




Cardiac catheterization is the passage of a catheter through peripheral arteries or veins into cardiac chambers, the pulmonary artery, and coronary arteries and veins.
Cardiac catheterization can be used to do various tests, including
Angiography
Detection and quantification of shunts
Endomyocardial biopsy
Intravascular ultrasonography (IVUS)
Measurement of cardiac output (CO)
Measurements of myocardial metabolism
These tests define coronary artery anatomy, cardiac anatomy, cardiac function, and pulmonary arterial hemodynamics to establish diagnoses and help clinicians select treatment.
Cardiac catheterization is also the basis for several therapeutic interventions (see Percutaneous coronary intervention in Treatment of Coronary Artery Disease).
Procedure for Cardiac Catheterization
Many but not all preprocedure protocols require patients to fast for 4 to 6 hours before cardiac catheterization. Most patients do not require overnight hospitalization unless a therapeutic intervention is also done.
Left heart catheterization
Left heart catheterization is most commonly used to assess
Coronary artery anatomy and presence of coronary artery disease
Left heart catheterization is also used to assess
Aortic blood pressure
Aortic valve function
Left ventricular pressure and function
Mitral valve function
Systemic vascular resistance
Left heart catheterization is done via femoral, subclavian, radial, or brachial artery puncture, with a catheter passed into the coronary artery ostia and/or across the aortic valve into the left ventricle (LV).
Catheterization of the left atrium (LA) and LV is occasionally done using transseptal perforation during right heart catheterization.
Right heart catheterization
Right heart catheterization is commonly used to measure
Right atrial pressure
Right ventricular pressure
Pulmonary artery pressure
Pulmonary artery occlusion pressure (PAOP—see figure Diagram of the Cardiac Cycle)
The most frequent indications for right heart catheterization are to assess hemodynamics, diagnose pulmonary hypertension, guide therapy, and assess need for cardiac transplantation or mechanical cardiac support (eg, a ventricular assist device).
PAOP approximates left atrial and left ventricular end-diastolic pressure. In seriously ill patients, PAOP helps assess volume status and, with simultaneous measurements of cardiac output, can help guide therapy.
Right heart catheterization is also useful for assessing cardiac filling pressures, pulmonary vascular resistance, tricuspid or pulmonic valve function, intracardiac shunts, and right ventricular pressure.
Right heart pressure measurements may help in the diagnosis of cardiomyopathy, constrictive pericarditis, and cardiac tamponade. when noninvasive testing is nondiagnostic, and it is an essential part of the assessment for cardiac transplantation or mechanical cardiac support (eg, use of a ventricular assist device).
The procedure is done via femoral, subclavian, internal jugular, or antecubital vein puncture. A catheter is passed into the right atrium, through the tricuspid valve, into the right ventricle, and across the pulmonary valve into the pulmonary artery.
Selective catheterization of the coronary sinus can also be done.
Hemodynamic assessment via right heart catheterization during exercise is increasingly being done as part of the workup for dyspnea of uncertain etiology. The test can be done at the same time as cardiopulmonary exercise testing, called invasive cardiopulmonary exercise testing. This is considered the standard for diagnosis of cardiac limitation to exercise but is currently available at relatively few centers. An exercise right heart catheterization should be considered in patients at intermediate pretest probability for heart failure with preserved ejection fraction if the diagnosis is uncertain after an initial evaluation. An increase in the PAOP > 25 mm Hg confirms the diagnosis when patients have signs and symptoms of heart failure irrespective of left ventricular ejection fraction.
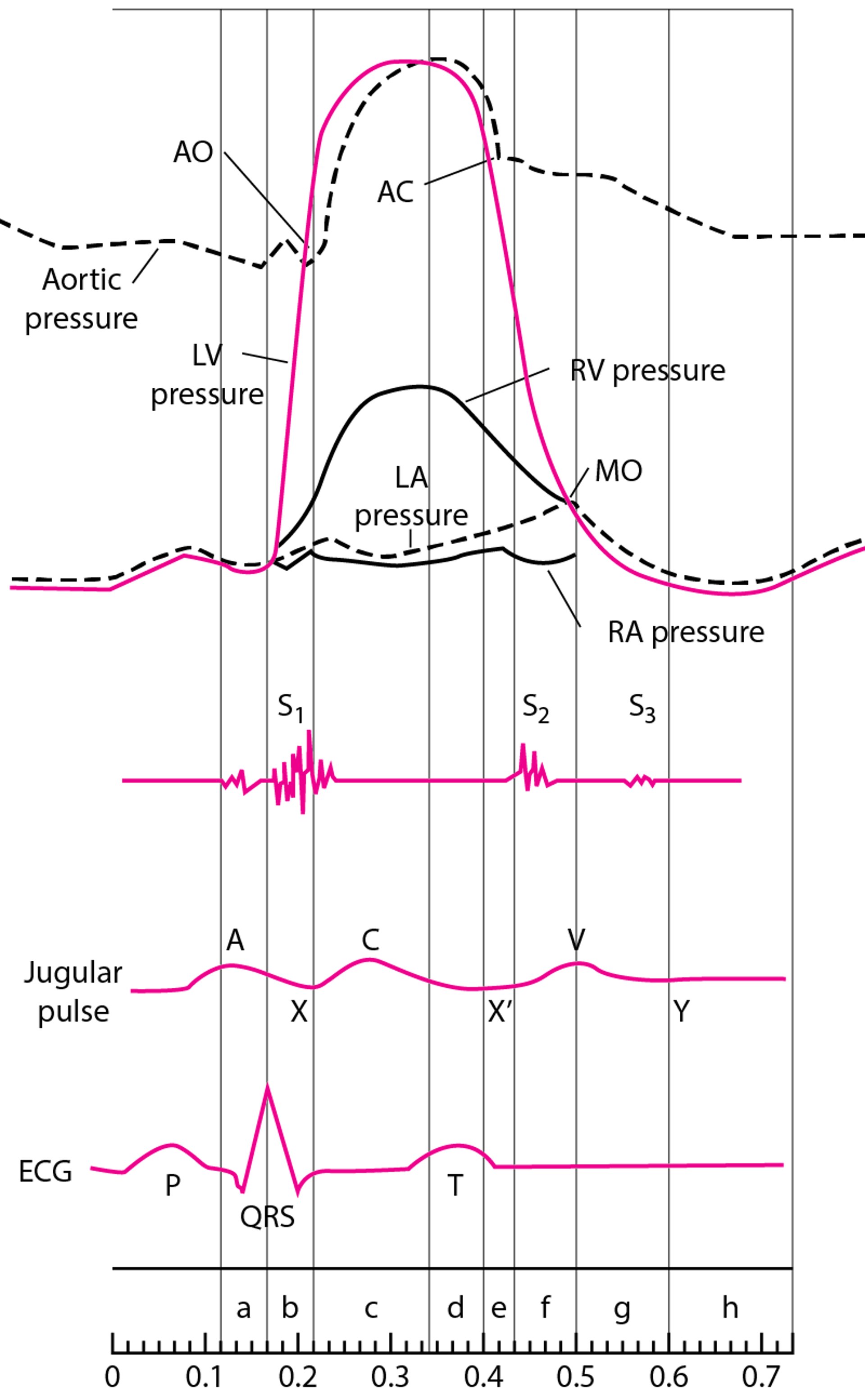
Diagram of the Cardiac Cycle, Showing Pressure Curves of the Cardiac Chambers, Heart Sounds, Jugular Pulse Wave, and the ECG
The phases of the cardiac cycle are atrial systole (a), isometric contraction (b), maximal ejection (c), reduced ejection (d), protodiastolic phase (e), isometric relaxation (f), rapid inflow (g), and diastasis, or slow LV filling (h). For illustrative purposes, time intervals between valvular events have been modified, and the z point has been prolonged. In the jugular venous pulse tracing, the A wave represents atrial contraction at end-diastole, C wave is the carotid artery impulse or bulging of the tricuspid valve into the right atrium in early systole, V wave is the increase in pressure and volume of right atrial filling in late systole and early diastole, X and X' descents represent movement of the lower part of the right atrium toward the ventricle with X' at end-systole, and the Y descent is tricuspid valve opening and ventricular filling in diastole. AO = aortic valve opening; AC = aortic valve closing; LV = left ventricle; LA = left atrium; RV = right ventricle; RA = right atrium; MO = mitral valve opening. |

Specific Tests During Cardiac Catheterization
Angiography
Injection of radiopaque contrast agent into coronary or pulmonary arteries, the aorta, and cardiac chambers is useful in certain circumstances. Digital subtraction angiography is used for nonmoving arteries and for chamber cineangiography.
Coronary angiography via left heart catheterization is used to evaluate coronary artery anatomy in various clinical situations, as in patients with suspected coronary atherosclerotic or congenital disease, valvular disorders before valvular replacement, or unexplained heart failure.

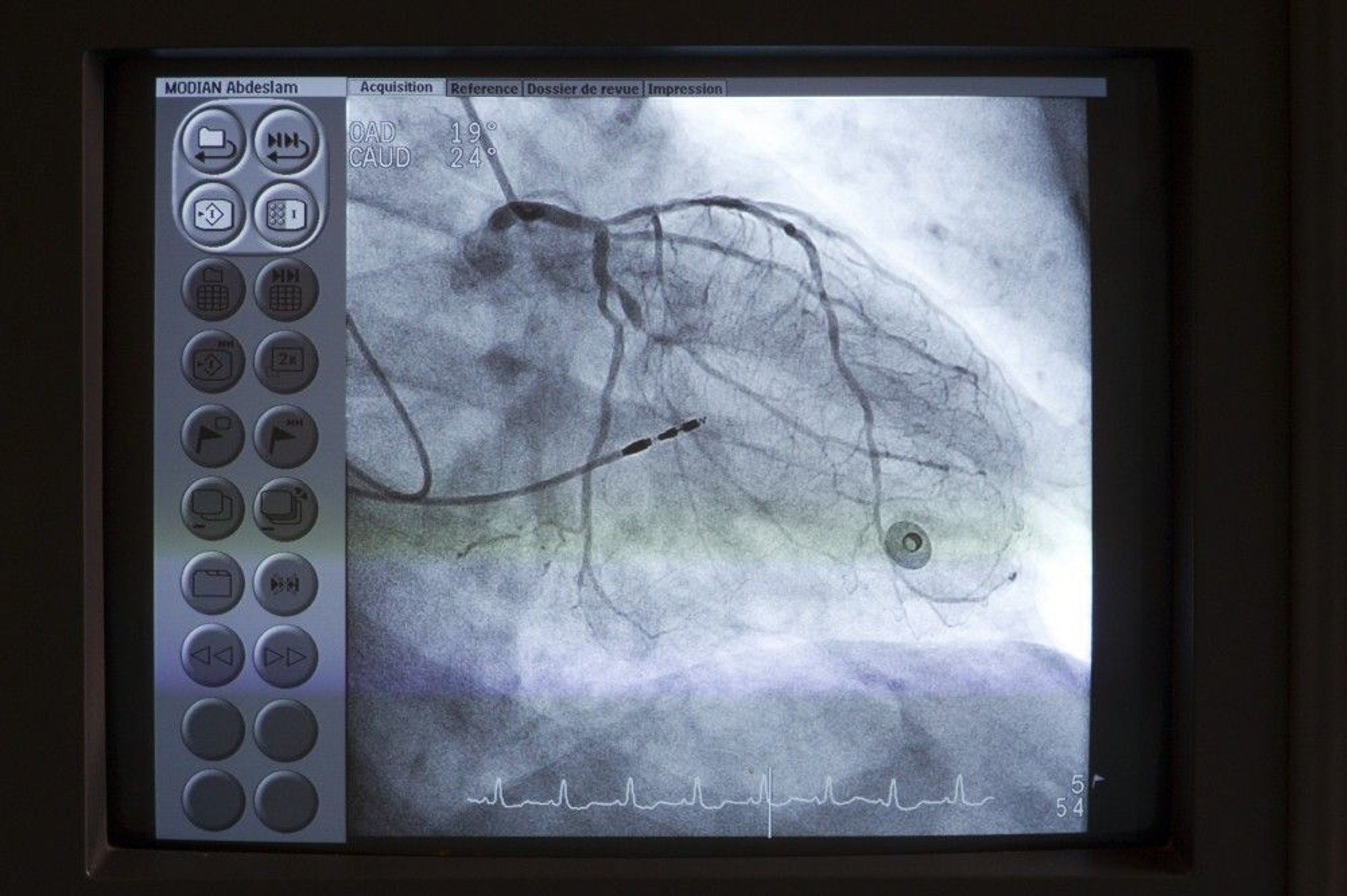
Astier/BSIP/SCIENCE PHOTO LIBRARY
Pulmonary angiography via right heart catheterization can be used to diagnose pulmonary embolism. Intraluminal filling defects or arterial cutoffs are diagnostic. Radiopaque contrast agent is usually selectively injected into one or both pulmonary arteries and their segments. Computed tomographic pulmonary angiography (CTPA) has largely replaced right heart catheterization for diagnosis of acute pulmonary embolism. Pulmonary angiography via right heart catheterization remains commonly used to determine a management plan for suspected chronic thromboembolic disease.
Aortic angiography via left heart catheterization is used to assess aortic regurgitation, coarctation, patent ductus arteriosus, and dissection.

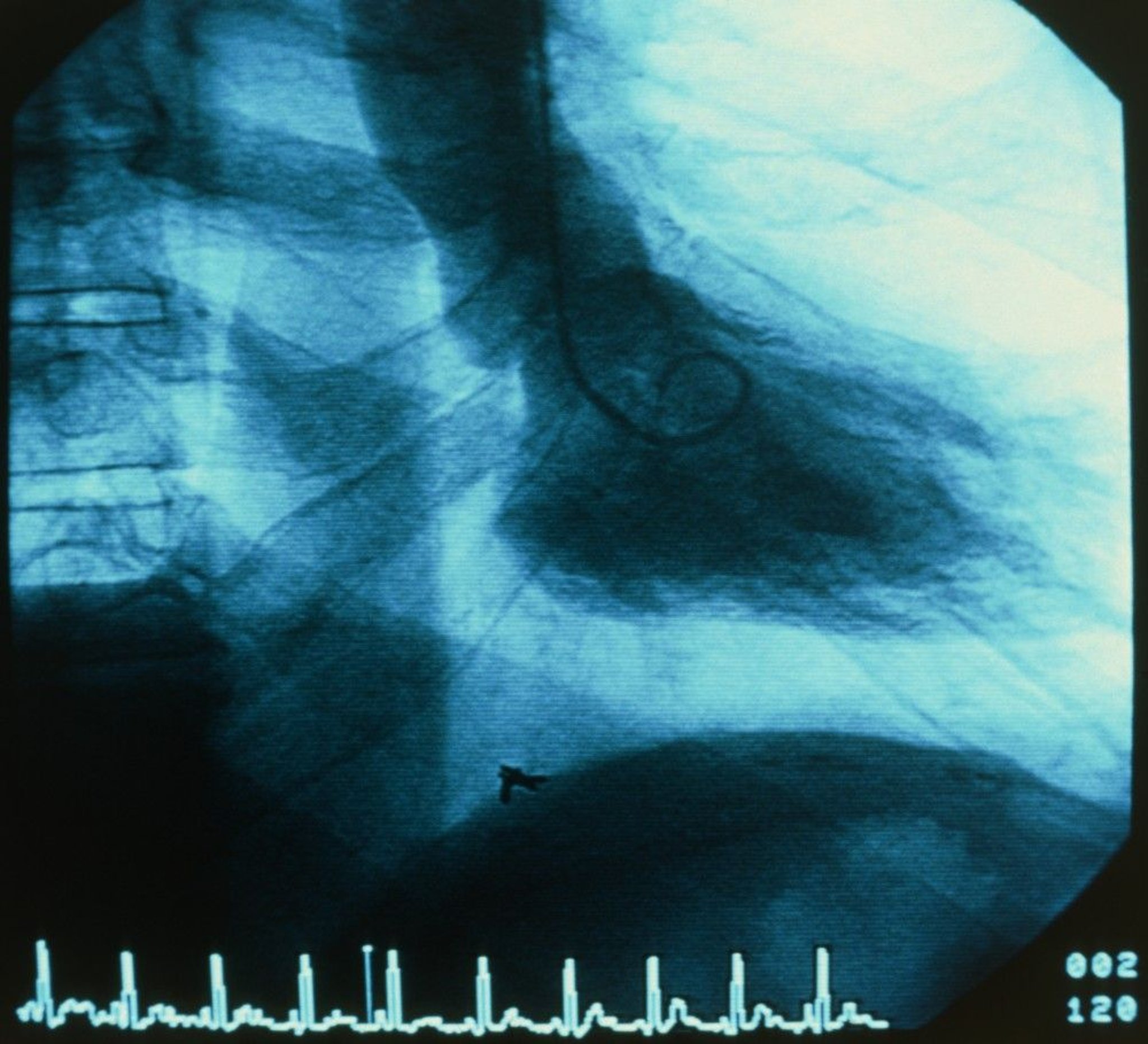
PETER MENZEL/SCIENCE PHOTO LIBRARY
Ventriculography is used to visualize ventricular wall motion and ventricular outflow tracts, including subvalvular, valvular, and supravalvular regions. It is also used to estimate severity of mitral valve regurgitation and determine its pathophysiology. After left ventricular mass and volume are determined from single planar or biplanar ventricular angiograms, end-systolic and end-diastolic volumes and ejection fraction can be calculated.
Coronary artery flow measurements
Coronary angiography shows the presence and degree of stenosis but not the functional significance of the lesion (ie, how much blood flows across the stenosis) or whether a specific lesion is likely to be the cause of symptoms.
Extremely thin guidewires with pressure sensors or Doppler flow sensors are available. Data from these sensors can be used to estimate coronary artery blood flow, which is expressed as fractional flow reserve (FFR). FFR is the ratio of maximal flow through the stenotic area to normal maximal flow obtained during hyperemia (most commonly with adenosine); an FFR of < 0.75 to 0.8 is considered abnormal. Newer techniques of measuring coronary blood flow, including instantaneous wave-free ratio (iFR) and diastolic hyperemia-free ratio (DFR), have been developed. These techniques have the advantage of not requiring hyperemia. Both iFR and DFR measure gradients across a stenosis during a period in diastole; an iFR or DFR of ≤ 0.89 is considered abnormal (1, 2).
These flow estimates correlate well with the need for intervention and long-term outcome; patients with lesions with FFR > 0.8, iFR > 0.89, or DFR > 0.89 do not seem to benefit from placement of a stent. These flow measurements are most useful with intermediate lesions (40 to 70% stenosis) and with multiple lesions (to identify those that are clinically most significant).
Intravascular ultrasonography (IVUS)
Miniature ultrasound transducers on the end of coronary artery catheters can produce images of coronary vessel lumina and walls and delineate blood flow. Intravascular ultrasonography is being increasingly used at the same time as coronary angiography in several clinical situations, including to guide optimal stent placement during percutaneous coronary intervention, detect cardiac allograft vasculopathy after heart transplantation, and identify coronary artery dissections.
Optical coherence tomography (OCT)
Optical coherence tomography is an optical analog of intracoronary ultrasound imaging that measures the amplitude of backscattered light to determine the temperature of coronary plaques and can help determine whether lesions are at high risk of future rupture (leading to acute coronary syndromes). Unlike in IVUS, injection of contrast is required to obtain images. The indications and appropriate use for OCT versus IVUS are currently uncertain.
Tests for cardiac shunts
Measuring blood oxygen content at successive levels in the heart and great vessels can help determine the presence, direction, and volume of central shunts. The maximal normal difference in oxygen content between structures is as follows:
The pulmonary artery and right ventricle: 0.5 mL/dL (0.5 vol%)
The right ventricle and right atrium: 0.9 mL/dL (0.9 vol%)
The right atrium and superior vena cava: 1.9 mL/dL (1.9 vol%)
If the blood oxygen content in a chamber exceeds that of the more proximal chamber by more than these values, a left-to-right shunt at that level is probable. Right-to-left shunts are strongly suspected when LA, LV, or arterial oxygen saturation is low (≤ 92%) and does not improve when pure oxygen (fractional inspirational O2 = 1.0) is given. Left heart or arterial desaturation plus increased oxygen content in blood samples drawn beyond the shunt site on the right side of circulation suggests a bidirectional shunt.
Measurement of cardiac output and flow
Cardiac output (CO) is the volume of blood ejected by the heart per minute (normal at rest: 4 to 8 L/minute). Techniques (see table Cardiac Output Equations) used to calculate CO include
Fick cardiac output technique
Indicator-dilution technique
Thermodilution technique
With the Fick technique, CO is proportional to oxygen consumption divided by arteriovenous oxygen difference.
Dilution techniques rely on the assumption that after an indicator is injected into the circulation, it appears and disappears proportionately to CO.
Usually, CO is expressed in relation to body surface area (BSA) as the cardiac index (CI) in L/minute/m2 (ie, CI = CO/BSA—see table Normal Values for Cardiac Index and Related Measures). BSA is calculated using DuBois height (ht)–weight (wt) equation:


Endomyocardial biopsy
Endomyocardial biopsy helps assess transplant rejection and myocardial disorders due to infection or infiltrative diseases. The biopsy catheter (bioptome) can be passed into either ventricle, usually the right. Three to 5 samples of myocardial tissue are removed from the septal endocardium. The main complication of endomyocardial biopsy, cardiac perforation, occurs in 0.3 to 0.5% of patients; it may cause hemopericardium leading to cardiac tamponade. Injury to the tricuspid valve and supporting chordae may also occur and can lead to tricuspid regurgitation.
Tests during cardiac catheterization references
1. Gotberg M, Christiansen EH, Gudmundsdottir IJ, et al: Instantaneous wave-free ratio versus fractional flow reserve to guide PCI. New Engl J Med 376:1813–1823, 2017. doi: 10.1056/NEJMoa1616540
2. Johnson NP, Li W, Chen X, et al: Diastolic pressure ratio: new approach and validation vs. the instantaneous wave-free ratio. Eur Heart J 40:2585–2594, 2019.
Contraindications to Cardiac Catheterization
Relative contraindications to cardiac catheterization include
Fever
Radiopaque contrast agent allergies in patients who have not been appropriately premedicated
Systemic infection
Uncontrolled arrhythmia
Uncontrolled hypertension
Uncompensated heart failure
Relative contraindications balance the urgency of the procedure (eg, in an acute myocardial infarction vs an elective case) and the severity of the contraindicating disorder. Periprocedural management of anticoagulants or antiplatelet drugs is individualized based on the type of procedure (ie, arterial vs venous access), the urgency of the procedure, the indication for the drug, and the patient's risk of bleeding. Catheterization laboratories frequently have policies for the periprocedural management of these drugs.
Complications of Cardiac Catheterization
The incidence of complications after cardiac catheterizations ranges from 0.8 to 8%, depending on patient factors, technical factors, and the experience of the operator. Patient factors that increase risk of complications include
Increasing age
Most complications are minor and can be easily treated. Serious complications (eg, cardiac arrest, anaphylactic reactions, shock, seizures, renal toxicity) are rare. Mortality rate is 0.1 to 0.2%. Myocardial infarction (0.1%) and stroke (0.1%) may result in significant morbidity. Incidence of stroke is higher in patients > 80 years.
In general, complications involve
The contrast agent
Effects of the catheter
The access site
Contrast agent complications
Injection of radiopaque contrast agent produces a transient sense of warmth throughout the body in many patients. Tachycardia, a slight fall in systemic pressure, an increase in cardiac output, nausea, vomiting, and coughing may occur. Rarely, bradycardia occurs when a large amount of a contrast agent is injected; asking the patient to cough often restores normal rhythm.
More serious reactions (see also Radiographic Contrast Agents and Contrast Reactions) include
Allergic-type contrast reactions
Contrast-induced kidney injury
Allergic-type reactionsAnaphylaxis and anaphylactoid reactions with bronchospasm, laryngeal edema, and dyspnea are rare reactions with an approximate frequency of about 1/5000 tests (1
Contrast-induced kidney injury is defined as impairment of renal function (either a 25% increase in serum creatinine from baseline or a 0.5 mg/dL [44 micromole/L] increase in absolute value) within 24 to 48 hours of IV contrast administration judged to be caused by contrast rather than alternative causes. For patients at risk, use of lowest possible dose of low-osmolar or iso-osmolar contrast, avoidance of multiple contrast studies within a short period of time, and infusion of a total 10 to 15 mL/kg normal saline IV beginning 4 to 6 hours before angiography and 6 to 12 hours afterward reduces this risk substantially. In patients at risk of impaired renal function, assess serum creatinine 48 hours after injection of contrast.
Contrast agent complications reference
1. Wang CL, Cohan RH, Ellis JH, et al: Frequency, outcome, and appropriateness of treatment of nonionic iodinated contrast media reactions. AJR Am J Roentgenol 191:409–415, 2008. doi: 10.2214/AJR.07.3421
Catheter-related complications
If the catheter tip contacts the ventricular endocardium, ventricular arrhythmias commonly occur, but ventricular fibrillation is rare. If it occurs, direct current cardioversion (DC cardioversion) is administered immediately.
Disruption of an atherosclerotic plaque by the catheter can release a shower of atheroemboli. Emboli from the aorta may cause stroke or nephropathy. Emboli from proximal to distal coronary arteries may cause myocardial infarction.
Coronary artery dissection is also possible.
Access site complications
Access site complications include
Bleeding
Hematoma
Pseudoaneurysm
Arteriovenous (AV) fistula
Limb ischemia
Bleeding from the access site may occur and usually resolves with compression. Mild bruises and small hematomas are common and do not require specific investigation or treatment.
A large or enlarging lump should be investigated using ultrasonography to distinguish hematoma from pseudoaneurysm. A bruit at the site (with or without pain) suggests an AV fistula, which can be diagnosed using ultrasonography. Hematomas usually resolve with time and do not require specific therapy. Pseudoaneurysms and AV fistulas usually resolve with compression; those that persist may require surgical repair.
Radial artery access is in general more comfortable for the patient and carries a much lower risk of hematoma or pseudoaneurysm or AV fistula formation when compared with femoral artery access.
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
ACR Manual on Contrast Media: 2021 ACR Committee on Drugs and Contrast Media provides a guide for safe and effective use of contrast media
Bashore TM, Balter S, Barac A, et al. 2012 American College of Cardiology Foundation/Society for Cardiovascular Angiography and Interventions expert consensus document on cardiac catheterization laboratory standards update: A report of the American College of Cardiology Foundation Task Force on Expert Consensus documents developed in collaboration with the Society of Thoracic Surgeons and Society for Vascular Medicine. J Am Coll Cardiol. 2012;59(24):2221-2305. doi:10.1016/j.jacc.2012.02.010
2012 American College of Cardiology Foundation/Society for Cardiovascular Angiography and Interventions expert consensus document on cardiac catheterization laboratory standards update: A report of the American College of Cardiology Foundation Task Force on Expert Consensus documents developed in collaboration with the Society of Thoracic Surgeons and Society for Vascular Medicine: Provides the most recent consensus opinions on standards for cardiac catheterization labs






