Abscesses can occur anywhere in the abdomen and retroperitoneum. They mainly occur after surgery, trauma, or conditions involving abdominal infection and inflammation, particularly when peritonitis or perforation occurs. Symptoms are malaise, fever, and abdominal pain. Diagnosis is by CT. Treatment is with drainage, either surgical or percutaneous. Antibiotics are ancillary.
(See also Acute Abdominal Pain.)
Etiology of Intra-Abdominal Abscesses
Intra-abdominal abscesses are classified as intraperitoneal, retroperitoneal, or visceral (see table Intra-Abdominal Abscesses).
Many intra-abdominal abscesses develop after perforation of a hollow viscus or colonic cancer. Others develop by extension of infection or inflammation resulting from conditions such as appendicitis, diverticulitis, Crohn disease, pancreatitis, pelvic inflammatory disease, or indeed any condition causing generalized peritonitis.
Abdominal surgery, particularly that involving the digestive or biliary tract, is a significant risk factor: The peritoneum may be contaminated during or after surgery by events such as anastomotic leaks. Traumatic abdominal injuries—particularly lacerations and hematomas of the liver, pancreas, spleen, and intestines—may develop abscesses, whether treated operatively or not.
The infecting organisms typically reflect normal bowel flora and are a complex mixture of anaerobic and aerobic bacteria. Most frequent isolates are
Aerobic gram-negative bacilli (eg, Escherichia coli and Klebsiella)
Anaerobes (especially Bacteroides fragilis)
Intra-Abdominal Abscesses
Location | Etiology | Organisms |
|---|---|---|
Intraperitoneal | ||
Subphrenic Right or left lower quadrant Interloop Paracolic Pelvic | Postoperative; perforation of hollow viscus, appendicitis, diverticulitis, or tumor; Crohn disease; pelvic inflammatory disease; generalized peritonitis of any etiology | Bowel flora, often polymicrobial |
Retroperitoneal | ||
Pancreatic | Trauma, pancreatitis | Bowel flora, often polymicrobial |
Perinephric | Spread of renal parenchymal abscess (complication of pyelonephritis or rarely hematogenous from a remote source) | Aerobic gram-negative bacilli |
Visceral | ||
Hepatic | Trauma, ascending cholangitis, portal bacteremia | Aerobic gram-negative bacilli if origin is biliary Polymicrobial bowel flora Amebic infection via the portal venous system |
Splenic | Trauma, hematogenous, infarction (as in sickle cell disease and malaria) | Staphylococci, streptococci, anaerobes, aerobic gram-negative bacilli including Salmonella Candida in patients with immunocompromise |
Symptoms and Signs of Intra-Abdominal Abscesses
Abscesses may form within 1 week of perforation or significant peritonitis, whereas postoperative abscesses may not occur until 2 to 3 weeks after operation and, rarely, not for several months. Although manifestations vary, most abscesses cause fever and abdominal discomfort ranging from minimal to severe (usually near the abscess). Paralytic ileus, either generalized or localized, may develop. Nausea, anorexia, and weight loss are common.
Abscesses in the Douglas cul-de-sac, adjacent to the rectosigmoid junction, may cause diarrhea. Contiguity to the bladder may result in urinary urgency and frequency and, if caused by diverticulitis, may create a colovesical fistula.
Subphrenic abscesses may cause chest symptoms such as nonproductive cough, chest pain, dyspnea, hiccups, and shoulder pain. Rales, rhonchi, or a friction rub may be audible. Dullness to percussion and decreased breath sounds are typical when basilar atelectasis, pneumonia, or pleural effusion occurs.
Generally, there is tenderness over the location of the abscess. Large abscesses may be palpable as a mass.
Complications of intra-abdominal abscesses
Undrained abscesses may extend to contiguous structures, erode into adjacent vessels (causing hemorrhage or thrombosis), rupture into the peritoneum or bowel, or form a cutaneous or genitourinary fistula.
Subdiaphragmatic abscesses may extend into the thoracic cavity, causing an empyema, lung abscess, or pneumonia.
An abscess in the lower abdomen may track down into the thigh or perirectal fossa.
Splenic abscess is a rare cause of sustained bacteremia in endocarditis that persists despite appropriate antimicrobial therapy.
Diagnosis of Intra-Abdominal Abscesses
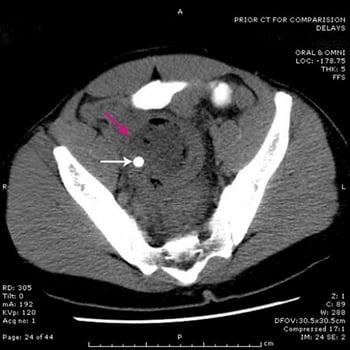
Abdominal CT
Rarely radionuclide scanning
CT of the abdomen and pelvis with oral contrast is the preferred diagnostic modality for suspected abscess.
Other imaging studies, if done, may show abnormalities; plain abdominal x-rays may reveal extraintestinal gas in the abscess, displacement of adjacent organs, a soft-tissue density representing the abscess, or loss of the psoas muscle shadow. Abscesses near the diaphragm may result in chest x-ray abnormalities such as ipsilateral pleural effusion, elevated or immobile hemidiaphragm, lower lobe infiltrates, and atelectasis.
A complete blood count and blood cultures should be done. Leukocytosis occurs in most patients, and anemia is common.

Occasionally, radionuclide scanning with indium-111–labeled leukocytes may be helpful in identifying intra-abdominal abscesses.
Treatment of Intra-Abdominal Abscesses
IV antibiotics
Drainage: Percutaneous or surgical
Almost all intra-abdominal abscesses require drainage, either by percutaneous catheters or surgery. Exceptions to drainage include small (< 2 cm) pericolic or periappendiceal abscesses, or abscesses that are draining spontaneously to the skin or into the bowel. Drainage through catheters (placed with CT or ultrasound guidance) may be appropriate given the following conditions:
Few abscess cavities are present.
The drainage route does not traverse bowel or uncontaminated organs, pleura, or peritoneum.
The source of contamination is controlled.
The pus is thin enough to pass through the catheter.
Antibiotics are not curative but may limit hematogenous spread and should be given before and after intervention. Therapy requires IV antibiotics active against bowel flora.
Patients with community-acquired infection should be characterized as at low or high risk of treatment failure or death based on signs of sepsis or septic shockmetronidazolePseudomonas) and anaerobes. (See also the Surgical Infection Society's 2017 revised guidelines on the management of intra-abdominal infection.)
Nutritional support is important, with the enteral route preferred. Parenteral nutrition should begin early if the enteral route is not feasible.
Prognosis for Intra-Abdominal Abscesses
Complicated intra-abdominal abscesses (those extending beyond a single organ into the peritoneal space) have a mortality rate of 10 to 40%. Outcome depends mainly on the presence of sepsis and on the patient’s primary illness or injury and general medical condition rather than on the specific nature and location of the abscess.
Key Points
Suspect abdominal abscess in patients with a previous causative event (eg, abdominal trauma, abdominal surgery) or condition (eg, Crohn disease, diverticulitis, pancreatitis) who develop abdominal pain and fever.
Abscess may be the first manifestation of a cancer.
Diagnosis is with abdominal CT.
Treatment is percutaneous or surgical drainage; antibiotics are necessary but alone are not adequate treatment.
More Information
The following English-language resource may be useful. Please note that THE MANUAL is not responsible for the content of this resource.
Surgical Infection Society: Revised Guidelines on the Management of Intra-Abdominal Infection (2017)
Sartelli M, Coccolini F, Kluger Y, et al: WSES/GAIS/SIS-E/WSIS/AAST global clinical pathways for patients with intra-abdominal infections. World J Emerg Surg 16(1):49, 2021. doi: 10.1186/s13017-021-00387-8