


Cryptosporidiosis is infection with the protozoan Cryptosporidium
(See also Overview of Intestinal Protozoan and Microsporidia Infections.)
Pathophysiology of Cryptosporidiosis
Cryptosporidia are obligate, intracellular coccidian protozoa that replicate in small-bowel epithelial cells of a vertebrate host.
After Cryptosporidium oocysts are ingested, they excyst in the gastrointestinal tract and release sporozoites, which parasitize gastrointestinal epithelial cells. In these cells, the sporozoites transform into trophozoites, replicate, and produce oocysts.
Two types of oocysts are produced:
Thick-walled oocysts, which are commonly excreted from the host
Thin-walled oocysts, which are primarily involved in autoinfection
The thick-walled infective oocysts are shed into the lumen and passed in stool by the infected host; they are immediately infective and can be transmitted directly from person to person by the fecal-oral route. Very few oocysts (eg, < 100) are required to cause disease, thus increasing risk of person-to-person transmission.
When the infective oocysts are ingested by humans or another vertebrate host, the cycle begins again.

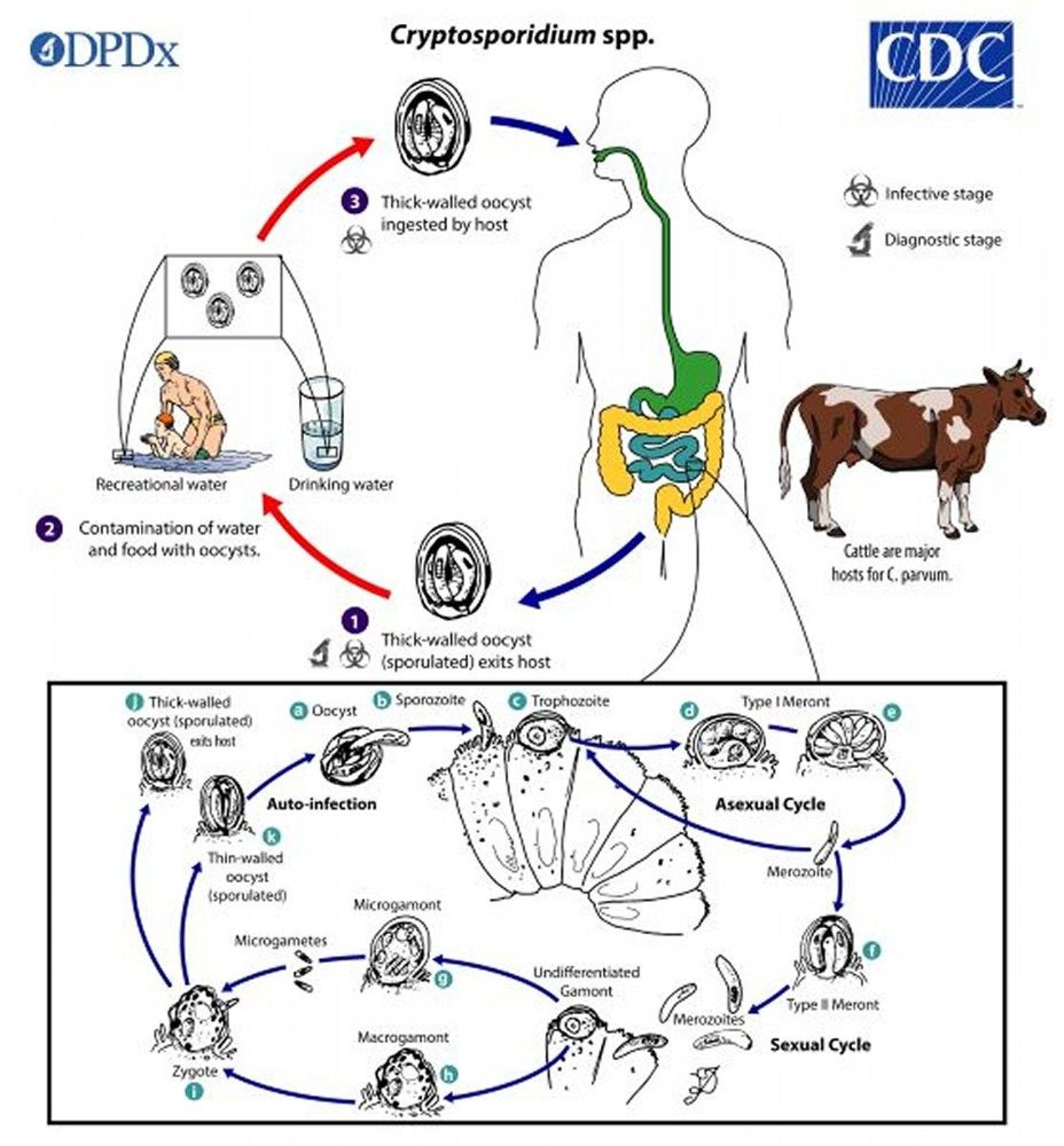
Image from the Centers for Disease Control and Prevention Image Library.
Oocysts are resistant to harsh conditions, including chlorine at levels usually used in public water treatment systems and swimming pools despite adherence to recommended residual chlorine levels.
Epidemiology of Cryptosporidiosis
Cryptosporidium species infect a wide range of animals. Cryptosporidium parvum and C. hominis (formerly C. parvum genotype 1) are responsible for most human cases of cryptosporidiosis. Infections by C. felis, C. meleagridis, C. canis, and C. muris have also been reported. Ingesting even a relatively small number of oocyts can result in disease. Infections result from the following:
Ingestion of fecally contaminated food or water (often water in public and residential pools, hot tubs, water parks, lakes, or streams)
Direct person-to-person contact
Zoonotic spread
The disease occurs worldwide. Cryptosporidiosis is responsible for 0.6 to 7.3% of diarrheal illness in countries with modern sanitation systems and an even higher percentage in areas with poor sanitation. In the US from 2009 to 2017, there were 444 reported cryptosporidiosis outbreaks resulting in 7,465 cases in 40 states and Puerto Rico. The number of reported outbreaks increased an average of 13% per year. Leading causes include swallowing contaminated water in pools or water playgrounds, contact with infected cattle, and contact with infected persons in child care settings (1). In Milwaukee, Wisconsin, > 400,000 people were affected during a waterborne outbreak in 1993, when the city’s water supply was contaminated by sewage during spring rains when the filtration system did not work correctly.
Children, travelers to foreign countries, immunocompromised patients, and medical personnel caring for patients with cryptosporidiosis are at increased risk. Outbreaks have occurred in day care centers. The small number of oocysts required to cause infection, the prolonged excretion of oocysts, the resistance of oocysts to chlorination, and their small size raise concern about swimming pools used by diapered children.
Severe, chronic diarrhea due to cryptosporidiosis is a problem in patients with AIDS, particularly those who have not received antiretroviral therapy (ART).
Epidemiology reference
1. Gharpure R, Perez A, Miller AD, et al: Cryptosporidiosis Outbreaks—United States, 2009-2017. MMWR Morb Mortal Wkly Rep 68:568-72, 2019.
Symptoms and Signs of Cryptosporidiosis
The incubation period for cryptosporidiosis is about 1 week, and clinical illness occurs in > 80% of infected people. Onset is typically abrupt, with watery diarrhea, abdominal cramping, and, less commonly, nausea, anorexia, fever, and malaise. Symptoms usually persist 2 to 3 weeks, rarely ≥ 1 month, and then abate. Fecal excretion of oocysts may continue for several weeks after symptoms have subsided. Asymptomatic shedding of oocysts is common among children in countries with poor sanitation. Cryptosporidiosis is also associated with undernutrition in children living in these areas.
In the immunocompromised host, onset may be more gradual, but diarrhea can be more severe. Unless the underlying immune defect is corrected, infection can persist, causing intractable diarrhea for life. Fluid losses of > 5 to 10 L/day have been reported in some AIDS patients. The intestine is the most common site of infection in immunocompromised hosts; however, other organs (eg, biliary tract, pancreas, respiratory tract) may be involved.
Diagnosis of Cryptosporidiosis
Enzyme immunoassay for fecal antigen or molecular probes for parasite DNA
Microscopic examination of stool (special techniques required)
Identifying the acid-fast oocysts in stool confirms the diagnosis of cryptosporidiosis, but conventional methods of stool examination (ie, routine "stool for ova and parasites" testing) are unreliable. Oocyst excretion is intermittent, and multiple stool samples may be needed. Several concentration techniques increase the yield. Cryptosporidium
Enzyme immunoassay for fecal Cryptosporidium antigen is more sensitive than microscopic examination for oocysts.
Sensitive and specific DNA-based assays for detection and speciation of C. parvum and C. hominis are available.
Intestinal biopsy can demonstrate Cryptosporidium within epithelial cells.
Treatment of Cryptosporidiosis
In immunocompetent people,
Age 1 to 3 years: 100 mg 2 times a day
Age 4 to 11 years: 200 mg 2 times a day
Age ≥ 12 years: 500 mg 2 times a day
No drug has proven efficacy in immunosuppressed patients. For HIV-infected patients, immune reconstitution with ART1).
Supportive measures, oral or parenteral rehydration, and hyperalimentation may be needed for immunocompromised patients with severe disease.
Treatment reference
1. Pantenburg B, Cabada MM, White AC Jr: Treatment of cryptosporidiosis. Expert Rev Anti Infect Ther 7(4):385-91, 2009. doi: 10.1586/eri.09.24
Prevention of Cryptosporidiosis
Prevention of cryptosporidiosis requires
Effective public water treatment
Hygienic food preparation
Special precautions during international travel
Appropriate fecal-oral hygiene
Thorough handwashing after contact with feces of humans and animals
Not swallowing water when swimming in lakes, rivers, streams, ocean, swimming pools, and hot tubs
Safer sex practices
Taking special care when traveling to areas with poor sanitation
Specific recommendations for the general public and people with compromised immunity due to AIDS or other causes are available from the Centers for Disease Control and Prevention (CDC). Stools of patients with cryptosporidiosis are highly infectious; strict stool precautions should be observed. Special biosafety guidelines have been developed for handling clinical specimens. Boiling potentially contaminated water for 1 min (3 min at altitudes > 2000 m [6562 ft]) is the most reliable decontamination method; only filters with pore sizes ≤ 1 micrometer (specified as “absolute 1 micron” or certified under NSF/ANSI International Standard No. 53 or No. 58) remove Cryptosporidium cysts.
Key Points
Cryptosporidiosis spreads easily because fecal excretion of oocysts persists for weeks after symptoms resolve, a very small number of oocysts are required for infection, and oocysts are difficult to remove by conventional water filtration and are resistant to chlorination.
Watery diarrhea with cramping is usually self-limited but can be severe and lifelong in patients with AIDS.
Diagnose using enzyme immunoassay for fecal Cryptosporidium antigen and microscopic stool examination; the latter is less sensitive and requires specialized techniques (eg, phase-contrast microscopy, acid-fast staining).
Treat people with AIDS with ART; symptoms may abate when the immune system improves with ART.
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
US Department of Health and Human Services: Guidelines for the Prevention and Treatment of Opportunistic Infections in HIV-Exposed and HIV-Infected Children
Centers for Disease Control and Prevention (CDC) Cryptosporidium Prevention & Control: Includes recommendations intended to help prevent and control cryptosporidiosis in the general public






