


Pathophysiology of Diabetic Retinopathy
Diabetic retinopathy is a major cause of blindness, particularly among working-age adults. The degree of retinopathy is highly correlated with
Duration of diabetes
Blood glucose levels
BP levels
Pregnancy can impair blood glucose control and thus worsen retinopathy.
Nonproliferative retinopathy
Nonproliferative retinopathy (also called background retinopathy) develops first and causes increased capillary permeability, microaneurysms, hemorrhages, exudates, macular ischemia, and macular edema (thickening of the retina caused by fluid leakage from capillaries).
Proliferative retinopathy
Proliferative retinopathy develops after nonproliferative retinopathy and is more severe; it may lead to vitreous hemorrhage and traction retinal detachment. Proliferative retinopathy is characterized by abnormal new vessel formation (neovascularization), which occurs on the inner (vitreous) surface of the retina and may extend into the vitreous cavity and cause vitreous hemorrhage. Neovascularization is often accompanied by preretinal fibrous tissue, which, along with the vitreous, can contract, resulting in traction retinal detachment. Neovascularization may also occur in the anterior segment of the eye on the iris; neovascular membrane growth in the anterior chamber angle of the eye at the peripheral margin of the iris can occur, and this growth leads to neovascular glaucoma. Vision loss with proliferative retinopathy may be severe.
Clinically significant macular edema can occur with nonproliferative or proliferative retinopathy and is the most common cause of vision loss due to diabetic retinopathy.
Symptoms and Signs of Diabetic Retinopathy
Nonproliferative retinopathy
Vision symptoms are caused by macular edema or macular ischemia. However, patients may not have vision loss even with advanced retinopathy. The first signs of nonproliferative retinopathy are
Capillary microaneurysms
Dot and blot retinal hemorrhages
Hard exudates
Cotton-wool spots (soft exudates)

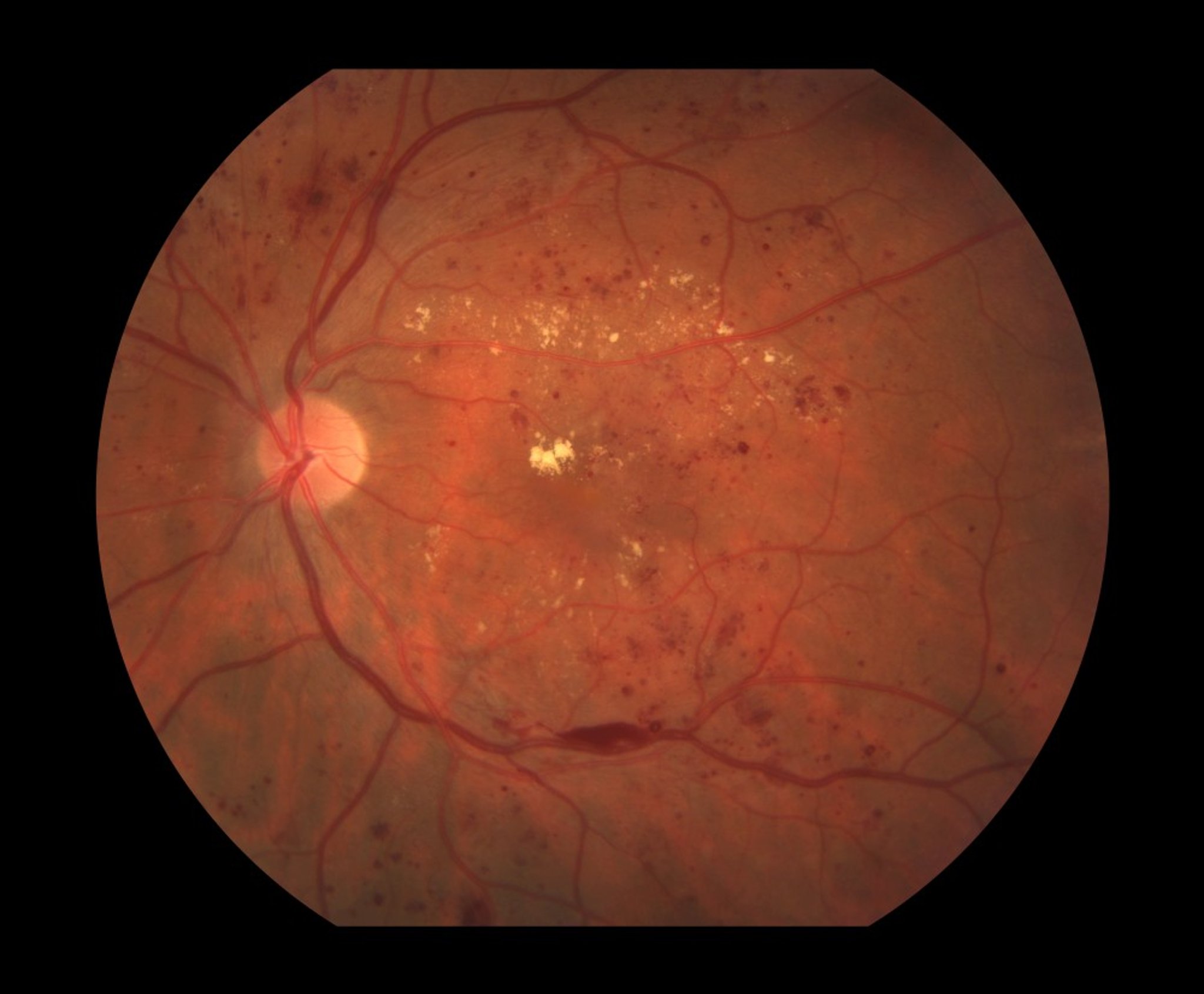
Paul Whitten/SCIENCE PHOTO LIBRARY
Hard exudates are discrete, yellow particles within the retina. When present, they suggest chronic edema. Cotton-wool spots are areas of microinfarction of the retinal nerve fiber layer that lead to retinal opacification; they are fuzzy-edged and white and obscure underlying vessels.
Signs in later stages are
Macular edema (seen on slit-lamp biomicroscopy as elevation and blurring of retinal layers)
Venous dilation and intraretinal microvascular abnormalities
Proliferative retinopathy
Symptoms may include blurred vision, floaters (black spots) or flashing lights (photopsias) in the field of vision, and sudden, severe, painless vision loss. These symptoms are typically caused by vitreous hemorrhage or traction retinal detachment.
Proliferative retinopathy, unlike nonproliferative retinopathy, causes formation of fine preretinal vessel neovascularization visible on the optic nerve or retinal surface. Macular edema or retinal hemorrhage may be visible on funduscopy.

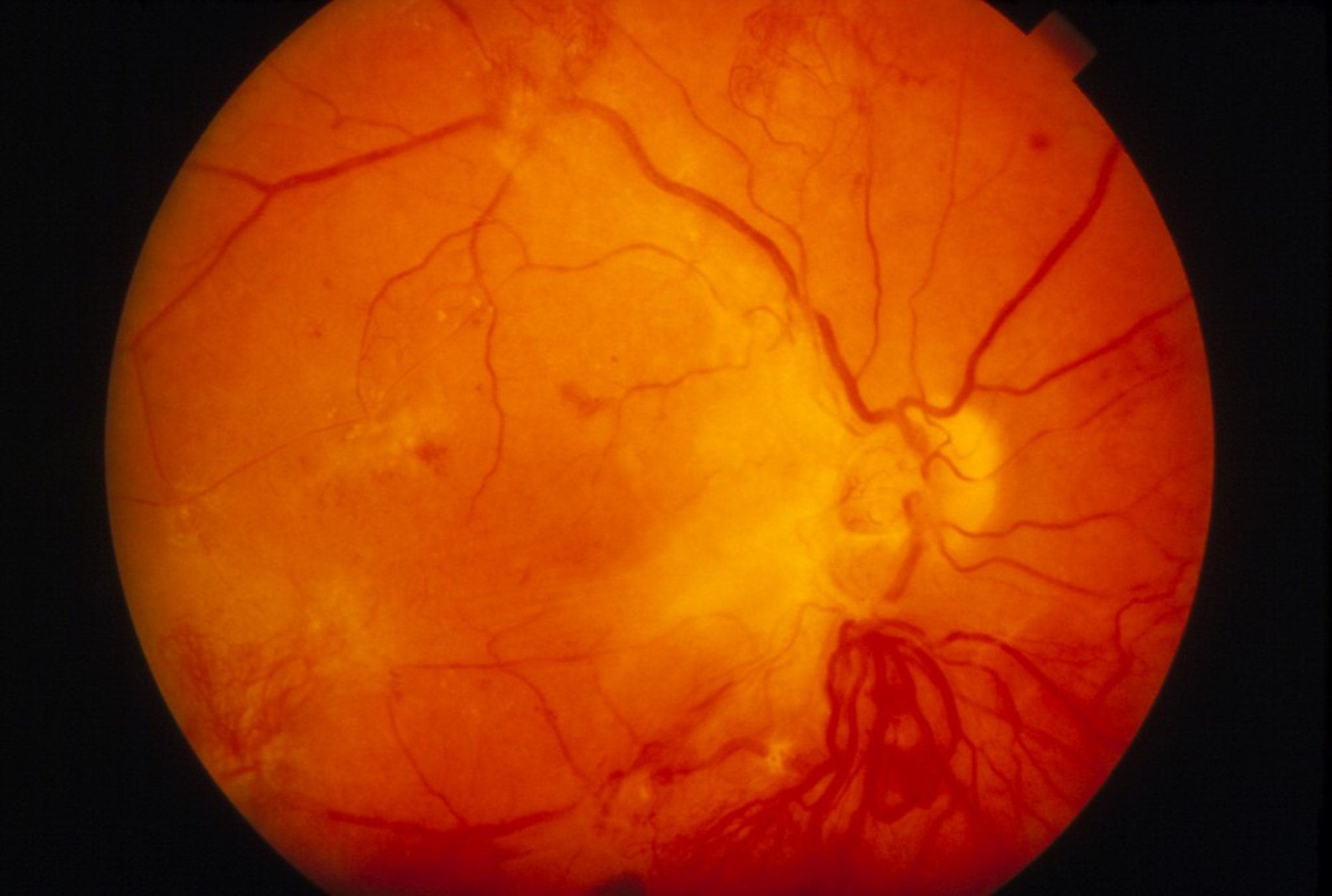
WESTERN OPHTHALMIC HOSPITAL/SCIENCE PHOTO LIBRARY
Diagnosis of Diabetic Retinopathy
Funduscopy
Color fundus photography
Optical coherence tomography
Screening
Because early detection is important, all patients with diabetes should have an annual dilated ophthalmologic examination. Pregnant patients with diabetes should be examined every trimester. Vision symptoms (eg, blurred vision) are indications for ophthalmologic referral.
Treatment of Diabetic Retinopathy
Control of blood glucose and blood pressure (BP)
For macular edema, intraocular injection of antivascular endothelial growth factor (anti-VEGF) drugs, intraocular corticosteroid implants, focal laser, and/or vitrectomy
For high-risk or complicated proliferative retinopathy, anti-VEGF drugs, panretinal laser photocoagulation and sometimes vitrectomy
In select cases of severe nonproliferative retinopathy, panretinal laser photocoagulation may be used; however, usually panretinal laser photocoagulation can be delayed until proliferative retinopathy develops.
Proliferative diabetic retinopathy with high-risk characteristics of vitreous hemorrhage, extensive preretinal neovascularization, or anterior segment neovascularization/neovascular glaucoma should be treated with panretinal laser photocoagulation. Studies have also supported the use of intravitreal anti-VEGF drugs in the treatment of proliferative diabetic retinopathy (2). These treatments significantly reduce the risk of severe vision loss.
Vitrectomy can help preserve and often restore lost vision in patients with any of the following:
Persistent vitreous hemorrhage
Extensive preretinal membrane formation
Traction retinal detachment
Recalcitrant diabetic macular edema
Treatment references
1. The Diabetic Retinopathy Clinical Research NetworkN Engl J Med372(13):1193-1203, 2015. doi:10.1056/NEJMoa1414264
2. Beaulieu WT, Bressler NM, Melia M, et alAm J Ophthalmol 170:206-213, 2016. doi: 10.1016/j.ajo.2016.08.008
Prevention of Diabetic Retinopathy
Control of blood glucose and blood pressure is critical; intensive control of blood glucose delays onset of retinopathy.
Key Points
Features of diabetic retinopathy can include microaneurysms, intraretinal hemorrhage, exudates, cotton-wool spots, macular edema, macular ischemia, neovascularization, vitreous hemorrhage, and traction retinal detachment.
Symptoms may not develop until damage is advanced.
Screen all diabetic patients with an annual dilated ophthalmologic examination.
Treat patients with high-risk or complicated proliferative retinopathy with panretinal laser photocoagulation, anti-VEGF drugs, and/or sometimes vitrectomy.






