Pityriasis rosea is a self-limited, inflammatory disease characterized by diffuse, scaling papules or plaques. Diagnosis is clinical. Treatment is usually unnecessary.
Pityriasis rosea most commonly occurs between ages 10 and 35. It affects women more often.
The cause of pityriasis rosea may be viral infection (some research has implicated human herpesviruses 6, 7, and 8) (1, 2). Some medications (eg, ACE inhibitors, hydrochlorothiazide, captopril, barbiturates, metronidazole, allopurinol), may cause a pityriasis rosea–like reaction.
References
1. Mubki TF, Bin Dayel SA, Kadry R: A case of pityriasis rosea concurrent with the novel influenza A (H1N1) infection. Pediatr Dermatol 28(3):341-342, 2011. doi: 10.1111/j.1525-1470.2010.01090.x
2. Prantsidis A, Rigopoulos D, Papatheodorou G, et al: Detection of human herpesvirus 8 in the skin of patients with pityriasis rosea. Acta Derm Venereol 89(6):604-606, 2009. doi: 10.2340/00015555-0703
Symptoms and Signs of Pityriasis Rosea
The condition classically begins with a single, primary, 2- to 10-cm herald patch that appears on the trunk or proximal limbs. A general centripetal eruption of 0.5- to 2-cm rose- or fawn-colored oval papules and plaques follows within 7 to 14 days. The lesions have a scaly, slightly raised border (collarette) and resemble ringworm (tinea corporis).
The rose or fawn color is not as evident in patients with dark skin. Patches that appear more pink in patients with light skin appear violaceous and/or hyperpigmented in patients with dark skin.
Most patients itch, occasionally severely. Papules may dominate with little or no scaling in children and pregnant women. Children more commonly have inverse pityriasis rosea (lesions in the axillae or groin that spread centrifugally).

Image courtesy of the Public Health Image Library of the Centers for Disease Control and Prevention.

Image provided by Thomas Habif, MD.
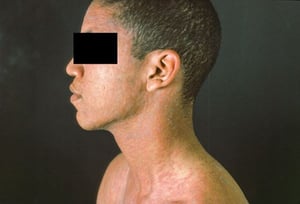
Image courtesy of Karen McKoy, MD.

Image courtesy of Karen McKoy, MD.

Image provided by E. Laurie Tolman, MD.


Image courtesy of the Public Health Image Library of the Centers for Disease Control and Prevention.


Image provided by Thomas Habif, MD.

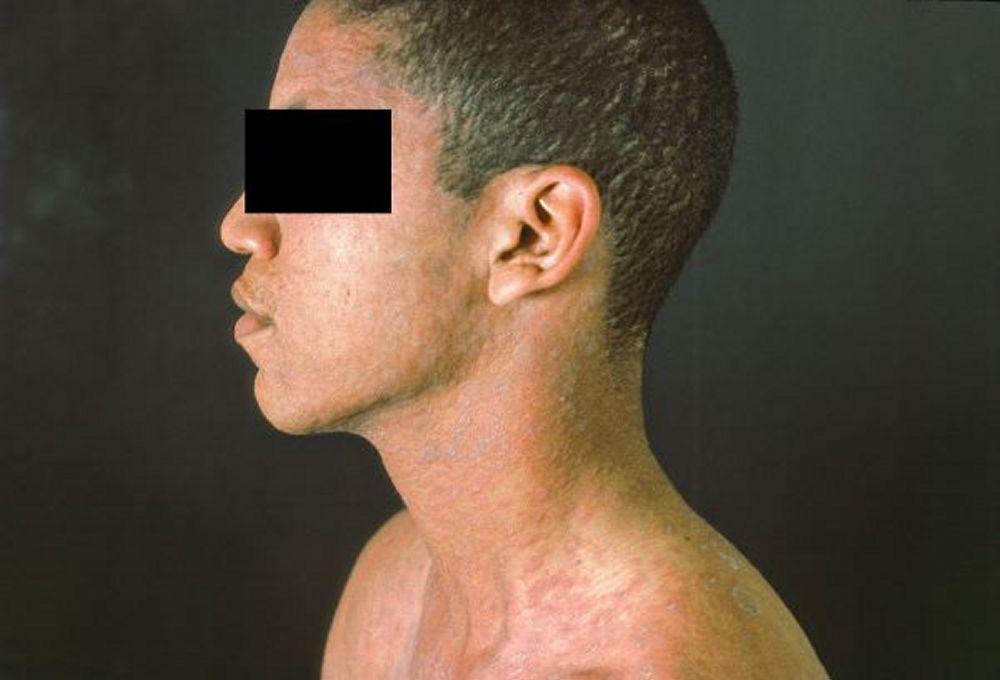
Image courtesy of Karen McKoy, MD.


Image courtesy of Karen McKoy, MD.


Image provided by E. Laurie Tolman, MD.
Classically, lesions orient along skin lines, giving pityriasis rosea a Christmas tree–like distribution when multiple lesions appear on the back.
A prodrome of malaise, headache, and sometimes arthralgia precedes the lesions in a minority of patients.
Diagnosis of Pityriasis Rosea
Clinical evaluation
Diagnosis of pityriasis rosea is based on clinical appearance and distribution.
Differential diagnosis includes
Pityriasis lichenoides chronica
Serologic testing for syphilis is indicated when the palms or soles are affected, when a herald patch is not seen, or when lesions occur in an unusual sequence or distribution.
Treatment of Pityriasis Rosea
Antipruritic therapy
No specific treatment is necessary because the eruption usually remits within 5 weeks and recurrence is rare.
Artificial or natural sunlight may hasten resolution.
Antipruritic therapy such as topical corticosteroids, oral antihistamines, or topical measures may be used as needed.
Treatment references
1. Contreras-Ruiz J, Peternel S, Jiménez Gutiérrez C, et al: Interventions for pityriasis rosea. Cochrane Database Syst Rev 2019(10):CD005068, 2019. doi: 10.1002/14651858.CD005068.pub3
2. Stashower J, Bruch K, Mosby A, et al: Pregnancy complications associated with pityriasis rosea: A multicenter retrospective study. J Am Acad Dermatol 85(6):1648-1649, 2021. doi: 10.1016/j.jaad.2020.12.063
Key Points
Pityriasis rosea is a self-limited, inflammatory disorder of the skin possibly caused by human herpesvirus types 6, 7, or 8 or medications.
An initial 2- to 10-cm herald patch is followed by centripetal eruption of oval papules and plaques with a slightly raised and scaly border, typically appearing along skin lines.
Diagnose based on clinical appearance and distribution.
Treat with antipruritic medications as needed and possibly topical corticosteroids and/or sunlight.
Pityriasis rosea during the first 15 weeks of pregnancy is associated with premature birth or fetal demise.
Pregnant women should be offered antiviral therapy, even though this has not proved to reduce obstetric complications.