


11Beta-hydroxylase (CYP11B1) deficiency involves defective production of cortisol, with accumulation of mineralocorticoid precursors, resulting in hypernatremia, hypokalemia, and hypertension and increased production of adrenal androgens, leading to virilization. Diagnosis is by measurement of cortisol, its precursors, and adrenal androgens and sometimes by measuring 11-deoxycortisol after adrenocorticotropic hormone administration. Treatment is with a corticosteroid (1, 2).
11Beta-hydroxylase deficiency causes about 5 to 8% of all cases of congenital adrenal hyperplasia. Conversion of 11-deoxycortisol to cortisol and deoxycorticosterone to corticosterone is partially blocked, leading to
Increased levels of adrenocorticotropic hormone (ACTH)
Accumulation of 11-deoxycortisol (which has limited biological activity) and deoxycorticosterone (which has mineralocorticoid activity)
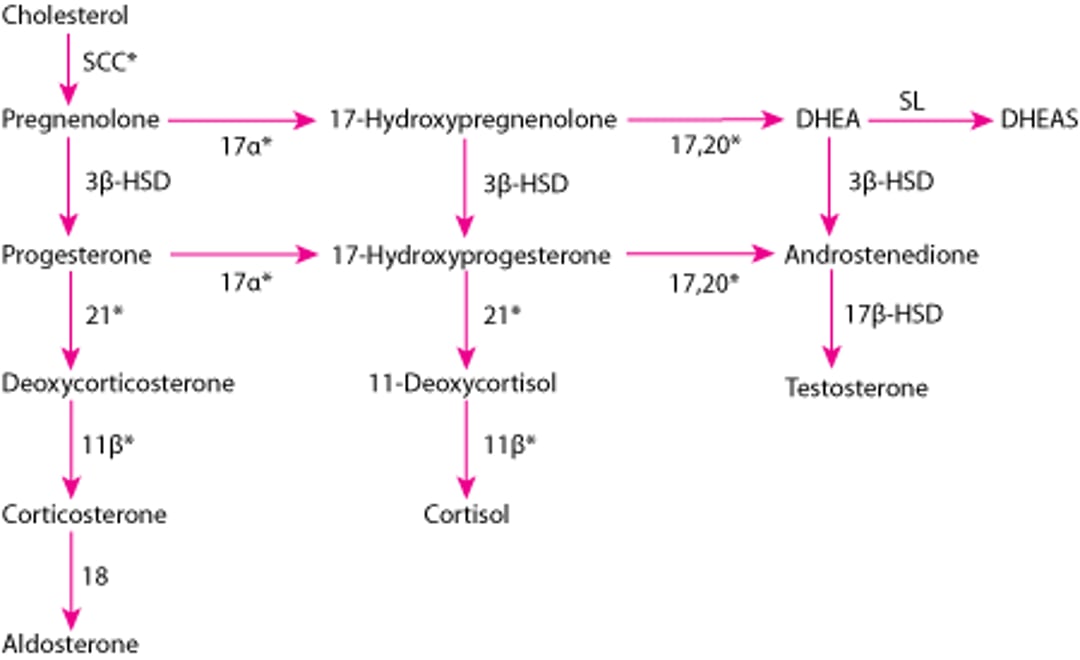
Adrenal hormone synthesis
* Enzymes stimulated by adrenocorticotropic hormone (ACTH). |
11β = 11β-hydroxylase (P-450c11); 17α = 17α-hydroxylase (P-450c17); 17,20 = 17,20 lyase (P-450c17); 18 = aldosterone synthase (P-450aldo); 21 = 21-hydroxylase (P-450c21); DHEA = dehydroepiandrosterone; DHEAS = DHEA sulfate; 3β-HSD = 3β-hydroxysteroid dehydrogenase (3β2-HSD); 17β-HSD = 17β-hydroxysteroid dehydrogenase (17β-HSD); SCC = side-chain cleavage (P-450scc); SL = sulfotransferase (SULT1A1, SULT1E1). |

General references
1. Witchel SF: Congenital adrenal hyperplasia. J Pediatr Adolesc Gynecol 30(5):520–534, 2017. doi: 10.1016/j.jpag.2017.04.001
2. El-Maouche D, Arlt W, Merke DP: Congenital adrenal hyperplasia. Lancet 390(10108):2194–2210, 2017. doi: 10.1016/S0140-6736(17)31431-9
Symptoms and Signs
Female neonates may present with genital ambiguity, including clitoral enlargement, labial fusion, and a urogenital sinus. Male neonates usually appear normal, but some present with penile enlargement. Some children present later, with precocious puberty or, in females, menstrual irregularities and hirsutism.
Salt retention with hypernatremia, hypertension, and hypokalemic alkalosis may result from increased mineralocorticoid activity due to increased deoxycorticosterone levels.
Diagnosis
Plasma levels of 11-deoxycortisol and adrenal androgens
Hypertension occurs in about two thirds of patients with CYP11B1 deficiency and distinguishes it from CYP21A2 deficiency, which causes hypotension. Because both CYP11B1 deficiency and CYP21A2
Pearls & Pitfalls
|
Treatment
Corticosteroid replacement
Sometimes antihypertensive therapy
Sometimes reconstructive surgery
2 orally 3 times a day, with total daily dose typically ≤ 20 mg/m2, which prevents further virilization and ameliorates hypertension by reducing levels of 11-deoxycortisol, deoxycorticosterone, and adrenal androgens that are stimulated by ACTH. Unlike CYP21A2 deficiency, mineralocorticoid replacement is not required, because sodium and potassium homeostasis is maintained from mineralocorticoid effects of deoxycorticosterone.
Response to treatment should be monitored, typically by measuring serum 11-deoxycortisol and adrenal androgens and by assessing growth velocity and skeletal maturation. Blood pressure should be monitored closely in patients who presented with hypertension. Antihypertensives, such as potassium-sparing diuretics or calcium channel blockers, may be required.
Affected female infants may require surgical reconstruction with reduction clitoroplasty and construction of a vaginal opening. Often, further surgery is required in adulthood, but with appropriate care and attention to psychosexual issues, normal sexual function and fertility may be expected.
Key Points
Children with 11beta-hydroxylase deficiency have excess mineralocorticoid activity and increased adrenal androgens, which cause hypertension, hypokalemia, and virilization.
In females, androgen excess usually manifests at birth with ambiguous external genitals (eg, clitoral enlargement, fusion of the labia majora, a urogenital sinus rather than distinct urethral and vaginal openings); later in life they may have hirsutism, oligomenorrhea, and acne.
Male infants usually appear normal but may later have precocious puberty.
Diagnose by steroid hormone levels and sometimes adrenocorticotropic hormone stimulation.
Treat with corticosteroid replacement and sometimes antihypertensives; females may require reconstructive surgery.






