




Lung abscess is a necrotizing lung infection characterized by a pus-filled cavitary lesion. It is most commonly caused by aspiration of oral secretions by patients who have impaired consciousness. Symptoms are productive cough, fever, sweats, and weight loss. Diagnosis is based primarily on chest x-ray. Treatment usually is with a combination beta-lactam/beta-lactamase inhibitor or a carbapenem.
Etiology of Lung Abscess
Aspiration of oral secretions (most common)
Endobronchial obstruction
Hematogenous seeding of the lungs (less common)
Most lung abscesses develop after aspiration of oral secretions by patients with gingivitis or poor oral hygiene. Typically, patients have altered consciousness as a result of alcohol, recreational drugs, anesthesia, sedatives, or opioids. Older patients and those unable to handle their oral secretions, often because of neurologic disease, are also at risk.
Lung abscesses can also develop secondary to endobronchial obstruction (eg, due to bronchial carcinoma) or to immunosuppression (eg, due to HIV/AIDS or after transplantation and use of immunosuppressive drugs).
A less common cause of lung abscess is necrotizing pneumonia that may develop from hematogenous seeding of the lungs due to suppurative thromboembolism (eg, septic embolism due to IV drug use or Lemierre syndrome) or right-sided endocarditis. In contrast to aspiration and obstruction, these conditions typically present acutely and cause multiple rather than isolated lung abscesses.
Direct infection (eg, from empyema, subphrenic or mediastinal abscess) rather than hematogenous seeding is possible with certain pyogenic bacteria (eg, Staphylococcus aureus).
Pathogens
The most common pathogens of lung abscesses due to aspiration are anaerobic bacteria, but about half of all cases involve both anaerobic and aerobic organisms (see table Infectious Causes of Cavitary Lung Lesions).
The most common anaerobic pathogens are
Peptostreptococcus
Fusobacterium
Prevotella
Bacteroides
The most common aerobic pathogens are
Staphylococci—sometimes methicillin-resistant Staphylococcus aureus (MRSA)
Occasionally, cases are due to gram-negative bacteria, especially Klebsiella. Immunocompromised patients with lung abscess are most commonly infected with Pseudomonas aeruginosa or other gram-negative bacilli but also may have infection with Nocardia, mycobacteria, or fungi.
Rare cases of pulmonary gangrene (extensive necrosis involving a lobe or a lung) or fulminant pneumonia with sepsis have been reported with pathogens such as MRSA, Pneumococcus, and Klebsiella. Some patients are at risk of abscess due to Mycobacterium tuberculosis, and rare cases are due to amebic infection (eg, with Entamoeba histolytica), hydatid cysts, paragonimiasis, or infection with Burkholderia pseudomallei.
Introduction of these pathogens into the lungs first causes inflammation, which, over a week or two, leads to tissue necrosis and then abscess formation. The abscess usually ruptures into a bronchus, and its contents are expectorated, leaving an air- and fluid-filled cavity. In about 10% of cases, direct or indirect extension (via bronchopleural fistula) into the pleural cavity can result in empyema.
Symptoms and Signs of Lung Abscess
Symptoms of abscess due to anaerobic bacteria or mixed anaerobic and aerobic bacteria are usually chronic (eg, occurring over weeks or months) and include productive cough, fever, night sweats, and weight loss. Patients may also present with hemoptysis and pleuritic chest pain. Sputum may be purulent or blood-streaked and classically smells or tastes foul. Patients may have fetid breath.
Symptoms of abscess due to aerobic bacteria develop more acutely and resemble bacterial pneumonia. Abscesses due to organisms other than anaerobes (eg, Mycobacteria, Nocardia) lack putrid respiratory secretions and may be more likely to occur in nondependent lung regions.
Signs of lung abscess, when present, are nonspecific and resemble those of pneumonia: decreased breath sounds indicating consolidation or effusion, temperature ≥ 38° C, crackles over the affected area, egophony, and dullness to percussion in the presence of effusion. Patients typically have signs of periodontal disease and a history of a predisposing cause of aspiration, such as dysphagia or a condition causing impaired consciousness.
Diagnosis of Lung Abscess
Chest x-ray
Often chest CT for better visualization or if endobronchial obstruction is suspected
Sputum cultures for aerobic bacteria, fungi, and mycobacteria
Bronchoscopy as needed to exclude cancer, detect unusual pathogens such as fungi or mycobacteria, and in immunocompromised patients
Culture of any pleural fluid
Lung abscess is suspected based on history in a patient who is at risk (eg, aspiration-prone due to altered consciousness or dysphagia or who is immunosuppressed) and is confirmed by chest x-ray showing cavitation.
Cavitary pulmonary lesions are not always caused by infection. Noninfectious causes of cavitary pulmonary lesions include the following:
Empyema or bulla with air-fluid level
Cystic (saccular) bronchiectasis
Lung infarction
Nodular silicosis nodule with central necrosis
Pulmonary sequestration
In an anaerobic infection due to aspiration, chest x-ray classically shows consolidation with a single cavity containing an air-fluid level in portions of the lung that would be dependent when the patient is recumbent (eg, the posterior segments of the upper lobes or the superior or lateral basal segments of the lower lobes). This pattern helps distinguish anaerobic abscess from other causes of cavitary pulmonary disease, because diffuse or embolic pulmonary disease often causes multiple cavitations, and tuberculosis typically involves the apices.
CT is not routinely needed (eg, if cavitation is clear on chest x-ray in a patient who has risk factors for lung abscess). However, CT may be useful when cavitation is suggested but not clearly seen on the chest x-ray, when an underlying pulmonary mass obstructing the drainage of a lung segment is suspected, or when abscess needs to be differentiated from empyema or bulla with an air-fluid level.

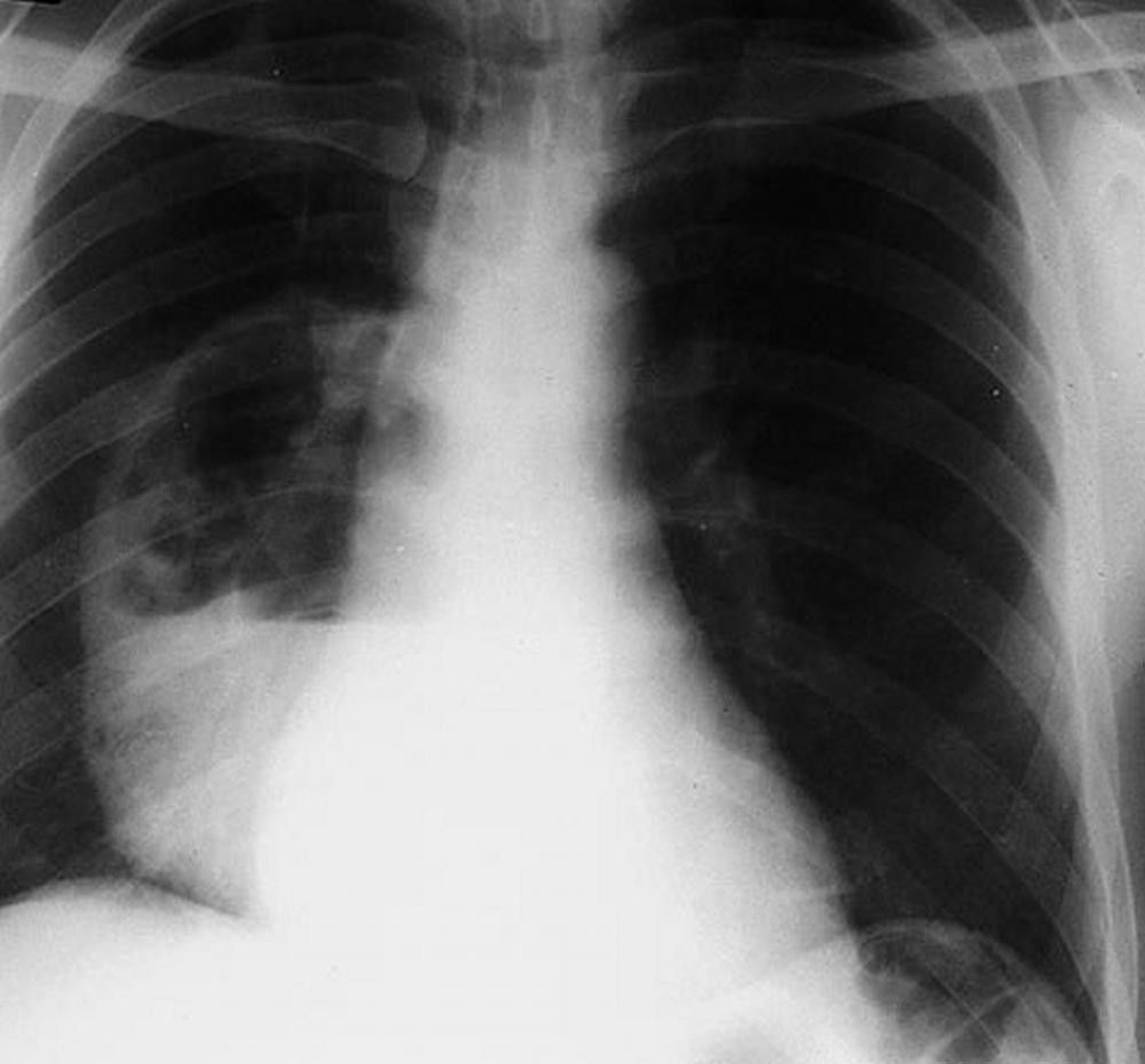
By permission of the publisher. From Leaf H. In Atlas of Infectious Diseases: Pleuropulmonary and Bronchial Infections. Edited by GL Mandell (series editor) and MS Simberkoff. Philadelphia, Current Medicine, 1996.
Bronchial carcinoma can lead to obstruction that causes pneumonia and abscess formation. Bronchial carcinoma should be suspected in patients who do not respond to antimicrobial treatment or have atypical findings such as a cavitary lesion and no fever. Bronchoscopy is sometimes done to exclude cancer or the presence of a foreign body or to detect unusual pathogens, such as fungi or mycobacteria. Bronchoscopy is done if patients are immunocompromised.
Cultures
Anaerobic bacteria are rarely identifiable on culture because uncontaminated specimens are difficult to obtain and because most laboratories do not culture anaerobes well or often. If sputum is putrid, then anaerobic infection is assumed to be the cause. However, if empyema is present, pleural fluid provides a good source for anaerobic culture.
When clinical findings make anaerobic infection less likely, aerobic, fungal, or mycobacterial infection should be suspected, and attempts should be made to identify a pathogen. Cultures of sputum, bronchoscopic aspirates, or both are helpful.
Treatment of Lung Abscess
IV antibiotics or, for less seriously affected patients, oral antibiotics
Percutaneous, endobronchial, or surgical drainage of any abscess that does not respond to antibiotics or of any empyema
If gram-negative bacilli are cultured in significant concentrations from sputum or blood and are identified on gram stain, the antibiotic regimen should be modified to cover the specific pathogen in addition to anaerobes.
Clostridioides (formerly, Clostridium) difficile
Optimal duration of treatment is unknown, but common practice is to treat until the chest x-ray shows complete resolution or a small, stable, residual scar, which generally takes 3 to 6 weeks or longer. In general, the larger the abscess, the longer it will take for x-rays to show resolution.
Most authorities do not recommend chest physical therapy and postural drainage because of the potential for spillage of infection into other bronchi with extension of the infection or acute obstruction.
An accompanying empyema must be drained. Surgical removal or drainage of lung abscesses is necessary in the roughly 10% of patients in whom lesions do not respond to antibiotics, and in those who develop pulmonary gangrene. Resistance to antibiotic treatment is most common with large cavities and with post-obstructive abscesses. If patients fail to defervesce or to improve clinically after 7 to 10 days, they should be evaluated for resistant or unusual pathogens, airway obstruction, and noninfectious causes of cavitation.
When surgery is necessary, lobectomy is the most common procedure; segmental resection may suffice for small lesions (< 6 cm diameter cavity). Pneumonectomy may be necessary for multiple abscesses unresponsive to drug therapy or for pulmonary gangrene. In patients likely to have difficulty tolerating surgery, percutaneous drainage or, rarely, bronchoscopic placement under ultrasound guidance of a pigtail catheter can help facilitate drainage. .
Key Points
Lung abscesses are most often caused by aspiration of oral secretions by patients who have impaired consciousness; thus, anaerobic bacteria are among the common pathogens.
Suspect lung abscess in patients prone to aspiration, who have subacute constitutional and pulmonary symptoms, and whose chest x-ray shows compatible lesions such as cavities.
Treat initially with antibiotics; if patients do not respond within 7 to 10 days, evaluate them for unusual or resistant pathogens, bronchial obstructive lesions, and noninfectious causes of lung cavitation.
Drain empyemas and consider surgical removal or drainage of lung abscesses that do not respond to drug therapy and for pulmonary gangrene.




