical versus clinical staging prior to primary chemoradiation in patients with cervical cancer FIGO stages IIB–IVA: Oncologic results of a prospective randomized international multicenter (Uterus-11) intergroup study. Int J Gynecol Cancer 30:1855–1861, 2020. doi:10.1136/ijgc-2020-001973
10. Ruengkhachorn I, Leelaphatanadit C, Therasakvichya S, et al: Oncologic outcomes of stage IVB or persistent or recurrent cervical carcinoma patients treated with chemotherapy at Siriraj Hospital: Thailand's largest tertiary referral center. Int J Gynecol Cancer 26(6):1154-1161, 2016. doi:10.1097/IGC.0000000000000712
11. Tewari KS, Sill MW, Long HJ IIIN Engl J Med 370 (8):734-743, 2014. doi: 10.1056/NEJMoa1309748
12. Viveros-Carreño D, Vieira-Serna S, Grillo-Ardila CF, et al: Definitive pelvic radiotherapy for patients with newly diagnosed stage IVB cervical cancer: a systematic review. Int J Gynecol Cancer 33(7):1057-1062, 2023. Published 2023 Jul 3. doi:10.1136/ijgc-2023-004465
13. Colombo N, Dubot C, Lorusso D, et al: Pembrolizumab for persistent, recurrent, or metastatic cervical cancer. N Engl J Med 385 (20):1856–1867, 2021. doi: 10.1056/NEJMoa2112435
14. Coleman RL, Lorusso D, Gennigens C, et alLancet Oncol 22(5):609-619, 2021. doi:10.1016/S1470-2045(21)00056-5
15. Shimada M, Kigawa J, Nishimura R, Yamaguchi S, et al: Ovarian metastasis in carcinoma of the uterine cervix. Gynecol Oncol 101 (2):234–237, 2006. doi: 10.1016/j.ygyno.2005.10.004
16. Salvo G, Ramirez PT, Leitao M, et al: Open vs minimally invasive radical trachelectomy in early-stage cervical cancer: International Radical Trachelectomy Assessment Study. Am J Obstet Gynecol 226 (1):97.e1-97.e16, 2022. doi: 10.1016/j.ajog.2021.08.029
17. Schmeler KM, Pareja R, Aldo Lopez Blanco AL, et al: ConCerv: A prospective trial of conservative surgery for low-risk early-stage cervical cancer. Int J Gynecol Cancer 31 (10):1317–1325, 2021. doi: 10.1136/ijgc-2021-002921
18. Plante M, Kwon JS, Ferguson et al: An international randomized phase III trial comparing radical hysterectomy and pelvic node dissection (RH) vs simple hysterectomy and pelvic node dissection (SH) in patients with low-risk early-stage cervical cancer (LRESCC): A Gynecologic Cancer Intergroup study led by the Canadian Cancer Trials Group (CCTG CX.5-SHAPE). [abstract taken from J Clin Oncol 41(suppl 17; abstract LBA5511), 2023. doi: 10.1200/JCO.2023.41.17_suppl.LBA5511
19. Plante M, van Trommel NE, Schaafsma M, et al: 2022-RA-678-ESGO CONTESSA/NEOCON-F trial: Assessing the effectiveness and safety of neoadjuvant chemotherapy followed by fertility-sparing surgery in FIGO 2018 stage IB2 cervical cancer. International Journal of Gynecologic Cancer 32:A20, 2022. http://dx.doi.org/10.1136/ijgc-2022-ESGO.45
Prognosis for Cervical Cancer
The most common histologic types of cervical cancer (squamous cell carcinoma, adenocarcinoma) usually metastasize to distant sites only when the cancer is locally advanced or recurrent. The 5-year survival rates are as follows:
Stage I: 80 to 90%
Stage II: 60 to 75%
Stage III: 30 to 40%
Stage IV: 0 to 15%
Nearly 80% of recurrences manifest within 2 years.
Adverse prognostic factors include
Lymph node involvement
Large tumor size and volume
Deep cervical stromal invasion
Parametrial invasion
Lymphovascular space invasion (LVSI)
Nonsquamous histology
Key Points
Consider cervical cancer if women have abnormal cervical cancer screening (HPV or Pap test) results, visible cervical lesions, or abnormal, particularly postcoital, vaginal bleeding.
Do a colposcopy and/or biopsy to further evaluate and confirm the diagnosis.
Stage cervical cancer clinically, using biopsy, pelvic examination, and available imaging, including chest x-ray; also use ultrasonography, PET/CT, MRI, or CT and surgical pathology, if available.
Treatment is surgical resection for early-stage cancer, radiation therapy plus chemotherapy for locally advanced cancer, and chemotherapy for metastatic and recurrent cancer.
Recommend HPV vaccination for children, before first sexual activity.
More Information
The following English-language resource may be useful. Please note that THE MANUAL is not responsible for the content of this resource.
National Cancer Institute: Cervical Cancer Treatment: This web site provides general information about cervical cancer and information about classification, staging, treatment by stage, and cervical cancer during pregnancy.






