




Pulmonary hypertension is a condition in which blood pressure in the arteries of the lungs (the pulmonary arteries) is abnormally high.
Many disorders can cause pulmonary hypertension.
People usually have shortness of breath with even mild exercise and loss of energy, and some people feel light-headed or fatigued with even mild exercise.
Chest x-rays, electrocardiography (ECG), and echocardiography give clues to the diagnosis, but measurement of blood pressure in the right ventricle and the pulmonary artery is needed for confirmation.
Treatment of the cause and use of drugs that improve blood flow through the lungs are helpful.
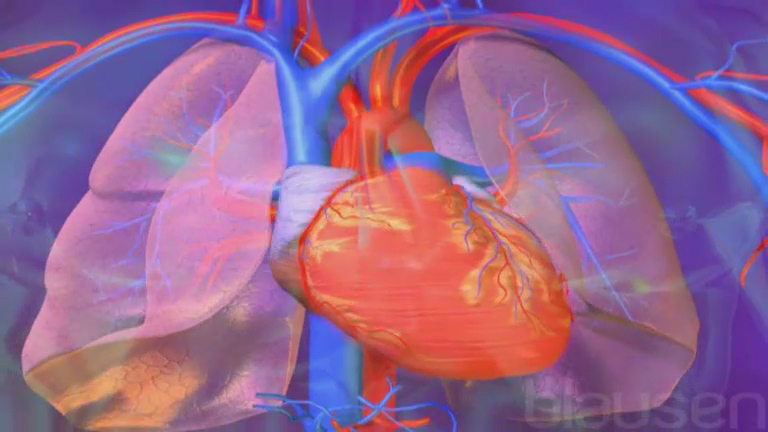
Blood travels from the right side of the heart through the pulmonary arteries into the small blood vessels of the lungs (the capillaries) where carbon dioxide is removed from the blood and oxygen is added. Normally, the pressure in the pulmonary arteries is low, allowing the right side of the heart to be less muscular than the left side (because relatively little muscle and effort are needed to push the blood through the lungs via the pulmonary arteries). In contrast, the left side of the heart is more muscular because it has to push blood through the entire body against a much higher pressure.
If the pressure of the blood in the pulmonary arteries increases to a sufficiently high level, the condition is called pulmonary hypertension. In pulmonary hypertension, the right side of the heart must work harder to push the blood through the pulmonary arteries. Over time, the right ventricle becomes thickened and enlarged and cor pulmonale develops, resulting in right-sided heart failure.
Causes of Pulmonary Hypertension
Pulmonary hypertension is currently classified into the following 5 groups based on the cause of the disease:
Pulmonary arterial hypertension
Left-sided heart disease (heart failure and valvular heart disease)
Lung disorders or low blood oxygen levels
Chronic disorders that cause blood clots
Other mechanisms
Pulmonary arterial hypertensioncocaine, and selective serotonin reuptake inhibitors (SSRIs). If SSRIs are taken by pregnant women after 20 weeks of pregnancy, risk of pulmonary hypertension in the newborn is higher than normal. Pulmonary arterial hypertension can also develop in people who have certain disorders, such as portal hypertension, HIV infection, congenital heart diseases, schistosomiasis, and systemic sclerosis (scleroderma).
Left-sided heart disease is one of the most common causes of pulmonary hypertension. Left-sided heart disease can occur in people who have longstanding high blood pressure or coronary artery disease. When the left side of the heart cannot pump blood out to the body normally, blood backs up in the lungs and increases blood pressure there. Inability of the heart to relax appropriately can also cause blood to back up into the lungs, which contributes to pulmonary hypertension.
Lung disorders or low blood oxygen levels can also lead to pulmonary hypertension. When the lungs are impaired by a disorder, more effort is needed to pump blood through them. One of the most common conditions is chronic obstructive pulmonary disease (COPD). Over time, COPD destroys the small air sacs (alveoli) together with their small blood vessels (capillaries) in the lungs. The single most important cause of pulmonary hypertension in COPD is the narrowing (constriction) of the pulmonary arteries that occurs as a result of low blood oxygen levels. Other conditions that lower blood oxygen levels, such as having sleep apnea, or living in or prolonged visiting in places that are at high altitudes can also cause pulmonary hypertension. Other lung disorders that may cause pulmonary hypertension include pulmonary fibrosis, cystic fibrosis, sarcoidosis, and extensive loss of lung tissue as a result of surgery or injury.
Certain chronic disorders can cause repeated (chronic) blood clots, typically blood clots in the deep leg veins (called deep vein thrombosis). Blood clots in the leg may dislodge and travel through the venous system and the right side of the heart to lodge in the pulmonary arteries or the smaller branches of these arteries in the lungs, causing pulmonary embolism. If these clots do not resolve properly, the pulmonary arteries can become narrower and stiffer. This results in a type of pulmonary hypertension called chronic thromboembolic pulmonary hypertension.
Disorders that cause pulmonary hypertension by other mechanisms include blood (hematologic) disorders (such as chronic hemolytic anemia, myeloproliferative disorders, and splenectomy), systemic disorders (such as sarcoidosis, pulmonary Langerhans cell histiocytosis, and lymphangioleiomyomatosis), and some other disorders.
Symptoms of Pulmonary Hypertension
Shortness of breath during exertion is the most common symptom of pulmonary hypertension, and virtually everyone who has the condition develops it. Some people feel light-headed or fatigued during exertion. The person is likely to feel weak because body tissues are not receiving enough oxygen.
Other symptoms, such as coughing (rarely, coughing up blood) and wheezing, are usually caused by the underlying lung disorder. Swelling (edema), particularly of the legs, may occur because fluid may leak out of the blood vessels and into the tissues. Swelling is usually a sign that right-sided heart failure has developed. Rarely, people with pulmonary hypertension become hoarse.
Diagnosis of Pulmonary Hypertension
Chest x-ray, echocardiography, and electrocardiography
Cardiac catheterization
Based on the symptoms, doctors may suspect pulmonary hypertension, particularly in people who have an underlying lung disorder or other known cause of pulmonary hypertension. Tests, including a chest x-ray, echocardiography, and electrocardiography, are done. A chest x-ray may show that the pulmonary arteries are enlarged. Electrocardiography (ECG) and echocardiography enable doctors to look for certain problems with the right side of the heart before cor pulmonale develops. For example, thickening of the right ventricle or a partial reversal (back flow) of blood through the tricuspid valve between the right ventricle and the right atrium may be detected on an echocardiogram.
Pulmonary function tests help doctors assess the extent of lung damage. A sample of blood may be taken from an artery in an arm to measure the level of oxygen in the blood.
A definite diagnosis of pulmonary hypertension usually requires passing a tube through a vein in an arm or a leg into the right side of the heart to measure the blood pressure in the right ventricle and the pulmonary artery (right heart catheterization).
Other tests may be done to help determine the cause of pulmonary hypertension and to measure its severity. For example, testing may include high-resolution computed tomography (CT) of the chest (for detailed information about lung disorders), blood tests to identify autoimmune disorders, and CT angiography to look for blood clots in the lungs. Testing for gene mutations may be done to look for causes of hereditary pulmonary arterial hypertension.
Treatment of Pulmonary Hypertension
Treatment of the cause of pulmonary hypertension
Often treatments to relieve symptoms, such as drugs that widen (dilate) blood vessels and supplemental oxygen
Sometimes treatments to prevent or treat complications, such as anticoagulants and lung transplantation
Treatment of pulmonary hypertension is best directed at the cause when the cause has been identified.
Vasodilators (drugs to dilate blood vessels) work by reducing blood pressure in the pulmonary arteries. Vasodilators may improve quality of life, prolong survival, and prolong the time until lung transplantation needs to be considered. Before administering vasodilators, however, doctors may first test the effectiveness of these drugs while the person is in a cardiac catheterization laboratory because use of these drugs may be dangerous in some people. Vasodilators have not proved effective for people with pulmonary hypertension due to chronic obstructive pulmonary disease (COPD). In contrast, vasodilators are often helpful for pulmonary hypertension that occurs in people with the following:
Idiopathic or inherited pulmonary hypertension
Autoimmune disorders
Chronic liver disease
HIV infection
Some congenital heart disorders
Pulmonary hypertension caused by drugs or toxins
Chronic thromboembolic pulmonary hypertension
In people with pulmonary hypertension who have a low level of oxygen in the blood, the continuous use of oxygen through nasal prongs or an oxygen mask may reduce blood pressure in the pulmonary arteries and may relieve shortness of breath. A diuretic drug is usually given to assist the right ventricle in maintaining a normal volume for effective beating and to reduce leg swelling. An anticoagulant may also be given to reduce the risk of blood clots and subsequent pulmonary embolism.
Lung transplantation is an established procedure for treating people with pulmonary hypertension. Lung transplantation can be used only in people with severe disease who are healthy enough to withstand the potential consequences and difficulties with the procedure.






