




Gait disorders are abnormalities in how people walk, such as losing speed, smoothness, symmetry, or balance.
Walking, standing up from a chair, turning, and leaning are important for being able to move around independently. Gait speed, the time it takes to stand up out of a chair, and the ability to stand with one foot in front of the other (tandem stance) help predict an older person's ability to do daily and other activities such as shopping, traveling, and cooking.
Walking without assistance requires coordination by areas of the brain that control attention, strength, sensation, and coordination of the perceptions of the senses and muscle contraction (see figure Using the Brain to Move a Muscle) for safe and steady walking. Dementia and other neurologic disorders can significantly affect walking by impairing these areas of the brain.
Normal Age-Related Changes in Gait
Some elements of gait normally change as people get older; others do not.
Speed of walking (gait velocity) remains the same until about age 70, and then it slows down. Speed of walking is a powerful predictor of mortality—as powerful as the number of chronic medical conditions and hospitalizations a person has. At age 75, slow walkers die 6 years or more before walkers with a normal speed and 10 years or more before fast walkers.
Speed of walking slows because older people take shorter steps. The most likely reason for shortened step length (the distance from one heel strike to the next) is weakness of the calf muscles. Calf muscles propel the body forward, and calf muscle strength declines with age. However, older people seem to compensate for decreased calf strength by using their hip flexor and extensor muscles more than young adults.
Cadence, which is the number of steps taken in a minute, does not slow down with age. Every person has a preferred cadence, which is related to leg length. Tall people take longer steps at a slower cadence; short people take shorter steps at a faster cadence.
Double stancetime refers to the time when both feet are on the ground while taking a step. This phase of a step is a more stable position for moving forward than when only one foot is on the ground. The percentage of time spent in double stance increases with age. Older people may increase the time spent in double stance even more when they walk on uneven or slippery surfaces, when they feel off-balance, or when they are afraid of falling. They may appear as if they are walking on slippery ice.
Walking posture changes only slightly with aging. Older people walk upright, with no forward lean. However, older people walk with more downward rotation of the pelvis and with an increased curve of the lower back (called lumbar lordosis). Usually, weak abdominal muscles, tight hip flexor muscles, and increased abdominal fat contribute to this change in posture. Older people also walk with their legs rotated laterally (toes out) about 5 degrees, possibly because their hips are less able to turn inward or they are trying to increase stability. Foot clearance in swing is unchanged with age.
Abnormal Changes in Gait
A number of disorders can contribute to a dysfunctional or unsafe gait. Common causes are
Neurologic disorders, including dementia and Parkinson disease
Muscle or bone disorders, including spinal stenosis
A gait can be abnormal in various ways, and certain types of abnormalities help doctors understand what is causing the gait problem.
Asymmetry: When healthy, a person’s body moves symmetrically while walking (that is, motions are equal on the right and left sides). If a person consistently does not have symmetry while walking, the cause is often a problem with nerves or bones and joints on one side of the body—for example, a limp caused by a painful hip or ankle. If the reason for the lack of symmetry is not obvious, the cause may be malfunction of the brain or the use of certain drugs.
Loss of synchrony: Normal synchrony of gait involves moving the upper and lower limbs in a regular, rhythmic way and smooth coordination of the limbs. Synchrony enables a person to move forward. Neurologic or musculoskeletal disorders that affect specific aspects of gait result in loss of synchrony.
Difficulty starting or continuing to walk: Older people may have difficulty starting or continuing to walk. When they start to walk, their feet may appear stuck to the floor, typically because they do not shift their weight to one foot to allow the other foot to move forward. Doctors may look for a movement disorder, such as Parkinson disease, to find the cause of this gait problem. Once gait is started, a person's steps should be continuous, with little variability in the timing of the steps. Freezing, stopping, or almost stopping usually suggests a cautious gait, a fear of falling, or a problem with the frontal lobe of the brain. Scuffing the feet is not normal (and is a risk factor for tripping). Causes of scuffing include Parkinson disease and weakness and/or numbness of the feet caused by nerve damage.
Retropulsion: Retropulsion is when a person unintentionally steps backward when trying to start walking or falls backward while walking. Doctors may look for a problem with the front lobes of the brain, parkinsonism, syphilis, small strokes, or progressive supranuclear palsy as the possible cause.
Footdrop: Footdrop is difficulty lifting the front part of the foot because of weakness or paralysis of the muscles involved. A person's toe drags when taking a step. To avoid catching the toe, people with a dropped foot may lift their leg higher than normal during a step. Footdrop may be caused by nerve damage or muscle weakness.
Short step length: Short step length may be caused by a fear of falling or by a nerve or muscle problem. The leg with the short step is usually the healthy one, and the short step usually occurs when a person spends less time on the problem leg than on the normal leg during walking.
Increased step width: As gait speed decreases, step width normally increases slightly. A wide-based gait can be caused by a problem in the knees, hips,the brain's cerebellum. Variable step width (lurching to one or both sides) may be due to poor muscle control because of a problem in the brain.
Circumduction: Circumduction is moving the foot in an arc rather than a straight line when stepping forward. Circumduction may caused by pelvic muscle weakness or difficulty bending the knee.
Forward lean: Leaning forward while walking can occur in people with kyphosis, Parkinson disease, or certain types of dementia (particularly vascular dementia and Lewy body dementia).
Festination: Festination is a progressive quickening of steps (usually while leaning forward) that can cause a person to break into a run to prevent falling forward. Festination can occur in people with Parkinson disease and rarely as a side effect of dopamine-blocking medications (such as certain antipsychotics).
Trunk lean: A person whose trunk leans sidewards may be compensating for joint pain due to arthritis or foot drop.
Arm swing changes: People with Parkinson disease or vascular dementia may swing their arms less while walking or not swing them at all. Side effects of dopamine-blocking medications can also cause changes in arm swing.
Evaluation of Gait
Doctors try to determine as many potential contributing factors to gait disorders as possible by
Discussing the person’s complaints, fears, and goals related to mobility
Observing gait with and without an assistive device, such as a cane or walker (if safe)
Assessing all components of gait (initiation of gait, right step length and height, left step length and height, and symmetry)
Observing gait again with a knowledge of the person’s gait components
Doctors do a physical examination and ask open-ended questions about any difficulty with walking, balance, or both, including whether the person has fallen (or fear they might fall). Doctors also ask about specific capabilities, such as whether the person can go up and down stairs; get in and out of a chair, shower, or tub; and walk as needed to buy and prepare food and do household tasks. Doctors also assess the person's muscle strength, especially in the calves and thighs.
Sometimes doctors do tests, including computed tomography (CT) or magnetic resonance imaging (MRI), to determine whether the abnormal gait is due to a disorder of the brain, spine, or other part of the body.
Treatment of Gait Disorders
A gait disorder does not always need to be treated or modified. A slow, abnormal gait may help an older person walk safely and without assistance. However, doctors may offer to treat a person's gait to help improve quality of life. Treatments include exercise, balance training, and assistive devices.
Strength training
Frail older people with mobility problems may improve with an exercise program. Walking or strength (resistance) training may reduce knee pain and improve gait in people with arthritis. Resistance exercises can improve strength, especially if the person is frail and has a slow gait. People usually need two or three training sessions a week until reaching their strength goal. Using good form during each exercise is important to reduce soreness or injury.
A combination of leg press machines (or alternatively chair rises with weight vests or weights attached to the waist), step ups, stair climbing, and knee extension machines may be recommended to strengthen all the large muscle groups involved in walking.
Nordic walking
Nordic walking is a walking exercise that exercises the whole body. It includes adjustable length walking poles. Compared with traditional walking, the Nordic walking motion uses shoulder and arm muscles and requires greater pelvic rotation, increasing step length and walking speed. When starting a Nordic walking program, frail walkers need supervision and training to use the walking sticks safely.
Balance training
Many people with balance problems improve with balance training. First, health care professionals help teach people a good standing posture and balance while standing still. People are then taught to be aware of the location of pressure on their feet and how the location of pressure moves with slow leaning or turning to look to the left or right. People practice leaning forward (using a wall or counter for support), backward (with a wall directly behind), and to each side. The goal is to be able stand on one leg for 10 seconds.
Balance training can also be more dynamic. Dynamic balance training can involve slow movements in a single stance, simple tai chi movements, tandem (heel to toe) walking, turns while walking, walking backward, walking over a virtual object (for example, a stripe on the floor), slow forward lunges, and slow dance movements.
Assistive devices
Assistive devices, such as canes and walkers, can help people maintain mobility and quality of life. Physical therapists help select the proper device and teach people how to use it.
Canes are particularly helpful for people with pain caused by knee or hip arthritis or with peripheral neuropathy of the feet because a cane transmits information about the type of surface or floor to the cane-holding hand. A quad cane (one with four small feet at the bottom) can stabilize the patient but usually slows gait. Canes are usually used on the side opposite the painful or weak leg. Many store-bought canes are too long but can be adjusted to the correct height (see figure Just the Right Height).
Walkers can reduce the force and pain at an arthritic joint more than a cane, in people with enough arm and shoulder strength to use them. Walkers provide good stability and moderate protection from forward falls but do little or nothing to help prevent backward falls for people with balance problems. When prescribing a walker, a physical therapist considers the sometimes competing needs of providing stability and maximizing walking efficiency. Four-wheeled walkers with larger wheels and brakes maximize efficiency but provide less stability.
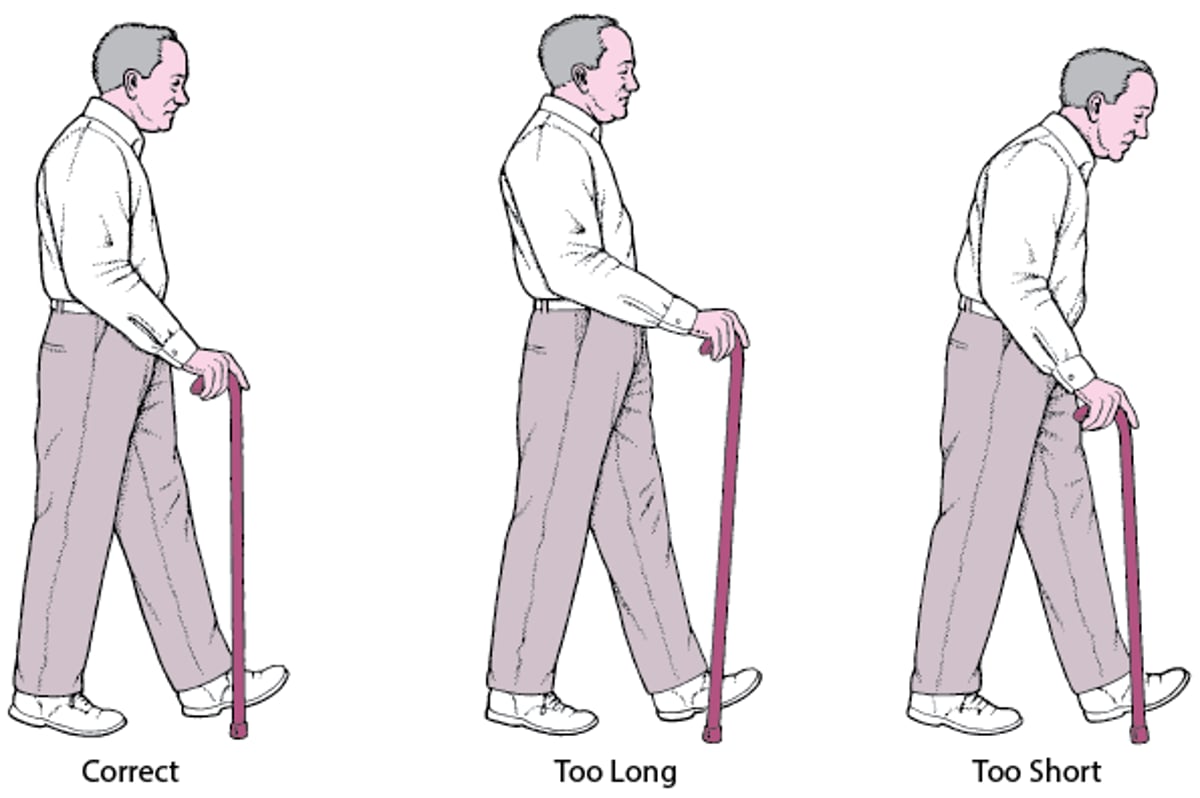
Just the Right Height
Using a cane that is the correct height is important. A cane that is too long or too short can cause low back pain, poor posture, and instability. The cane should be held on the side opposite the weak leg. |

Prevention of Gait Disorders
Physical activity, done at recommended levels, help older people maintain mobility, even in people with disease.
Regular walking or maintaining a physically active lifestyle is critical to keeping a healthy gait. The adverse effects of being inactive cannot be overstated. A regular walking program of 30 minutes each day is the best single activity for maintaining mobility. However, walking on flat terrain does not increase strength in a person who is weak. Including inclined surfaces, such as hills, during the walk can help maintain leg strength. The use of canes or walking sticks that are adjustable can provide confidence and safety for older adults.
Prevention also includes strength and balance training.




