




(See also Overview of Sexually Transmitted Infections.)
Several organisms can cause nongonococcal sexually transmitted cervicitis in women and urethritis, proctitis, and pharyngitis in both sexes. These organisms include
Chlamydia trachomatis (causes lymphogranuloma venereum [rare], about 50% of nongonococcal urethritis cases, and most cases of mucopurulent cervicitis)
Mycoplasma genitalium and M. hominis (which causes urogenital infections in women but not men)
Trichomonas vaginalis (trichomoniasis)
The imprecise term "nonspecific urethritis” can be used, but only if tests for chlamydiae and gonococci are negative and no other pathogen is identified.
Chlamydiae and mycoplasmas also cause infections that are not sexually transmitted, including trachoma and neonatal conjunctivitis (chlamydiae) and pneumonia (chlamydiae and mycoplasmas).
Symptoms and Signs of Chlamydia
Men develop symptomatic urethritis after a 7- to 28-day incubation period, usually beginning with mild dysuria, discomfort in the urethra, and a clear to mucopurulent discharge. Discharge may be slight, and symptoms may be mild but are frequently more marked early in the morning; then, the urethral meatus is often red and blocked with dried secretions, which may also stain underclothes. Occasionally, onset is more acute and severe, with severe dysuria, frequency, and a copious, purulent discharge that simulates gonococcal urethritis. Infection may progress to epididymitis. After rectal or orogenital contact with an infected person, proctitis or pharyngitis may develop.
Women are usually asymptomatic, although vaginal discharge, dysuria, increased urinary frequency and urgency, pelvic pain, dyspareunia, and symptoms of urethritis may occur. Cervicitis with yellow, mucopurulent exudate and cervical ectopy (expansion of the red endocervical epithelium onto the vaginal surfaces of the cervix) are characteristic. Pelvic inflammatory disease (PID; salpingitis and pelvic peritonitis) may cause lower abdominal discomfort (typically bilateral) and marked tenderness when the abdomen, adnexa, and cervix are palpated. Long-term consequences of PID include ectopic pregnancy and infertility. Fitz-Hugh-Curtis syndrome (perihepatitis) may cause right upper quadrant pain, fever, and vomiting.
Chlamydiae may be transferred to the eye, causing acute conjunctivitis.
Reactive arthritis caused by immunologic reactions to genital and intestinal infections is an infrequent complication of chlamydial infections in adults. Reactive arthritis sometimes is accompanied by skin lesions (keratoderma blennorrhagicum), eye lesions (conjunctivitis and uveitis), noninfectious recurrent urethritis, or balanitis.

Image courtesy of Susan Lindsley via the Public Health Image Library of the Centers for Disease Control and Prevention.

Image courtesy of Joe Miller via the Public Health Image Library of the Centers for Disease Control and Prevention.

Image courtesy of Drs. Weisner and Kaufman via the Public Health Image Library of the Centers for Disease Control and Prevention.

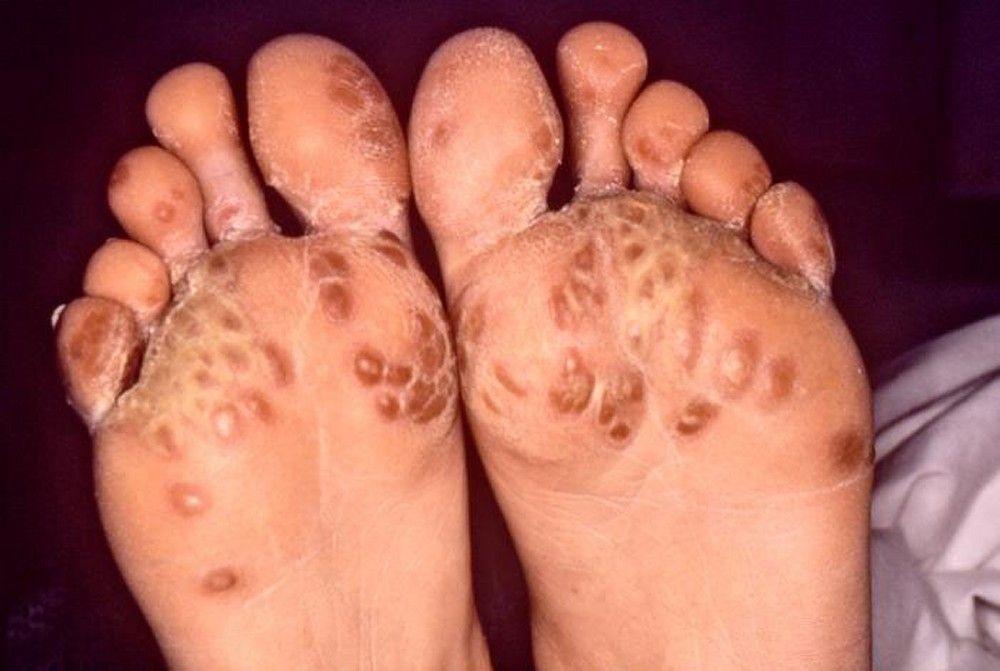
Image courtesy of Susan Lindsley via the Public Health Image Library of the Centers for Disease Control and Prevention.

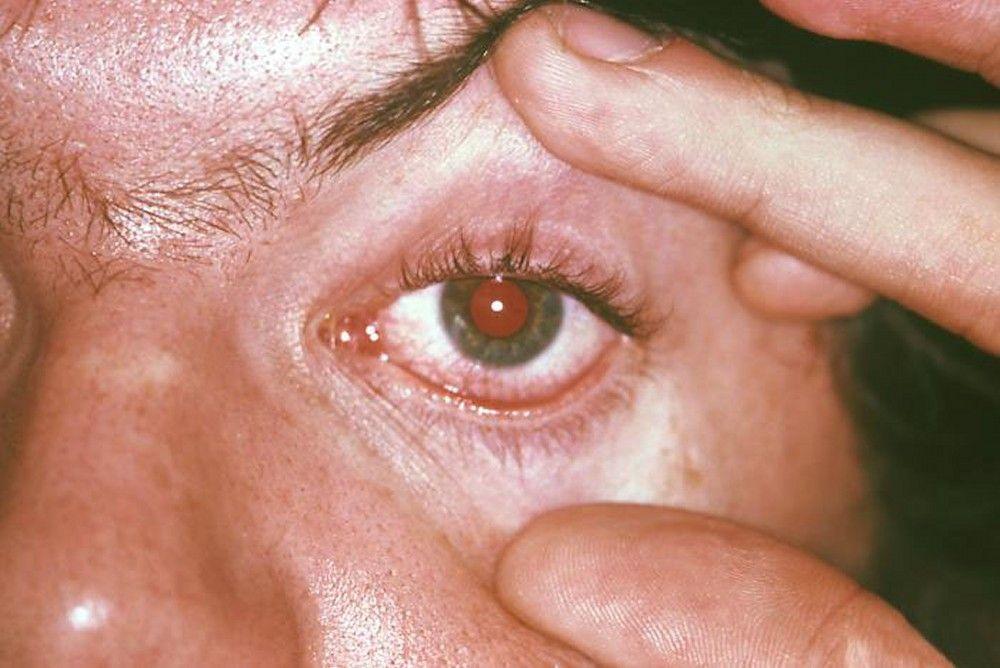
Image courtesy of Joe Miller via the Public Health Image Library of the Centers for Disease Control and Prevention.


Image courtesy of Drs. Weisner and Kaufman via the Public Health Image Library of the Centers for Disease Control and Prevention.
Infants born to women with chlamydial cervicitis may develop chlamydial pneumonia or ophthalmia neonatorum (neonatal conjunctivitis).
Diagnosis of Chlamydia
Nucleic acid–based tests of cervical, urethral, pharyngeal, or rectal exudate or urine
Chlamydial or mycoplasmal infection is suspected in patients with symptoms of urethritis, salpingitis, cervicitis, or unexplained proctitis, but similar symptoms can also result from gonococcal infection.
If clinical evidence for urethritis is uncertain, the Centers for Disease Control and Prevention (CDC) 2021 Sexually Transmitted Infections Treatment Guidelines state that urethritis can be documented by any of the following:
Mucoid, mucopurulent, or purulent discharge observed during examination
≥ 10 white blood cells per high-power field in spun first-void urine
A positive leukocyte esterase test on first-void urine
≥ 2 white blood cells per oil immersion field in Gram-stained urethral secretions
Samples of cervical or vaginal specimens or male urethral or rectal exudates are obtained to check for chlamydiae. Urine samples can be used as an alternative to cervical or urethral specimens. Throat and rectal swabs are needed to test for infection at those sites.
Commercially available nucleic acid amplification tests (NAATs) are highly sensitive and specific for chlamydia and can also be done on self-collected urine or vaginal specimens, eliminating the need for doing an uncomfortable swab of the urethra or cervix. Point-of-care NAAT platforms are available and can provide same-visit results. In general, samples from the throat and rectum should be tested only in laboratories that have verified the use of these tests for those anatomic sites.
Because other STIs (particularly gonococcal infection) often coexist, patients who have symptomatic urethritis should also be tested for gonorrhea. All patients who receive a diagnosis of gonorrhea or chlamydia should be tested for other STIs, including syphilis and HIV.
Mycoplasma genitalium can be detected using commercial NAAT assays, but those may not be widely available.
In the US, confirmed cases of chlamydial infection, gonorrhea, and syphilis must be reported to the public health system.
Screening for Chlamydia
Testing urine or self-collected vaginal swabs using NAAT is especially useful for screening asymptomatic people at high risk of STIs because genital examination is not necessary. Screening recommendations vary by sex, age, sexual practices, and setting. The following are based on the CDC's Sexually Transmitted Infections (STI) Treatment Guidelines, 2021.
Women are screened annually if they are sexually active and < 25 years of age or if they are ≥ 25 years of age, sexually active, and have one or more of the following risk factors:
Have a history of a prior STI
Engage in high-risk sexual behavior (eg, have a new sex partner or multiple sex partners; engage in sex work; or use condoms inconsistently when not in a mutually monogamous relationship)
Have a partner who has an STI or engages in high-risk behavior (eg, a sex partner who has concurrent partners)
Have a history of incarceration
Pregnant women who are < 25 years or who are ≥ 25 years with one or more of the risk factors are screened during their first prenatal visit and again during their 3rd trimester if risk remains high.
The American College of Obstetrics and Gynecology (ACOG) recommends that all pregnant women be tested for chlamydia early in pregnancy, with a repeat test in the 3rd trimester for women with risk factors. It recommends testing for gonorrhea in pregnant women ≤ 25 years and for those living in an area where gonorrhea is common. (See ACOG: Routine Tests During Pregnancy.)
Heterosexually active men are not routinely screened except for those in clinical settings with a high prevalence of chlamydial infection (eg, adolescent clinics, STI clinics, correctional facilities).
Men who have sex with men are screened at least annually if they have been sexually active within the previous year (for insertive intercourse, urine screen; for receptive intercourse, rectal swab; and for oral intercourse, pharyngeal swab), regardless of condom use. Those at increased risk (eg, with HIV infection, receive preexposure prophylaxis with antiretrovirals, have multiple sex partners, or whose partner has multiple partners) should be screened more frequently, at 3 to 6-month intervals.
Transgender and gender diverse people are screened if they are sexually active on the basis of sexual practices and anatomy (eg, annual screening for all people with a cervix who are < 25 years old; if ≥ 25 years old, people with a cervix should be screened annually if at increased risk; rectal swab based on reported sexual behaviors and exposure).
(See also the US Preventive Services Task Force’s summary of recommendations regarding screening for chlamydial infection.)
Treatment of Chlamydia
Empiric treatment for gonorrhea if it has not been excluded
Treatment of sex partners
Uncomplicated documented or suspected chlamydial infections are treated with one of the following:
1).
Patients who relapse (about 10%) are usually coinfected with microbes that do not respond to antichlamydial therapy, or they were reinfected since treatment.
They should be retested for chlamydial infection and gonorrhea and, if possible, for mycoplasma and trichomoniasis.
In areas where trichomoniasis
Current sex partners should be treated. Patients should abstain from sexual intercourse until they and their partners have been treated for ≥ 1 week.
If chlamydial genital infections are untreated, symptoms and signs subside within 4 weeks in about two thirds of patients. However, in women, asymptomatic cervical infection may persist, resulting in chronic endometritis, salpingitis, or pelvic peritonitis and their sequelae—pelvic pain, infertility, and increased risk of ectopic pregnancy. Because chlamydial infections can have serious long-term consequences for women, even when symptoms are mild or absent, detecting the infection in women and treating them and their sex partners is crucial.
Treatment references
1. Kong FYS, Tabrizi SN, Fairley CK, et al: The efficacy of azithromycin and doxycycline for the treatment of rectal chlamydia infection: a systematic review and meta-analysis. J Antimicrob Chemother 70: 1290–1297, 2015. doi: 10.1093/jac/dku574
2. Centers for Disease Control and Prevention: Sexually Transmitted Infections Treatment Guidelines, 2021: Mycoplasma genitalium. Accessed June 27, 2022.
Key Points
Sexually acquired chlamydial and mycoplasmal infections may affect the urethra, cervix, adnexa, throat, or rectum.
Diagnose using nucleic acid amplification tests.
Also test for coinfection with other STIs, including gonorrhea, syphilis, and HIV infection.
Screen high-risk, asymptomatic patients for chlamydial infection.
Use an antibiotic regimen that also treats gonorrhea if it has not been excluded.
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
US Preventive Services Task Force: Chlamydia and Gonorrhea: Screening: A review of evidence that screening tests can accurately detect chlamydia and gonorrhea
Centers for Disease Control and Prevention: Sexually Transmitted Infections Treatment Guidelines, 2021: Diseases Characterized by Urethritis and Cervicitis: Clinical guidance on treatment of STIs, prevention strategies, and diagnostic recommendations






