


Asbestosis is a form of interstitial pulmonary fibrosis caused by asbestos exposure. Asbestosis can cause progressive dyspnea on exertion, nonproductive cough, and fatigue. Diagnosis is based on history and chest x-ray or CT findings. Treatment is supportive.
(See also Overview of Asbestos-Related Disorders and Overview of Environmental and Occupational Pulmonary Disease.)
Asbestos is a family of naturally occurring silicates whose heat-resistant and structural properties are useful in construction and shipbuilding materials, automobile brakes, and some textiles. There are two main classes of asbestos: serpentine (which includes chrysotile) and amphibole (which includes amosite, crocidolite, anthophyllite, tremolite, and actinolite).
Asbestosis is a form of interstitial lung disease caused by asbestos exposure. The latency period between exposure and disease presentation is usually 20 to 40 years. Asbestosis appears earlier in patients with greater duration and intensity of exposure.
Risk factors
Direct occupational exposure remains the predominant cause of asbestos-related disease. In most developed countries, asbestos use has declined over the past several decades. Asbestos can still be found in old building materials and some products, and today most occupational exposures occur during repair, renovation, removal, or maintenance of asbestos-containing products installed in prior eras. Workplace exposure levels were generally much higher in the past.
Occupations that were traditionally associated with highest risk of exposure include construction trades (insulators, pipefitters, carpenters, electricians, roofers, drywall workers), maintenance workers, shipyard workers and Navy personnel, boilermakers and furnace workers, auto brake mechanics, and individuals involved with asbestos mining and processing.
Pathophysiology of Asbestosis
Alveolar macrophages attempting to engulf inhaled fibers release cytokines and growth factors that stimulate inflammation, oxidative injury, collagen deposition, and ultimately fibrosis. Asbestos fibers may also be directly toxic to lung tissue.
Risk of disease is generally related to the duration and intensity of exposure and the type, length, and thickness of inhaled fibers (1).
Pathophysiology reference
1. Solbes E, Harper RW. Biological responses to asbestos inhalation and pathogenesis of asbestos-related benign and malignant disease. J Investig Med 2018;66(4):721-727. doi:10.1136/jim-2017-000628
Symptoms and Signs of Asbestosis
The most common clinical presentation is gradual and progressive dyspnea on exertion, nonproductive cough, and fatigue.
Generally, asbestosis progresses slowly over many years and can continue to progress after cessation of exposure.
Severe cases can result in end-stage fibrosis and right ventricular failure (cor pulmonale).
Diagnosis of Asbestosis
Chest x-ray or preferably high-resolution chest CT
Sometimes bronchoalveolar lavage or lung biopsy
Diagnosis of asbestosis is based on history of exposure to asbestos and chest x-ray or high-resolution CT. History should include onset, duration, and type and intensity of the patient's exposure.
Chest x-ray shows bilateral, linear reticular opacities signifying fibrosis, usually in the peripheral lower lobes, with or without pleural changes. Chest CT offers higher sensitivity in identifying pleural and parenchymal abnormalities, and typically shows a usual interstitial pneumonia pattern of pulmonary fibrosis. Honeycombing, which may involve the mid and lower lung fields, signifies more advanced disease.
The International Labor Organization system (International Classification of Radiographs of Pneumoconioses) is used to characterize the presence and severity of pneumoconioses based on size, shape, location, and profusion of opacities. Asbestosis produces reticular opacities with a lower lobe predominance. Hilar and mediastinal adenopathy and nodular opacities are uncharacteristic and suggest a different diagnosis.
Pulmonary function tests may show restriction, reduced diffusing capacity for carbon monoxide (DLCO), and/or mild airflow obstruction. Such findings are nonspecific but help characterize the severity of disease.


Image courtesy of David W. Cugell, MD.

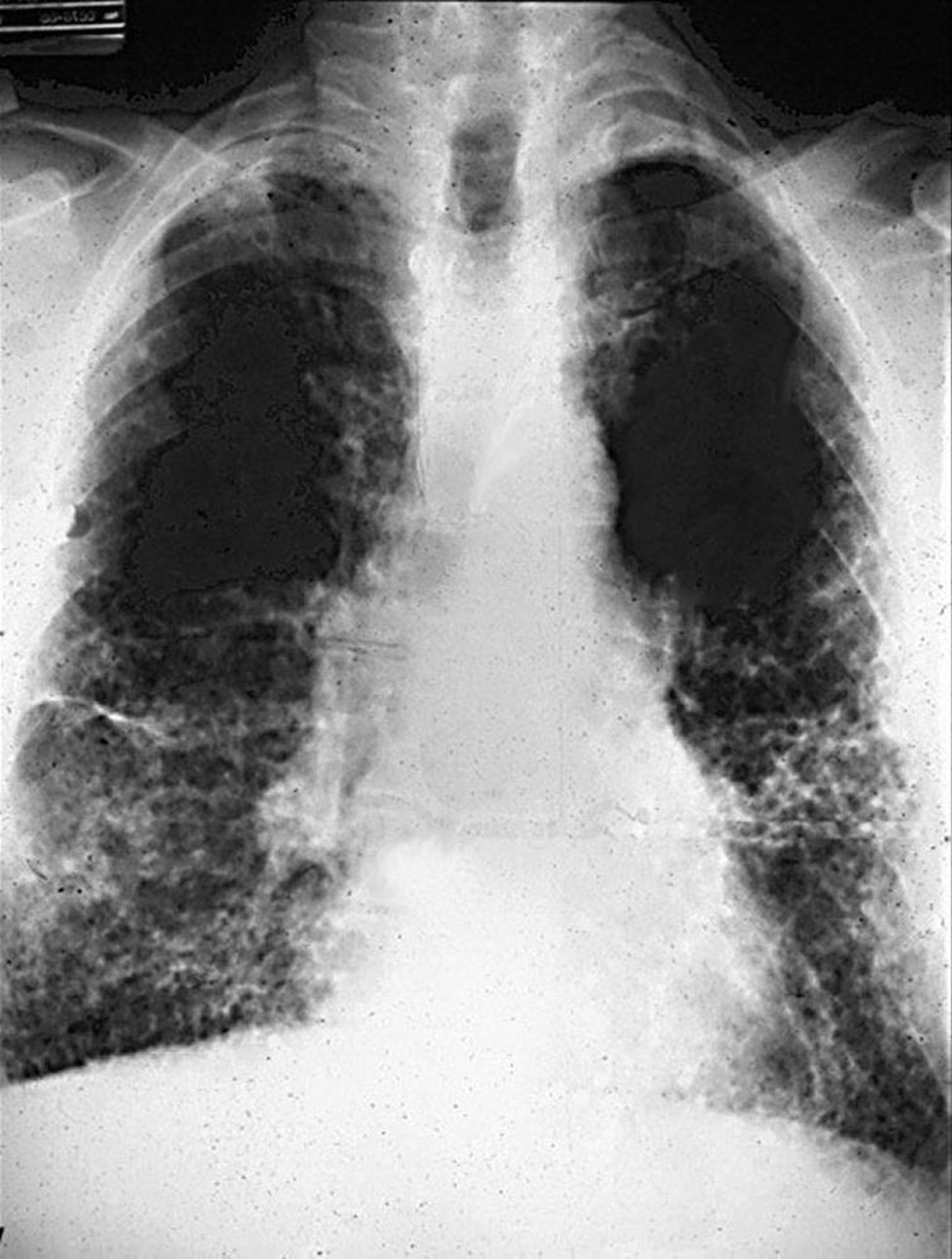
Image courtesy of David W. Cugell, MD.
Bronchoalveolar lavage or lung biopsy is potentially useful when the diagnosis is uncertain. The demonstration of asbestos fibers and/or asbestos bodies can help support the diagnosis but is not required.
Treatment of Asbestosis
Supportive care
No specific treatment exists. Patients should avoid further asbestos exposure.
Management is supportive, including the use of supplemental oxygen when indicated and prompt treatment of respiratory infections. Antifibrotic agents and immune therapies used in other interstitial lung diseases may have efficacy.
Pulmonary rehabilitation can be helpful for patients with impairment.
Patients with advanced disease may be eligible for lung transplantation.
Vaccination against influenza, COVID-19, and pneumonia is important in patients with asbestosis.
Prognosis for Asbestosis
Prognosis varies; asbestosis typically progresses slowly over many years. Many patients have mild symptoms and do well, whereas some develop progressive dyspnea and a few develop respiratory failure and right ventricular failure.
Patients with asbestosis have a significantly increased risk of lung cancer (usually non–small cell lung carcinoma). Additionally, asbestos and smoking have a synergistic effect on lung cancer risk. All forms of inhaled asbestos have been associated with an elevated risk of lung cancer.
Prevention of Asbestosis
Preventive measures include eliminating exposure, asbestos abatement in occupational and nonoccupational settings, and smoking cessation. Smoking cessation is critical considering the synergistic risk of lung cancer with smoking and asbestos exposure.
While there is no specific recommendation for lung cancer screening in asbestosis, patients who qualify for lung cancer screening based on recommendations for the general population should undergo annual screening.
Key Points
Although the use of asbestos has declined, due to the long latency of disease onset (20 to 40 years), asbestosis remains an important public health concern.
Diagnosis is based on a history of exposure to asbestos and radiographic evidence of interstitial lung disease.
Treatment is primarily supportive; smoking cessation is important.






