




Pulmonary embolism (PE) is the occlusion of pulmonary arteries by thrombi that originate elsewhere, typically in the large veins of the legs or pelvis. Risk factors for pulmonary embolism are conditions that impair venous return, conditions that cause endothelial injury or dysfunction, and underlying hypercoagulable states. Symptoms of pulmonary embolism are nonspecific and include dyspnea, pleuritic chest pain, and, in more severe cases, light-headedness, presyncope, syncope, or cardiorespiratory arrest. Signs are also nonspecific and may include tachypnea, tachycardia, and in more severe cases, hypotension. Diagnosis of pulmonary embolism is most commonly accomplished with CT angiography, although ventilation perfusion scanning is sometimes required. Pulmonary embolism treatment is with anticoagulants and, sometimes, clot dissolution with systemic or catheter-directed thrombolysis or by removal of the clot via catheter suction thrombectomy or surgical resection. When anticoagulation is contraindicated, an inferior vena caval (IVC) filter can be considered until anticoagulation is resumed. Preventive measures include early mobilization, anticoagulants, and, in patients who are hospitalized, sometimes mechanical compression devices that are applied to the legs.
(See also European Society of Cardiology 2019 Guidelines on Diagnosis and Management of Pulmonary Embolism and American Society of Hematology 2020 guidelines for management of venous thromboembolism: treatment of deep vein thrombosis and pulmonary embolism.)
The estimated annual incidence of pulmonary embolism world wide is approximately 1 per 1000 people (1). Up to 20% of people diagnosed with acute PE die in the next 90 days (2). However, the cause of death is usually not the PE itself but the underlying condition increasing the patients risk for PE. From 30 to 50% of patients who have a PE describe functional and exercise limitations up to a year after the event, which is referred to as the post PE syndrome (3).
General references
1. Kahn SR, de Wit K. Pulmonary Embolism. N Engl J Med 2022;387(1):45-57. doi:10.1056/NEJMcp2116489
2. Lehnert P, Lange T, Møller CH, Olsen PS, Carlsen J. Acute Pulmonary Embolism in a National Danish Cohort: Increasing Incidence and Decreasing Mortality. Thromb Haemost 2018;118(3):539-546. doi:10.1160/TH17-08-0531
3. Kahn SR, Hirsch AM, Akaberi A, et al. Functional and Exercise Limitations After a First Episode of Pulmonary Embolism: Results of the ELOPE Prospective Cohort Study. Chest 2017;151(5):1058-1068. doi:10.1016/j.chest.2016.11.030
Etiology of Pulmonary Embolism
Nearly all pulmonary emboli arise from thrombi in the veins of the legs or pelvis (deep venous thrombosis). Risk of embolization is higher with thrombi that reach the popliteal vein or above. Thromboemboli can also originate in arm veins or central veins of the chest (caused by central venous catheters or resulting from thoracic outlet syndromes).
Pulmonary embolism can also arise from nonthrombotic sources (eg, embolism of air, amniotic fluid, fat, infected material, orthopedic cement, foreign body, tumor).
Risk factors for deep venous thrombosis and pulmonary embolism (see table Risk Factors for Deep Venous Thrombosis and Pulmonary Embolism) are similar in children and adults and include
Conditions that impair venous return, including bed rest and confinement without walking
Conditions that cause endothelial injury or dysfunction such as trauma or surgery
Underlying hypercoagulable (thrombophilic) disorders such as cancer or primary clotting disorders
COVID-19 appears to be a risk factor for deep venous thrombosis and pulmonary embolism. Although part of the risk may be due to reduced mobility associated with illness, it is thought that SARS-CoV-2 infection is prothrombotic.
Pathophysiology of Pulmonary Embolism
Once deep venous thrombosis develops, clots may dislodge and travel through the venous system and the right side of the heart to lodge in the pulmonary arteries, where they partially or completely occlude one or more vessels. The consequences depend on the size and number of emboli, the underlying condition of the lungs, how well the right ventricle (RV) is functioning, and the ability of the body’s intrinsic thrombolytic system to dissolve the clots. Death, when is does occur, is often due to right ventricular failure.
Small emboli may have no acute physiologic effects and may begin to lyse immediately and resolve within hours or days. Larger emboli can cause a reflex increase in ventilation (tachypnea), hypoxemia due to ventilation/perfusion (V/Q) mismatch, low mixed venous oxygen content as a result of low cardiac output, atelectasis due to alveolar hypocapnia and abnormalities in surfactant, and an increase in pulmonary vascular resistance caused by mechanical obstruction and vasoconstriction resulting in tachycardia and hypotension. Endogenous lysis reduces most emboli, even those of moderate size, and physiologic alterations decrease over hours or days. Some emboli resist lysis and may organize and persist and sometimes cause chronic thromboembolic pulmonary hypertension (CTEPH).
Pulmonary emboli may be classified according to the physiologic effects as described by the European Society of Cardiology/American Heart Association (1) into the following:
High risk (massive): Impaired right ventricular function causing hypotension, as defined by systolic blood pressure < 90 mm Hg or a drop in systolic blood pressure of ≥ 40 mm Hg from baseline for a period of 15 minutes
Intermediate risk (submassive): Impaired right ventricular function without hypotension. This is evidenced by right ventricular enlargement and/or hypokinesis on imaging (eg, CT angiography, echocardiography) as well as by increases in circulating biomarkers (eg, troponin, brain natriuretic peptide). Note that the European Society of Cardiology defines intermediate-risk pulmonary embolism also as patients with a simplified pulmonary embolism severity index (sPESI) of > 0, thus including patients with other disorders or findings (1). Intermediate-risk pulmonary embolism can be further divided into intermediate high risk (the presence of right ventricular dysfunction by imaging and elevated circulating biomarkers) versus intermediate low risk (the presence of right ventricular dysfunction by imaging or circulating biomarker elevation).
Low risk: Absence of right ventricular impairment and absence of hypotension (and by European Society of Cardiology, sPESI score = 0)
Saddle pulmonary embolism describes a pulmonary embolus that lodges in the bifurcation of the main pulmonary artery and into the right and left pulmonary arteries; saddle emboli are usually, but not always, intermediate risk or high risk. A saddle configuration does not dictate a specific therapeutic approach. Although saddle emboli are often large, causing near-complete or complete obstruction, they may also be a relatively thin, nonobstructive embolus.
In 1 to 3% of cases, chronic residual obstruction leads to pulmonary hypertension (chronic thromboembolic pulmonary hypertension) that evolves over months to years and can result in chronic right heart failure.
When a large embolus acutely occludes major pulmonary arteries or when many smaller emboli combine to occlude a significant proportion of the more distal vessels, RV pressure increases, which may lead to acute RV failure, shock, or sudden death. The risk of death depends on the degree and rate of rise of right-sided pressures and on the patient’s underlying cardiopulmonary status. Patients with preexisting cardiopulmonary disease are at higher risk of death, but young and/or otherwise healthy patients may survive a PE that occludes > 50% of the pulmonary bed.
Pulmonary infarction (interruption of pulmonary artery blood flow leading to ischemia of lung tissue, sometimes represented by a pleural-based [peripherally located], often wedge-shaped pattern on chest x-ray [Hampton hump] or other imaging modalities) occurs in < 10% of patients diagnosed with PE. This low rate has been attributed to the dual blood supply to the lung (ie, bronchial and pulmonary). Generally, pulmonary infarction is due to smaller emboli that become lodged in more distal pulmonary arteries and is nearly always completely reversible; pulmonary infarction is recognized early, often before necrosis occurs.
Pathophysiology reference
1. Konstantinides SV, Meyer G, Becattini C, et al: 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur Heart J 2020;41(4):543-603. doi:10.1093/eurheartj/ehz405
Symptoms and Signs of Pulmonary Embolism
Many pulmonary emboli are small, physiologically insignificant, and asymptomatic. Even when present, symptoms are nonspecific and vary in frequency and intensity, depending on the extent of pulmonary vascular occlusion and preexisting cardiopulmonary function.
Emboli often cause
Acute dyspnea
Pleuritic chest pain (when there is pulmonary infarction)
Dyspnea may be minimal at rest and can worsen during activity.
Less common symptoms include
Cough (usually caused by comorbid disorders or by dilation of the pulmonary arteries)
Hemoptysis (occasionally occurs when there is pulmonary infarction)
In older patients, the first symptom may be altered mental status.
Massive pulmonary emboli may manifest with hypotension, tachycardia, light-headedness/presyncope, syncope, or cardiac arrest.
The most common signs of pulmonary embolism are
Tachycardia
Tachypnea
Less commonly, patients have hypotension.
A loud 2nd heart sound (S2) due to a loud pulmonic component (P2) is possible but uncommon in acute PE because increases in pulmonary artery pressures are only modest. Crackles or wheezing may occur, but these sounds are usually due to comorbid disease. In the presence of right ventricular failure, distended internal jugular veins and a RV heave may be evident, and a RV gallop (3rd heart sound [S3]), with or without tricuspid regurgitation, may be audible.
Fever, when present, is usually low-grade unless caused by an underlying condition.
Pulmonary infarction is typically characterized by chest pain (mainly pleuritic) and, occasionally, hemoptysis. The chest wall may be tender.
Chronic thromboembolic pulmonary hypertension causes symptoms and signs of right heart failure, including exertional dyspnea, easy fatigue, and peripheral edema that develops over months to years.
Patients with acute pulmonary embolism may also have symptoms of deep venous thrombosis (ie, pain, swelling, and/or erythema of a leg or an arm). Such leg symptoms are often not present, however.
Diagnosis of Pulmonary Embolism
High index of suspicion
Assessment of pretest probability (based on clinical findings, including pulse oximetry and chest x-ray)
Subsequent testing based on pretest probability
The diagnosis of pulmonary embolism is challenging because symptoms and signs are nonspecific and diagnostic tests are not 100% sensitive and specific. It is important to include PE in the differential diagnosis when nonspecific symptoms, such as dyspnea, pleuritic chest pain, hemoptysis, light-headedness, or syncope are encountered. Thus, PE should be considered in the differential diagnosis of patients suspected of having
Acute chest syndrome (in patients with sickle cell disease)
Acute anxiety with hyperventilation
Significant, unexplained tachycardia may be a clue. Pulmonary embolism also should be considered in any older patient with tachypnea and altered mental status.
Initial evaluation should include pulse oximetry and chest x-ray. Electrocardiography (ECG), arterial blood gas (ABG) measurements, or both may help to exclude other diagnoses (eg, acute myocardial infarction).
The chest x-ray usually is nonspecific but may show atelectasis, focal infiltrates, an elevated hemidiaphragm, or a pleural effusion. The classic findings of focal loss of vascular markings (Westermark sign), a peripheral, wedge-shaped density arising from the pleura (Hampton hump), or enlargement of the right descending pulmonary artery are suggestive but uncommon (ie, insensitive) and have low specificity. Chest x-ray can also help exclude pneumonia. Pulmonary infarction due to pulmonary embolism may be mistaken for pneumonia.
Pulse oximetry provides a quick way to assess oxygenation; hypoxemia is one sign of PE, and it requires further evaluation. Blood gas testing should be considered, particularly for patients with dyspnea or tachypnea who do not have hypoxemia detected with pulse oximetry. Arterial blood gas measurement may show an increased alveolar to arterial oxygen (A-a) difference (sometimes called A-a gradient) or hypocapnia. Pulse oximetry and blood gas testing are moderately sensitive for PE, but neither is specific. Oxygen saturation may be normal due to a small clot burden, or to compensatory hyperventilation; a very low partial pressure of carbon dioxide (PCO2) detected with an arterial blood gas measurement can confirm hyperventilation.
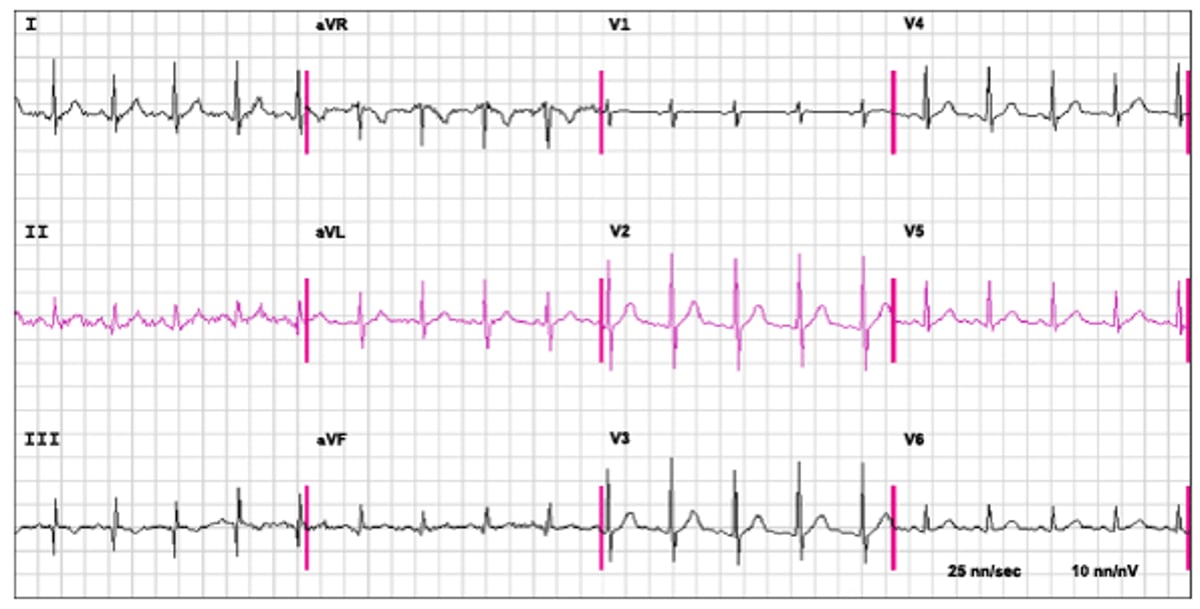
ECG most often shows tachycardia and various ST-T wave abnormalities, which are not specific for pulmonary embolism (see figure An ECG in Pulmonary Embolism). An S1Q3T3 (S wave in lead I, Q wave in lead III, inverted T wave in lead III) or a new right bundle branch block may indicate the effect of abrupt rise in RV size affecting RV conduction pathways; these findings are moderately specific but insensitive, occurring in only about 5% of patients, although the findings occur in a higher percentage of patients with massive PE. Right axis deviation (R > S in V1) and P-pulmonale may be present. T-wave inversion in leads V1 to V4 also occurs.
An ECG in Pulmonary Embolism
The ECG shows sinus tachycardia at a rate of 110 beats/minute, an S1Q3T3 and R = S in V1 in a patient with proven acute pulmonary embolism. |

Clinical probability
Clinical probability of pulmonary embolism can be assessed by combining ECG and chest x-ray findings with findings from the history and physical examination. Clinical prediction scores, such as the Wells score or the revised Geneva score (1), or the Pulmonary Embolism Rule-Out Criteria (PERC) rule, may aid clinicians in assessing the chance that acute pulmonary embolism is present. These prediction scores assign points to a variety of clinical factors, with cumulative scores corresponding to designations of the probability of PE before testing (pretest probability). For example, the Wells score result is classified as likely or unlikely for PE. Clinical probability scoring has been best studied in patients presenting to the emergency department.
One of the important clinical criteria is a judgment of whether PE is more likely than an alternate diagnosis, and this determination is somewhat subjective. However, the clinical judgment of experienced clinicians is as sensitive as, or even more sensitive than, results from formal prediction scores. PE should probably be considered more likely if one or more of the symptoms and signs, particularly dyspnea, hemoptysis, tachycardia, or hypoxemia, cannot be explained clinically or by chest x-ray results.
Pretest probability guides testing strategy and the interpretation of test results. In patients in whom the probability of PE is unlikely, only minimal additional testing (ie, D-dimer testing in outpatients) may be needed. In such cases, a negative D-dimer test (< 0.4 mcg/mL [< 2.2 nmol/L]) is highly indicative of the absence of pulmonary embolism. Conversely, if there is a high clinical suspicion of PE and the risk of bleeding is low, immediate anticoagulation should be considered while the diagnosis is confirmed with additional tests.
The PERC rule specifies 8 criteria. Presence of all these criteria in a patient who, based on clinical findings, is at low risk specifies that testing for PE is not indicated (2). The criteria are:
Age < 50 years
Heart rate < 100
Oxygen saturation ≥ 95%
No prior deep venous thrombosis or pulmonary embolism
No unilateral leg swelling
No estrogen use
No hemoptysis
No surgery or trauma requiring hospitalization within the past 4 weeks
Use of the PERC rule has been recommended as a way to decrease rates of testing for PE with conventional testing using D-dimer, but with similar rates of sensitivity and negative predictive values.
Diagnostic testing
Screening of outpatients with D-dimer testing if pre-test probability is low or of intermediate probability
If pretest probability is high or if D-dimer result is elevated, CT angiography, or if renal insufficiency is present or when CT contrast is contraindicated, with ventilation/perfusion (V/Q) scanning
Sometimes ultrasonography of the legs or arms (to confirm deep venous thrombosis when lung imaging is delayed or prohibitive)
There is no universally accepted algorithm for the approach to suspected acute pulmonary embolism. Tests most useful for diagnosing or excluding PE are
D-dimer testing
CT angiography
Ventilation/perfusion scanning
Duplex ultrasonography
Echocardiography may be useful to identify pulmonary embolism on the way to the lung (clot-in-transit) or to find evidence of new right ventricular dysfunction. Echocardiographic findings that may suggest pulmonary embolism include the 60/60 sign, which is the combination of a pulmonary artery acceleration time of < 60 milliseconds with a peak systolic tricuspid valve gradient of < 60 mm Hg (3), and the McConnell sign, which is depressed contractility of the RV free wall compared to the RV apex (4).
D-Dimer is a by-product of intrinsic fibrinolysis; thus, elevated levels occur in the presence of a recent thrombus. Historically, when pretest probability is considered low or intermediate, a negative D-dimer level (< 0.4 mcg/mL [< 2.2 nmol/L]) is highly sensitive for the absence of PE with a negative predictive value of > 95%; in most cases, this result is sufficiently reliable for excluding the diagnosis of PE in the emergency department or clinic. More recently, data have shown that age can elevate D-dimer levels, which can cause a false-positive test result. Therefore, in patients with a low or intermediate pretest probability of PE and age over 50 years, the most common correction factor is to use a cutoff value of age multiplied by 10 in ng/mL. However, elevated D-dimer levels are not specific for venous thrombus because many patients without deep venous thrombosis (DVT) or PE also have elevated levels (particularly in patients who are hospitalized). Therefore, further testing is required when the D-dimer level is elevated or when the pretest probability for PE is high.
CT angiography is the preferred imaging technique for diagnosing acute pulmonary embolism. It is rapid, accurate, and highly sensitive and specific. It can also give more information about other lung pathology (eg, demonstration of pneumonia rather than PE as a cause of hypoxia or pleuritic chest pain) as well as severity of PE (for example by the size of the right ventricle or the reflux into the hepatic veins). Although poor quality scans due to motion artifact or poor contrast boluses can limit the sensitivity of the examination, CT technology now allows acquisition times of < 2 seconds, providing relatively motion-free images in patients with dyspnea. Fast scanning times allow the use of smaller volumes of iodinated contrast, which reduces the risk of acute kidney injury.

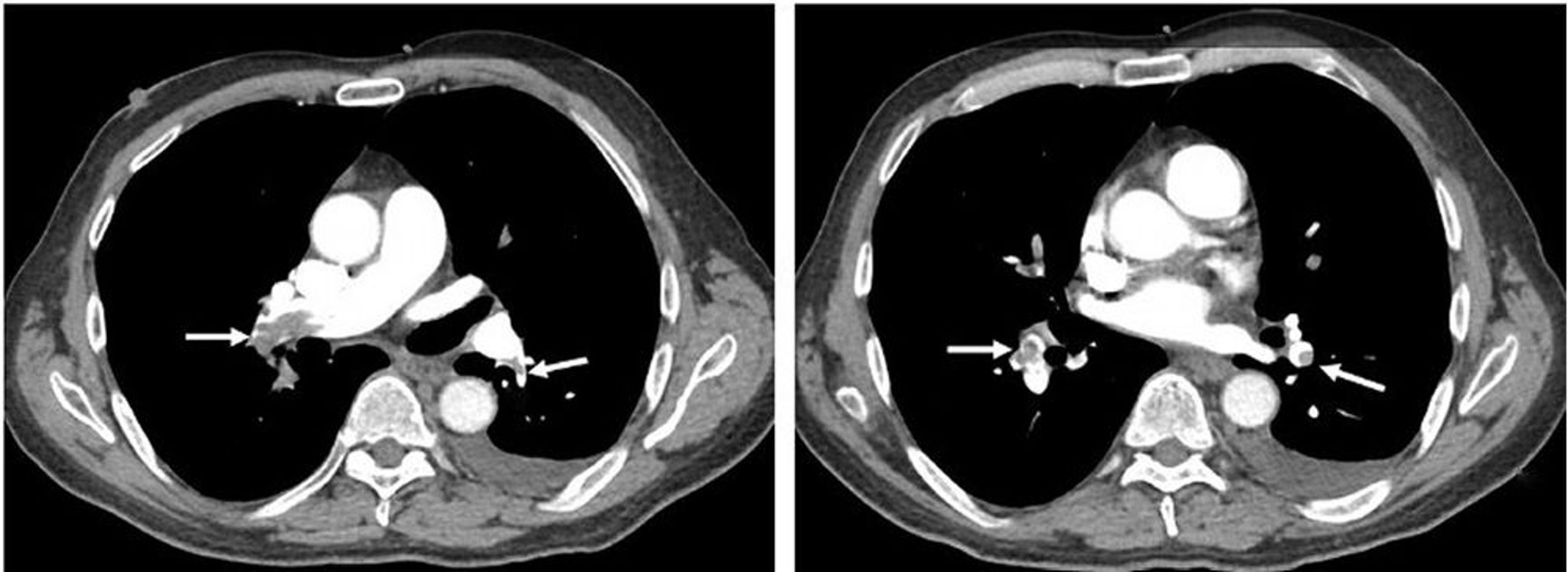
Image courtesy of Victor F. Tapson, MD.
The sensitivity of CT angiography is highest for pulmonary embolism in the main pulmonary artery or lobar or segmental vessels. Sensitivity of CT angiography is lowest for emboli in subsegmental vessels (about 30% of all pulmonary emboli). However, CT angiography is still the preferred means of diagnosing acute PE if there are no contraindications.
Ventilation/perfusion (V/Q) scans in pulmonary embolism detect areas of lung that are ventilated but not perfused. V/Q scanning takes longer than CT angiography and is less specific. However, when chest x-ray findings are normal or near normal and no significant underlying lung disease exists, it is a highly sensitive test. V/Q scanning is particularly useful when renal insufficiency precludes the use of contrast agents, which are otherwise required for CT angiography, and in pregnant patients (5). In some hospitals, V/Q scanning can be done with a portable machine that provides 3 views of ventilation and perfusion, which is useful when a patient is too ill to move. Perfusion defects may occur in many other lung conditions (eg, COPD, pulmonary fibrosis, pneumonia, pleural effusion). Mismatched perfusion defects that may mimic PE may occur in pulmonary vasculitis, pulmonary veno-occlusive disease, and sarcoidosis.
Results are based on patterns of V/Q mismatch and typically are reported as
Normal: Excludes PE with nearly 100% accuracy
Very low probability: < 5%
Low probability: 15% likelihood of PE
Intermediate probability: 30 to 40% probability of PE
High probability: 80 to 90% probability of PE
The results of clinical probability testing must be used together with the scan result to determine the need for treatment or further testing (6).

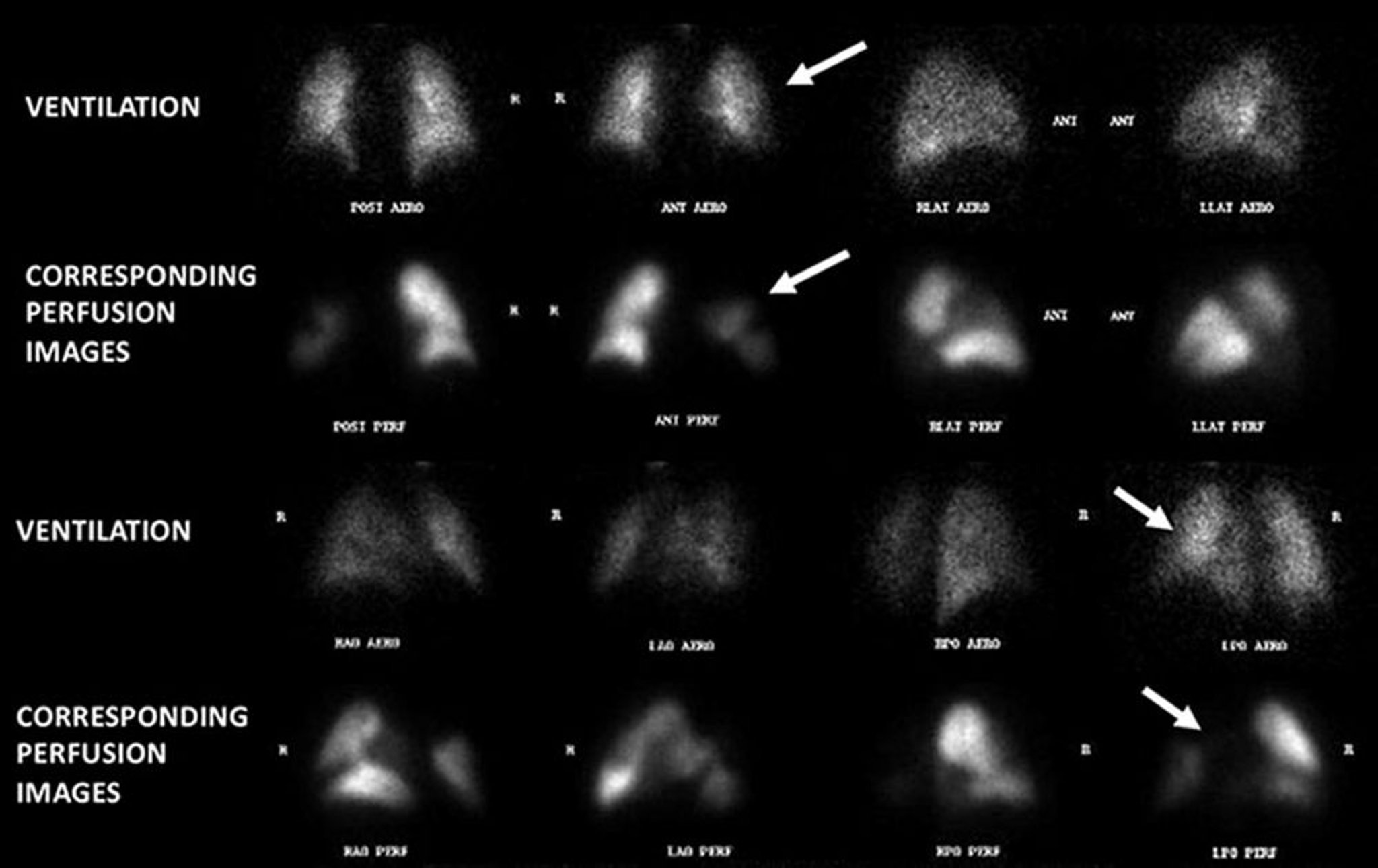
Image courtesy of Victor F. Tapson, MD.
Duplex ultrasonography is a safe, noninvasive, portable technique for detecting leg or arm thrombi. A clot can be detected by showing poor compressibility of the vein or by showing reduced flow by Doppler ultrasonography. The test has a sensitivity of > 95% and a specificity of > 95% for thrombus. Confirming DVT in the calf or iliac veins can be more difficult but can generally be accomplished. The ultrasound technician should always attempt to image below the popliteal vein into its trifurcation.
Absence of thrombi in the leg veins does not exclude the possibility of thrombus from other sources, such as the upper extremities or pelvic vasculature, but patients with suspected DVT and negative results on Doppler duplex ultrasonography have > 95% event-free survival, because thrombi from other sources are so much less common.
Although ultrasonography of the legs or arms is not diagnostic for PE, a study that reveals leg or axillary-subclavian thrombus establishes the need for anticoagulation and may obviate the need for further diagnostic testing unless more aggressive therapy (eg, thrombolytic therapy) is being considered. Therefore, stopping the diagnostic evaluation after detection of DVT on ultrasonography of the legs or arms is most appropriate for stable patients with contraindications to CT contrast and in whom V/Q scanning is expected to have low specificity (eg, in patients with an abnormal chest x-ray). In suspected acute PE, a negative ultrasound does not negate the need for additional studies.
Pearls & Pitfalls
|
Echocardiography may show a clot in the right atrium or ventricle, but echocardiography is most commonly used for risk stratification in acute PE. The presence of right ventricular dilation and hypokinesis may suggest the need for more aggressive therapy.
Cardiac marker testing is a useful means of stratifying mortality risk in patients with acute pulmonary embolism. Cardiac marker testing can be used as an adjunct to other testing if PE is suspected or proven. Elevated troponin levels signify right ventricular (or sometimes left ventricular) ischemia. Elevated brain natriuretic peptide (BNP) and pro-BNP levels may signify RV dysfunction; however, these tests are not specific for RV dysfunction or for PE.
Thrombotic disorder (thrombophilia) testing should not be done routinely. Testing should be considered for patients with unprovoked PE (ie, with no known risk factors or cause), especially if they are younger (age < 60 years), have recurrent PE, or have a positive family history. Certain thrombophilias, such as antiphospholipid syndrome, require disease-specific types of anticoagulation therapy. SARS-CoV-2 infection should be considered in the appropriate clinical setting.
Pulmonary arteriography is rarely needed to diagnose acute PE because noninvasive CT angiography has similar sensitivity and specificity. However, in patients in whom catheter-based thrombolytic therapy is being used, pulmonary angiography is useful for assessment of catheter placement and may be used as a rapid means of determining success of the procedure when the catheter is removed. Pulmonary arteriography is also used together with right-heart catheterization in assessing whether patients with chronic thromboembolic pulmonary hypertension are candidates for pulmonary endarterectomy.
Diagnosis references
1. Le Gal G, Righini M, Roy PM, et al: Prediction of pulmonary embolism in the emergency department: the revised Geneva score. Ann Intern Med 144:165–171, 2006.
2. Kline JA, Courtney DM, Kabrhel C, et al. Prospective multicenter evaluation of the pulmonary embolism rule-out criteria. J Thromb Haemost 6(5):772-780, 2008. doi:10.1111/j.1538-7836.2008.02944.x
3. Kurzyna M, Torbicki A, Pruszczyk P, et al: Disturbed right ventricular ejection pattern as a new Doppler echocardiographic sign of acute pulmonary embolism. Am J Cardiol 90(5):507–511, 2002. doi:10.1016/s0002-9149(02)02523-7
4. McConnell MV, Solomon SD, Rayan ME, et al: Regional right ventricular dysfunction detected by echocardiography in acute pulmonary embolism. Am J Cardiol 78(4):469–473, 1996. doi:10.1016/s0002-9149(96)00339-6
5. Leung AN, Bull TM, Jaeschke R, et al. An official American Thoracic Society/Society of Thoracic Radiology clinical practice guideline: evaluation of suspected pulmonary embolism in pregnancy. Am J Respir Crit Care Med 2011;184(10):1200-1208. doi:10.1164/rccm.201108-1575ST
6. PIOPED Investigators: Value of the ventilation/perfusion scan in acute pulmonary embolism. Results of the prospective investigation of pulmonary embolism diagnosis (PIOPED). JAMA 263(20):2753–2759, 1990. doi:10.1001/jama.1990.03440200057023
General Treatment of Pulmonary Embolism
Supportive therapy
Anticoagulation
Inferior vena cava filter placement (rarely, in selected patients)
Rapid clot burden reduction via thrombolysis or embolectomy (in selected patients)
Rapid assessment
In general,
Patients at low risk should receive anticoagulation alone
Patients at high risk require anticoagulation plus additional measures such as systemic thrombolysis or surgical or catheter-directed therapy
For patients at intermediate risk (high or low), treatment considerations are more complicated. Patients who are at intermediate-low risk are most commonly treated with anticoagulation alone. However, patients in intermediate-risk categories require repeat assessment of the entire clinical picture for any clinical deterioration, including
Deterioration of vital signs
Severity of RV dysfunction by echocardiography
Amount of oxygen and need for vasopressor agents
Clot burden and location
Anticoagulation is the mainstay of therapy for PE, and rapid reduction of clot burden via thrombolytic therapy or embolectomy is indicated for patients with hypotension that does not resolve after fluid resuscitation, and for selected patients with impaired RV function or escalating oxygen requirements. Placement of a removable percutaneous inferior vena cava filter (IVCF) should be considered for patients with contraindications to anticoagulation or for those with recurrent PE despite anticoagulation. For example, patients who have acute PE and residual clot in the leg and cannot be anticoagulated, should have a filter placed because they have persistent risk of subsequent deep venous thrombosis.
Hospitalization for at least 24 to 48 hours is done for most patients with PE. Patients with abnormal vital signs or high risk or intermediate risk PE require longer periods of hospitalization.
ICU (intensive care unit) admission is required for patients with high risk PE. ICU admission should also be considered if patients have
Extensive clot burden
RV compromise
Significant hypoxemia
Low or borderline blood pressure
Clinical deterioration
Outpatient management may be used for select patients who are at low risk and have incidentally discovered PE or for those with very small clot burdens and minimal symptoms provided their vital signs are stable, education is undertaken, and a reasonable plan for outpatient treatment and follow-up is in place.
Pulmonary embolism response team (PERT)
Given the evolving therapeutic options and the lack of randomized controlled trials, choosing appropriate treatment for individual patients can be challenging. Many hospitals use a multidisciplinary group of clinicians (pulmonary embolus response team) to rapidly evaluate patients, determine the level of pulmonary embolism risk, and make the complex treatment decisions needed. These teams may be comprised of clinicians in pulmonary/critical care medicine, interventional cardiology, interventional radiology, cardiothoracic surgery, hematology, emergency medicine, and other specialties. Recent single-center studies published have shown lower rates of bleeding, shorter time to therapeutic anticoagulation, decreased 30-day mortality, and decreased use of IVC filters in patients whose care is managed by a PERT. The use of PERT in the management of acute PE is now recommended by the European Society of Cardiology (1, 2).
General treatment references
1. Chaudhury P, Gadre SK, Schneider E, et al. Impact of Multidisciplinary Pulmonary Embolism Response Team Availability on Management and Outcomes. Am J Cardiol 2019;124(9):1465-1469. doi:10.1016/j.amjcard.2019.07.043
2. Konstantinides SV, Meyer G, Becattini C, et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS): The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC). Eur Respir J 2019;54(3):1901647. doi:10.1183/13993003.01647-2019
Anticoagulation in Pulmonary Embolism
Initial anticoagulation followed by maintenance anticoagulation is indicated for patients with acute pulmonary embolism to prevent further embolization as well as new clot formation. Anticoagulant therapy for acute PE should be started whenever PE is strongly suspected, as long as the risk of bleeding is deemed low. Otherwise, anticoagulation should be started as soon as the diagnosis is made.
The likelihood of benefit versus harm in treating emboli in smaller, subsegmental vessels (particularly asymptomatic and incidentally discovered emboli) is currently unknown, and it is possible that for certain patients harm may outweigh benefit. Still, treatment is recommended for the vast majority of patients.
The primary complication of anticoagulation therapy is bleeding, and patients should be closely observed for bleeding during hospitalization.
Initial anticoagulation
Initial anticoagulation choices for acute PE include
Factor Xa
Direct thrombinheparin-induced thrombocytopenia
heparin is given, followed by an infusion of heparin dosed by protocol to achieve an activated partial thromboplastin time (PTT) 1.5 to 2.5 times that of normal control. Therefore, unfractionated heparin requires ongoing hospitalization to administer. Further, the pharmacokinetics of unfractionated heparin are relatively unpredictable, resulting in frequent periods of over-anticoagulation and under-anticoagulation and necessitating frequent dose adjustments. Some clinicians prefer this IV unfractionated heparin regimen when thrombolytic therapy is given or contemplated or when patients are at risk of bleeding because if bleeding occurs, the short half-life means that anticoagulation is quickly reversed after the infusion is stopped.
Superior bioavailability
Ease of administration (can be given subcutaneously once or twice a day)
Decreased incidence of bleeding
Potentially better outcomes
The potential for patients to self-inject (thereby allowing earlier discharge from the hospital)
Lower risk of heparin
In patients with renal insufficiency, dose reductions are needed, and subsequent verification of appropriate dosing should be done by checking serum factor Xa
Adverse effects of all heparins include
Bleeding
Thrombocytopenia (including with the potential for thromboembolism)
Urticaria
Anaphylaxis (rare)
heparin
is a factor Xa antagonist given subcutaneously. It can be used in acute DVT and acute PE instead of heparin or low molecular weight heparin. Outcomes appear to be similar to those of unfractionated heparin. Advantages include once or twice a day fixed-dose administration, no need for monitoring of the degree of anticoagulation, and lower risk of thrombocytopenia. The drug is contraindicated if creatinine clearance is < 30 mL/minute.
The other factor Xa inhibitors,maintenance anticoagulants with no need for laboratory monitoring of the anticoagulant effect. They also cause few adverse interactions with other drugs, although azole antifungal therapy and older HIV therapies (protease inhibitors) will increase oral factor Xafactor Xa
Anticoagulation reversal of the oral factor Xa1). The half-lives of the factor Xa
The safety and efficacy of these medications in patients with PE complicated by severe cardiopulmonary decompensation have not yet been studied, and parenteral drugs should be used for anticoagulation in these patients until there is significant improvement in cardiopulmonary function.
The direct thrombin inhibitorDabigatrandabigatran.
Finally, in patients with suspected or proven 2).
Maintenance anticoagulation
Maintenance anticoagulation is indicated to reduce the risk of clot extension or embolization and to reduce the risk of new clot formation. Medication choices for maintenance anticoagulation include
Oral vitamin K
Oral factor Xa
Oral direct thrombin
warfarin therapy for a minimum of 5 days and until the international normalized ratio (INR) has been within the therapeutic range (2.0 to 3.0) for at least 24 hours.
warfarin should be wary of such interactions; in a patient taking warfarin, virtually any newly ingested drug or substance should be checked.
Bleeding is the most common complication of warfarin treatment; patients > 65 years and those with comorbidities (especially diabetes, recent myocardial infarction, hematocrit < 30%, or creatinine > 1.5 mg/dL [>133 micromol/L]) and a history of stroke or gastrointestinal bleeding seem to be at greatest risk. Bleeding can be reversed with vitamin K and, in an emergency, with fresh frozen plasma or a new concentrate formulation (prothrombin complex concentrates) containing factor II (prothrombin), factor VII, factor IX, factor X, protein C, and protein S. Vitamin K may cause flushing, local pain, and, rarely, anaphylaxis.
Warfarin-induced necrosis, a devastating complication of warfarin therapy, is a paradoxical hypercoagulable state that can arise upon the initiation of warfarin. Warfarin inactivates vitamin K-dependent clotting factors II, VII, IX, and X. At the same time, vitamin K-dependent proteins C and S are inactivated. This may cause a paradoxical hypercoagulable state in which microthrombi form in cutaneous and subcutaneous venules, resulting in skin necrosis. Based on these considerations and the development of more convenient oral anticoagulants, warfarin use has been declining substantially. However, cost considerations continue to make warfarina reasonable treatment option for some patients.
Pearls & Pitfalls
|
The oral factor Xa inhibitor anticoagulantsOral Anticoagulants3, 456) were as effective (in non-inferiority analyses) as warfarin in preventing recurrent DVT and PE. A meta-analysis of large phase III randomized controlled trials found that rates of major bleeding, including intracranial hemorrhage, were significantly lower with oral factor Xa inhibitor anticoagulants than with warfarin (78).
The direct thrombindabigatran than with warfarin. The use of dabigatran as maintenance therapy has the same advantages and disadvantages as the use of the factor Xa inhibitors.
9).
aspirin in patients already treated with anticoagulation for 6 to 12 months (8).
Duration of anticoagulation
Duration of maintenance anticoagulation for PE is dependent on a variety of factors (eg, risk factors for PE, bleeding risk) and can range from 3 months to lifelong therapy. Clearly transient risk factors (eg, immobilization, recent surgery, trauma) require only 3 months of treatment. Patients with unprovoked PE, those with more durable risk factors for PE (eg, cancer, thrombophilic disorder), and those with recurrent PE might benefit from lifelong anticoagulation provided the bleeding risk is low or moderate. In patients with unprovoked venous thromboembolism, annual assessment of bleeding risk versus clotting risk should be done and an informed joint decision regarding continuing anticoagulation reached.
Risk factors for bleeding include
Age > 65 years
Previous bleeding
Thrombocytopenia
Antiplatelet therapy
Poor anticoagulant control
Frequent falls
Liver failure
Alcohol overuse
Recent surgery
Reduced functional capacity
Previous stroke
Diabetes
Anemia
Cancer
Renal failure
Low risk for bleeding is defined as no risk factors for bleeding, moderate risk for bleeding is defined as one risk factor, and high risk for bleeding is defined as two or more risk factors.
Anticoagulation references
1. Yee J, Kaide CG. Emergency Reversal of Anticoagulation. West J Emerg Med 2019;20(5):770-783. doi:10.5811/westjem.2018.5.38235
2. Nilius H, Kaufmann J, Cuker A, Nagler M. Comparative effectiveness and safety of anticoagulants for the treatment of heparin-induced thrombocytopenia. Am J Hematol 2021;96(7):805-815. doi:10.1002/ajh.26194
3. EINSTEIN Investigators, Bauersachs R, Berkowitz SD, et al: Oral rivaroxaban for symptomatic venous thromboembolism. N Engl J Med 363(26):2499–2510, 2010.
4. EINSTEIN-PE Investigators, Buller HR, Prins MH, et al: Oral rivaroxaban for the treatment of symptomatic pulmonary embolism. N Engl J Med 366 (14):1287–1297, 2012.
5. Agnelli G, Buller HR, Cohen A, et al: Oral apixaban for the treatment of acute venous thromboembolism. N Engl J Med 369(9):799–808, 2013.
6. Hokusai-VTE Investigators, Buller HR, Decousus H, et al: Edoxaban versus warfarin for the treatment of symptomatic venous thromboembolism. N Engl J Med 369(15): 1406–1415, 2013.
7. van Es N, Coppens M, Schulman S, et al: Direct oral anticoagulants compared with vitamin K antagonists for acute symptomatic venous thromboembolism: evidence from phase 3 trials. Blood124 (12): 1968–1975, 2014.
8. Weitz JI, Lensing AWA, Prins MH, et al: Rivaroxaban or aspirin for extended treatment of venous thromboembolism. N Engl J Med 376:1211–1222, 2017. doi: 10.1056/NEJMoa1700518.
9. Stevens SM, Woller SC, Kreuziger LB, et al: Antithrombotic therapy for VTE disease: Second update of the CHEST Guideline and Expert Panel Report [published correction appears in Chest 2022 Jul;162(1):269]. Chest 2021;160(6):e545-e608. doi:10.1016/j.chest.2021.07.055
Rapid Reduction of Clot Burden
Clot elimination by means of embolectomy or dissolution with IV or catheter-based thrombolytic therapy should be considered for acute pulmonary embolism associated with hypotension that does not resolve after fluid resuscitation (high-risk/massive PE). Patients who are hypotensive and require vasopressor therapy are obvious candidates. Patients with a systolic blood pressure < 90 mm Hg or a decrease from baseline value in systolic blood pressure > 40 mm Hg that lasts at least 15 minutes despite fluid challenge are hemodynamically compromised and are also candidates.
Although only anticoagulation is generally recommended for patients with mild RV dysfunction (based on clinical, ECG, or echocardiographic findings), thrombolytic therapy or embolectomy may be needed when RV compromise and/or hypoxemia is severe even when hypotension is not present, particularly when deterioration is likely as suggested by an increase in heart rate or decrease in oxygen saturation or blood pressure.
Systemic thrombolytic therapy
plasminogen activator [tPA]) offers a noninvasive way to rapidly restore pulmonary blood flow, but long-term benefits do not clearly outweigh the risk of hemorrhage in some patients. Experts agree that systemic thrombolytic therapy should be given to patients with hemodynamic compromise if there are no contraindications, particularly when other means of rapidly reducing clot burden are not readily available. Although no prospective randomized trial of systemic thrombolytic therapy has shown improved survival in patients with intermediate-risk/submassive PE, some experts recommend thrombolytics, particularly when patients also have numerous or large clots; very severe RV dysfunction; marked tachycardia; significant hypoxemia; other concomitant findings such as residual clot in the leg, positive troponin values, and/or elevated BNP values; and there are no active contraindications to its administration. Others reserve thrombolytic therapy only for patients with high-risk (massive) PE.
Absolute contraindications to thrombolytics include
Prior hemorrhagic stroke
Ischemic stroke within 1 year
Active external or internal bleeding from any source
Intracranial injury or surgery within 2 months
Intracranial tumor
Certain surgeries within the previous weeks
Relative contraindications include
Age > 75 years
Recent surgery (≤ 10 days)
Hemorrhagic diathesis (as in hepatic insufficiency)
Pregnancy
Recent punctures of large noncompressible veins (eg, subclavian vein)
Recent femoral artery catheterization (eg, ≤ 10 days)
Peptic ulcer disease or other conditions that increase the risk of bleeding
Severe hypertension (systolic blood pressure > 180 mm Hg or diastolic blood pressure > 110 mm Hg)
Head trauma from PE-induced syncope, even if brain CT is normal
Except for concurrent intracerebral hemorrhage, thrombolytic therapy is sometimes given to patients with high-risk (massive) PE who have "absolute contraindications" to such therapy if, without intervention, death is otherwise anticipated. In patients with relative contraindications, the decision to give systemic thrombolytics depends on individual patient factors.
Bleeding, if it occurs, can be reversed with cryoprecipitate or fresh frozen plasma. Accessible vascular access sites that are bleeding can be compressed. The potential for bleeding after systemic thrombolysis has led to increased implementation of catheter-directed thrombolysis, because much lower doses of thrombolytic agents are used.
Catheter-directed therapy
Catheter-directed PE therapy (thrombolytics, embolectomy) uses catheter placement in the pulmonary arteries for disruption, removal, and/or lysis of clot. Indications for its use are evolving in patients who are high risk and those at intermediate high risk. In catheter-directed PE thrombolytic therapy, the pulmonary arteries are accessed via a typical pulmonary arteriography procedure, and thrombolytics are delivered directly to large proximal emboli via the catheter. The most widely studied technique uses high-frequency, low-power ultrasonography. Ultrasonography accelerates thrombolysis by disaggregating fibrin strands and increasing permeability of lytic drug into the clot. Studies to date are limited to mainly single-arm studies and registries. One randomized controlled trial, the ULTIMA study, demonstrated that the use of catheter-directed thrombolytics in patients with proximal clot and evidence of RV strain leads to an improved RV/LV ratio at 24 hours compared with anticoagulation alone (1). However, there was no difference between the groups in RV function, RV/LV ratio at 90 days, or 90-day mortality (1).
Mechanical disruption, or removal of the thrombus via suction embolectomy without thrombolysis, is becoming more widely used. Mechanisms of clot removal include direct aspiration or fragmentation with aspiration. Devices for this purpose differ by size of catheter and method of embolectomy. If the use of thrombolysis is contraindicated, catheter-directed suction embolectomy may be considered and, depending on local resources and expertise, tried before surgical embolectomy. Data on the use of suction embolectomy devices are limited to patients at intermediate high risk or high risk who participated in single-arm studies and registries (2). Randomized controlled trials to help determine appropriate use of these devices in patients with PE are ongoing.
Surgical embolectomy
Surgical embolectomy is reserved for patients with PE who are hypotensive despite supportive measures (persistent systolic blood pressure ≤ 90 mm Hg after fluid therapy and oxygen or if vasopressor therapy is required) or on the verge of cardiac or respiratory arrest. Surgical embolectomy can be considered if use of thrombolysis is contraindicated, although catheter-directed suction embolectomy may be tried first. As with catheter-based thrombosis/clot extraction, the decision to proceed with embolectomy and the choice of technique depend on local resources and expertise. Surgical embolectomy as a management strategy for acute PE is decreasing in frequency as catheter-based percutaneous techniques become more widely available.
Extracorporeal membrane oxygenation
Extracorporeal membrane oxygenation (ECMO) has been used increasingly in catastrophic acute pulmonary embolism when thrombolysis is contraindicated or failed. ECMO may serve as a bridge to surgical embolectomy or catheter-directed therapy, or it may buy time for improvement with anticoagulation alone.
Rapid reduction in clot burden references
1. Kucher N, Boekstegers P, Müller OJ, et al. Randomized, controlled trial of ultrasound-assisted catheter-directed thrombolysis for acute intermediate-risk pulmonary embolism. Circulation 2014;129(4):479-486. doi:10.1161/CIRCULATIONAHA.113.005544
2. Hountras P, Bull TM. Advanced therapies for pulmonary embolism. Curr Opin Pulm Med 2020;26(5):397-405. doi:10.1097/MCP.0000000000000714
Prognosis for Pulmonary Embolism
Most deaths resulting from pulmonary embolism occur withing 1 hour of presentation (1). Most patients who die as a result of acute PE are never diagnosed before death. In fact, PE is not suspected in most of these patients. Overall in-hospital mortality rate ranges from approximately 8% in stable patients to 25% in those presenting with cardiogenic shock and to 65% in patients requiring cardiopulmonary resuscitation (2).
The best prospects for reducing mortality involve
Improving the frequency of diagnosis (eg, by including PE in the differential diagnosis when patients present with nonspecific but compatible symptoms or signs)
Improving the rapidity of diagnosis
Improving risk stratification
Improving the rapidity of initiation of anticoagulation therapy
Providing appropriate prophylaxis in at-risk patients
Very high D-dimer levels appear to predict a poor outcome.
Patients with chronic thromboembolic disease represent a small, but important fraction of patients with PE who survive. Anticoagulant therapy reduces the rate of recurrence of PE to about 5% and even lower in some cases.
Prognosis references
1. Wood KE. Major pulmonary embolism: review of a pathophysiologic approach to the golden hour of hemodynamically significant pulmonary embolism. Chest 2002;121(3):877-905. doi:10.1378/chest.121.3.877
2. Kasper W, Konstantinides S, Geibel A, et al. Management strategies and determinants of outcome in acute major pulmonary embolism: results of a multicenter registry. J Am Coll Cardiol 1997;30(5):1165-1171. doi:10.1016/s0735-1097(97)00319-7
Prevention of Pulmonary Embolism
Prevention of acute venous thromboembolism
Prevention of pulmonary embolism means prevention of deep venous thrombosis (DVT); the need depends on the patient’s risks, including
Type and duration of any surgery
Comorbid conditions, including cancer and hypercoagulable disorders
Presence of a central venous catheter
Prior history of DVT or PE
Bedbound hospitalized patients and patients undergoing surgical, especially orthopedic, procedures benefit significantly from venous thromboembolism prophylaxis, and most of these patients can be identified before a thrombus forms (see table Risk Assessment for Thrombosis
Choice of drug or device depends on various factors, including patient demographics, the perceived risk, contraindications (eg, bleeding risk), relative costs, and ease of use. The American College of Chest Physicians has published comprehensive evidence-based recommendations for prophylaxis of acute DVT, including the duration of prophylaxis, in surgical and nonsurgical patients and during pregnancy (1, 2). The need for prophylaxis has been studied in numerous patient populations.
The type of surgery as well as patient-specific factors determine the risk of DVT. Independent risk factors include
Age ≥ 60 years
Prior DVT or PE
Cancer
Anesthesia ≥ 2 hours
Bed rest ≥ 4 days
Male sex
Hospital stay ≥ 2 days
Sepsis
Pregnancy or the postpartum state
Central venous access
Body mass index (BMI) > 40
The Caprini score is commonly used for DVT risk stratification and determination of the need for DVT prophylaxis in surgical patients (see table Risk Assessment for Thrombosis).
The need for DVT prophylaxis is based on the risk assessment score (see table Prophylaxis Based on Caprini Score
Medication regimens for pulmonary embolism prevention
Medication therapy to prevent DVT is usually delayed until after surgery to help avoid intraoperative bleeding. However, preoperative prophylaxis is also effective.
In general surgery patients,
dosing for DVT prophylaxisheparin for preventing DVT and PE.
heparin-induced thrombocytopenia or some other situations, such as after major orthopedic surgery (3). It is a selective factor Xa inhibitor.
is usually effective and safe at a dose adjusted to maintain an INR of 2 to 3 in patients who have undergone total hip or knee replacement. Warfarin use is increasingly being supplanted by the use of direct oral anticoagulants.
The direct oral anticoagulantsfactor Xa inhibitors. They can be used for prevention of acute DVT/PE in patients undergoing total knee or hip arthroplasty.
Prophylactic devices for pulmonary embolism
Inferior vena cava filters, intermittent pneumatic compression (also known as sequential compression devices [SCD]), and graded elastic compression stockings may be used alone or in combination with medications to prevent PE. Whether these devices are used alone or in combination depends on the specific indication.
An inferior vena cava filter (IVCF) may help prevent PE in patients with DVT in the leg or pelvic vasculature, but IVCF placement may risk long-term complications. More recent evidence raises questions regarding the efficacy of retrievable filters in patients receiving anticoagulation (4). A filter is most clearly indicated in patients who have
Proven DVT and contraindications to anticoagulation
Recurrent DVT (or emboli) despite adequate anticoagulation
Possibly marginal cardiopulmonary function, causing concern for their ability to tolerate additional small emboli
Because venous collaterals can develop, providing a pathway for emboli to circumvent long-standing IVCFs, and because filters occasionally thrombose, patients with recurrent DVT or nonmodifiable risk factors for DVT may still require anticoagulation. An IVCF is placed in the inferior vena cava just below the renal veins via catheterization of an internal jugular or femoral vein. Most IVCFs used currently are removable. Occasionally, a filter dislodges and may migrate up the venous bed, even to the heart or pulmonary vasculature. A filter can also become thrombosed, causing severe venous congestion (including acute phlegmasia cerulea dolens) in the leg, lower body ischemia, and acute kidney injury (5).
Intermittent pneumatic compression (IPC) with SCDs provides rhythmic external compression to the legs or to the legs and thighs. It is more effective for preventing calf than proximal DVT. It is insufficient as sole prophylaxis after hip or knee replacement but is often used in low-risk patients after other types of surgery or in medical patients who have a low-risk of DVT or who are at high risk of bleeding. IPC can theoretically trigger PE in immobilized patients who have developed occult DVT while not receiving DVT prophylaxis.
Graded elastic compression stockings are likely less effective than external pneumatic leg compression.
Choices for prevention of pulmonary embolism
After orthopedic surgery of the hip or knee,
For total hip arthroplasty, patients should continue to take anticoagulants for 35 days postoperatively. In selected patients at very high risk of both DVT/PE and bleeding, temporary placement of an IVCF is an option for prophylaxis.
In patients undergoing elective neurosurgical procedures,
In patients with spinal cord injury or multiple trauma,6). For patients at very high risk, a temporary IVCF may be considered.
In acutely ill medical patients,
Prevention references
1. Kearon C, Akl EA, Ornelas J, et al. Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report [published correction appears in Chest 2016 Oct;150(4):988]. Chest 2016;149(2):315-352. doi:10.1016/j.chest.2015.11.026
2. Stevens SM, Woller SC, Kreuziger LB, et al. Antithrombotic Therapy for VTE Disease: Second Update of the CHEST Guideline and Expert Panel Report [published correction appears in Chest 2022 Jul;162(1):269]. Chest 2021;160(6):e545-e608. doi:10.1016/j.chest.2021.07.055
3. Tran AH, Lee G. Fondaparinux for prevention of venous thromboembolism in major orthopedic surgery. Ann Pharmacother 2003;37(11):1632-1643. doi:10.1345/aph.1C104
4. Mismetti P, Laporte S, Pellerin O, et al. Effect of a retrievable inferior vena cava filter plus anticoagulation vs anticoagulation alone on risk of recurrent pulmonary embolism: a randomized clinical trial. JAMA 2015;313(16):1627-1635. doi:10.1001/jama.2015.3780
5. Marron RM, Rali P, Hountras P, Bull TM. Inferior Vena Cava Filters: Past, Present, and Future. Chest 2020;158(6):2579-2589. doi:10.1016/j.chest.2020.08.002
6. Aito S, Pieri A, D'Andrea M, Marcelli F, Cominelli E. Primary prevention of deep venous thrombosis and pulmonary embolism in acute spinal cord injured patients. Spinal Cord 2002;40(6):300-303. doi:10.1038/sj.sc.3101298
Key Points
Acute pulmonary embolism (PE) is a common and potentially devastating medical condition.
Clinical suspicion and a confirmatory diagnosis are essential because in most patients who die from acute PE, PE is not even suspected.
Because anticoagulation improves survival, patients should be given anticoagulants when PE is diagnosed or strongly suspected.
Patients with high risk/massive PE and certain patients with intermediate risk/submassive PE should be considered for thrombolytic therapy or embolectomy.
Prevention of deep venous thrombosis (and thus PE) should be considered in all patients who are hospitalized and at risk.
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
Konstantinides SV, Meyer G, Becattini C, et al: 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur Heart J. 2020 Jan 21;41(4):543-603. doi: 10.1093/eurheartj/ehz405
Stevens SM, Woller SC, Kreuziger LB, et al. Antithrombotic Therapy for VTE Disease: Second Update of the CHEST Guideline and Expert Panel Report [published correction appears in Chest 2022 Jul;162(1):269]. Chest 2021;160(6):e545-e608. doi:10.1016/j.chest.2021.07.055






