Central retinal artery occlusion occurs when the central retinal artery becomes blocked, usually due to an embolus. It causes sudden, painless, unilateral, and usually severe vision loss. Diagnosis is by history and characteristic retinal findings on funduscopy. Intraocular pressure can be decreased within the first 24 hours of occlusion to attempt to dislodge the embolus. If patients present within the first few hours of occlusion, some centers catheterize the carotid/ophthalmic artery and selectively inject thrombolytic drugs.
Etiology
Retinal artery occlusion may be due to embolism or thrombosis.
Emboli may come from any of the following:
Atherosclerotic plaques
Fat
Atrial myxoma
Thrombosis is a less common cause of retinal artery occlusion but can be seen with systemic vasculitis such as systemic lupus erythematosus (SLE) and giant cell arteritis, which is an important cause of arterial occlusion that requires prompt diagnosis and treatment.
Occlusion can affect a branch of the retinal artery as well as the central retinal artery.
Neovascularization (abnormal new vessel formation) of the retina or iris (rubeosis iridis) with secondary (neovascular) glaucoma occurs in about 20% of patients within weeks to months after occlusion. Vitreous hemorrhage may result from retinal neovascularization.
Risk of stroke is increased after retinal artery occlusion, particularly in the first weeks.
Symptoms and Signs
Retinal artery occlusion causes sudden, painless, severe vision loss or visual field defect, usually unilaterally.
The pupil may respond poorly to direct light but constricts briskly when the other eye is illuminated (relative afferent pupillary defect). In acute cases, funduscopy shows a pale, opaque fundus with a red fovea (cherry-red spot). Typically, the arteries are attenuated and may even appear bloodless. An embolus (eg, a cholesterol embolus, called a Hollenhorst plaque) is sometimes visible. If a major branch is occluded rather than the entire artery, fundus abnormalities and vision loss are limited to that sector of the retina.
Patients who have giant cell arteritis are 55 or older and may have a headache, a tender and palpable temporal artery, jaw claudication, fatigue, or a combination.
Diagnosis
Clinical evaluation

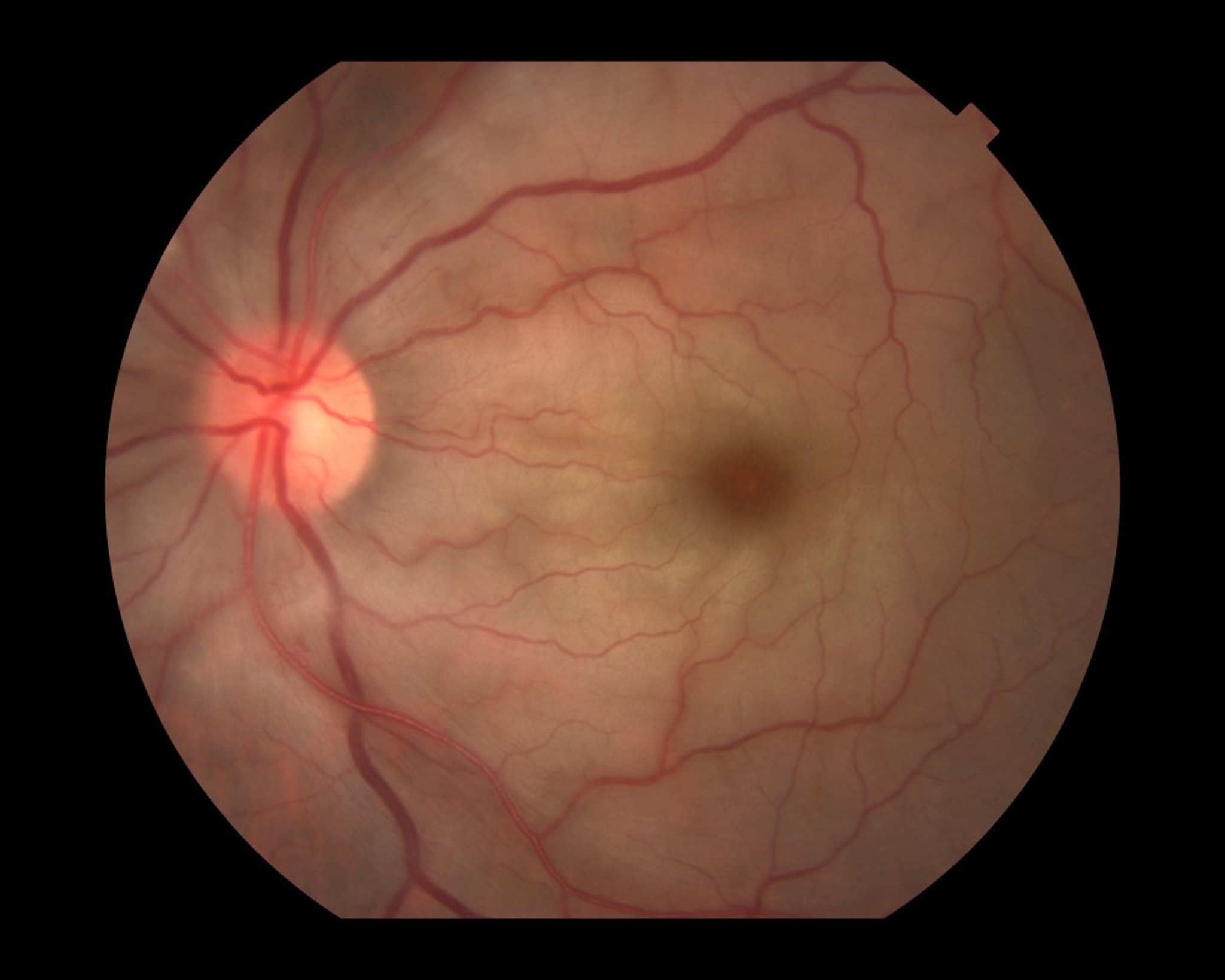
Paul Whitten/SCIENCE PHOTO LIBRARY
Once the diagnosis is made, carotid Doppler ultrasonography and echocardiography should be done to identify an embolic source so that further embolization can be prevented.
If giant cell arteritis is suspected, erythrocyte sedimentation rate (ESR), C-reactive protein, and platelet count should be done immediately. These tests may not be necessary if an embolic plaque is visible in the central retinal artery.
Because risk of stroke is increased, some centers rapidly evaluate patients similarly to those who have had stroke or transient ischemic attack.
Prognosis
Patients with a branch artery occlusion may maintain good to fair vision, but with central artery occlusion, vision loss is often profound, even with treatment. Once retinal infarction occurs (as quickly as 90 minutes after the occlusion), vision loss is permanent.
If underlying giant cell arteritis is diagnosed and treated promptly, the vision in the uninvolved eye can often be protected and some vision may be recovered in the affected eye.
Treatment
Reduction of intraocular pressure
Pearls & Pitfalls
|
If acute thromboembolism is suspected, the patient should be referred immediately to a specialized stroke center because there is an increased risk of other cerebrovascular events.
Patients with occlusion secondary to giant cell arteritis should receive high-dose systemic corticosteroids.
Key Points
Central or branch retinal artery occlusion can be caused by an embolus (eg, due to atherosclerosis or endocarditis), thrombosis, or giant cell arteritis.
Painless, severe loss of vision affects part or all of the visual field.
Confirm the diagnosis by doing funduscopy (typically showing a pale, opaque fundus with a red fovea and arterial attenuation).
Immediately refer patients with acute thromboembolic events to a specialized stroke center.