




Cricothyrotomy, whether traditional surgical cricothyrotomy or percutaneous cricothyrotomy using a guidewire, uses an incision through the skin and cricothyroid membrane through which an artificial airway is inserted into the trachea. Cricothyrotomy is typically done emergently, when endotracheal intubation is contraindicated or unachievable by other methods of tube insertion, and non-definitive methods of airway management and ventilation (eg, extraglottic devices such as a laryngeal mask airway) fail to adequately ventilate and oxygenate the patient.
(See also Airway Establishment and Control.)
Cricothyrotomy using a guidewire is similar to the Seldinger technique (catheter over guidewire) of central venous line insertion and may be more suitable for operators with limited surgical experience.
Needle cricothyrotomy, a temporary method that uses a 12- to 14-gauge angiocatheter attached to a bag-valve-mask device (or a jet ventilator if available), is the preferred cricothyrotomy method for children < 10 years old. This apparatus can be easily assembled by attaching the angiocatheter to a 3-mL syringe with the plunger removed. The adapter from a 6.5-mm endotracheal (ET) tube is then attached to the syringe, and the patient is ventilated using a bag-valve-mask device attached to the ET tube adapter.
Indications for Percutaneous Cricothyrotomy
Apnea, severe respiratory failure, or impending respiratory arrest requiring endotracheal intubation and either
Failed attempts at orotracheal or nasotracheal intubation with the inability to oxygenate or ventilate via alternate methods (eg, bag-valve-mask, supraglottic airway device)
Contraindications to orotracheal or nasotracheal intubation such as massive oral hemorrhage, severe facial trauma, or mass effect due to tumor
Contraindications to Percutaneous Cricothyrotomy
Absolute contraindications
Age < 8 years
Relative contraindications
Inability to identify landmarks due to significant injury to the larynx, thyroid cartilage, or cricoid cartilage
Partial or complete transection of the distal trachea
Age 8 to 12 (varying age cutoffs without definitive expert consensus)
Complications of Percutaneous Cricothyrotomy
Early complications, recognized immediately or within hours after cricothyrotomy, include the following:
Bleeding, sometimes uncontrollable
Insertion of tube into neck tissues rather than trachea, typically immediately recognized by absence of breath sounds on lung auscultation and remediated by reinsertion of tube into trachea
Injury to or perforation of the posterior aspect of the trachea
Larynx, vocal cord, or thyroid injury
Late complications, recognized weeks or months after cricothyrotomy, include the following:
Progressive airway obstruction due to subglottic stenosis and stomal granulation tissue
Voice changes, which are chronic but may resolve with time
Wound infection
Equipment for Percutaneous Cricothyrotomy
Sterile drapes
Sterile gloves and gowns along with eye and face protection (universal precautions)
Catheter-over-the-needle device capable of accommodating a guidewire, attached to a 3- to 6-mL syringe half-filled with saline
Flexible guidewire in a plastic housing
Airway catheter (tracheal tube) that has a plastic inflatable cuff and a removable intraluminal curved blunt dilator (which facilitates insertion)
#15 scalpel blade
Suction source and suction catheter
Bag-valve-mask and oxygen source
Patient monitoring equipment, including cardiac monitor, pulse oximeter, blood pressure monitor (noninvasive)
Capnometer (end-tidal carbon dioxide monitor), if available
Some commercially available kits contain all or some of these: airway catheter, guidewire, syringe, and catheter-over-needle device.
Additional Considerations for Percutaneous Cricothyrotomy
The cricothyroid membrane should be readily identifiable because with the guidewire technique often no skin incision is made initially. Anatomic distortions will make the cricothyroid membrane less identifiable.
Sterile technique is necessary to prevent local microbial contamination during the procedure.
Relevant Anatomy for Percutaneous Cricothyrotomy
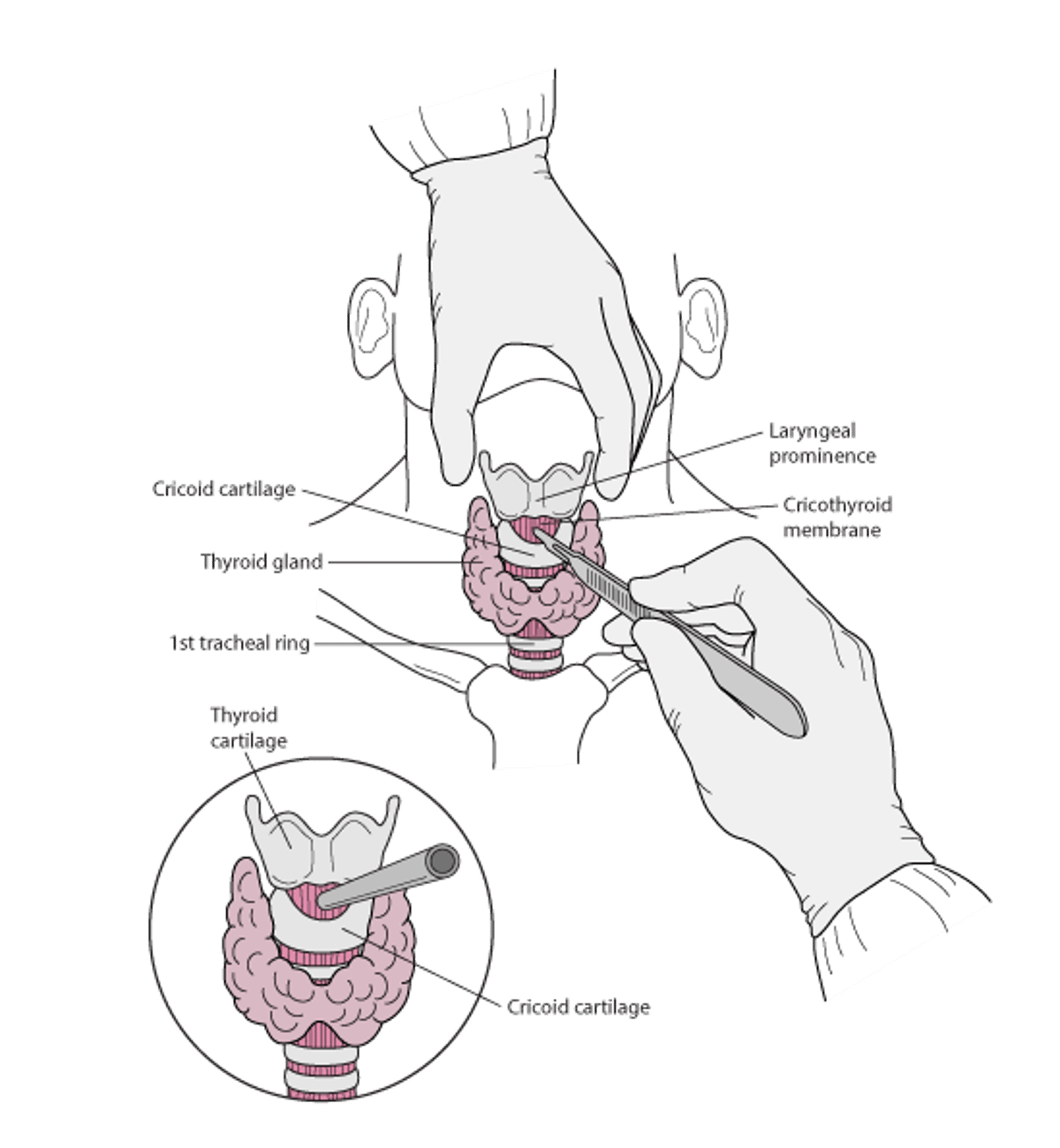
The cricothyroid membrane lies between the thyroid cartilage and the cricoid cartilage. The membrane is about 1 cm longitudinally and 2 to 3 cm transversely. Tracheal cartilages extend caudally from the cricoid cartilage to the sternal notch.
The area around the cricothyroid membrane is rich with blood vessels (superior thyroid arteries and the relatively uncommon variant thyroid ima arteries).
Emergency cricothyrotomy
The patient lies supine with the neck extended. After sterile preparation, the larynx is grasped with one hand while a blade is used to incise the skin, subcutaneous tissue, and cricothyroid membrane precisely in the midline, accessing the trachea. A hollow tube is used to keep the airway open. |

Positioning for Percutaneous Cricothyrotomy
Position the patient supine, and, if cervical spinal injury is not a concern, hyperextend the neck. The sniffing position is not necessary for cricothyrotomy.
Step-by-Step Description of Percutaneous Cricothyrotomy
To the extent possible, ensure adequate oxygenation and ventilation throughout this procedure, using a bag-valve-mask or laryngeal mask airway and supplemental oxygen (high-flow if readily available).
Test the cuff of the tracheal tube balloon for leaks by using a syringe to inflate it with air. Then deflate the balloon.
Apply a small amount of water-soluble lubricant to the dilator/airway assembly, including the balloon cuff, using a gloved finger.
Attach a syringe, half-filled with saline, to the insertion needle.
Identify the cricothyroid membrane. Move your finger caudally from the laryngeal prominence (the most prominent part of the anterior thyroid cartilage) until you feel the cricothyroid membrane, palpable as a step-off between the caudal end of the thyroid cartilage and the cricoid cartilage.
Inject a local anesthetic along the anticipated skin incision site (see next bullet) if the patient is capable of feeling pain.
Stabilize the larynx with your non-dominant hand by grasping the sides of the thyroid cartilage with your thumb and middle finger. Maintain stabilization until the airway catheter is in place.
Some operators make a 2- to 3-cm midline longitudinal incision using a scalpel over the skin and subcutaneous tissues over the cricothyroid membrane.
Insert the needle (typically within a catheter), with the fluid-containing syringe attached, through the cricothyroid membrane, aiming caudally at an angle of about 45 degrees. Keep back-pressure on the syringe plunger as you advance.
Confirm needle placement in the airway by feeling a pop as the needle enters the trachea and by seeing air entering the syringe, visible as air bubbles in the saline. Stop advancing the needle as soon as air is returned.
Remove the syringe from the needle. If a catheter lies over the needle, advance the catheter and withdraw the needle.
Thread the flexible tip of the guidewire through the needle or catheter and into the trachea.
While maintaining firm control of the guidewire, gently remove the needle or catheter, leaving the guidewire in place.
Make a skin incision directly below the guidewire insertion site (if not previously made) to facilitate passage of the blunt dilator and airway, which are advanced as a unit into the trachea. Carefully guide the dilator over the guidewire. Be sure the guidewire passes through the dilator and that you control the proximal end of the wire before proceeding (so the guidewire is not lost within the airway).
Dissect the site further as needed to facilitate passage of the device through the tissues and into the trachea. If resistance to passage is significant, try using gentle but steady force, rotating the unit as it advances, and using further dissection if needed. Fully inserted, the hub and flange of the airway catheter should be flush against the skin.
Withdraw the guidewire and the dilator.
Inflate the balloon cuff to the minimum volume needed for effective ventilation.
Resume ventilation using the newly established airway.
Secure the device in place using cloth or tape threaded through the catheter flanges.
When the airway is secure, confirm proper airway placement using auscultation and end-tidal carbon dioxide detection.
Aftercare for Percutaneous Cricothyrotomy
A chest x-ray can be done to confirm placement.
The cricothyrotomy is generally viewed as a bridge to a more permanent tracheostomy, which is traditionally done within 72 hours of the initial emergent cricothyrotomy. The conversion to tracheostomy is thought to decrease the risk of subglottic stenosis; however, there is no strong literature supporting this mandated conversion.
Tips and Tricks for Percutaneous Cricothyrotomy
A battery-powered electrocautery device can often be used to help control any significant bleeding due to the vertical skin incision.






