


Growths can originate in any type of tissue in and around the mouth, including connective tissues, bone, muscle, and nerve. Most commonly, growths form on the lips, the sides of the tongue, the floor of the mouth, and the soft palate. Some growths cause pain or irritation. Growths may be noticed by the patient or discovered during examination.
(See also Evaluation of the Dental Patient, Oral Squamous Cell Carcinoma, Oropharyngeal Squamous Cell Carcinoma, and Candidiasis [Mucocutaneous].)
Etiology of Oral Growths
Oral growths can be
Benign
Premalignant (dysplastic)
Malignant
Benign oral growths
Most oral growths are benign; there are numerous types.

DR P. MARAZZI/SCIENCE PHOTO LIBRARY

DR P. MARAZZI/SCIENCE PHOTO LIBRARY

CLINICA CLAROS/SCIENCE PHOTO LIBRARY

Image provided by Thomas Habif, MD.

CLINICA CLAROS/SCIENCE PHOTO LIBRARY

DR P. MARAZZI/SCIENCE PHOTO LIBRARY
© Springer Science+Business Media

DR P. MARAZZI/SCIENCE PHOTO LIBRARY

DR. P. MARAZZI/SCIENCE PHOTO LIBRARY

Image courtesy of K. Mae Lennon and Clement Benjamin via the Public Health Image Library of the Centers for Disease Control and Prevention.


DR P. MARAZZI/SCIENCE PHOTO LIBRARY


DR P. MARAZZI/SCIENCE PHOTO LIBRARY

CLINICA CLAROS/SCIENCE PHOTO LIBRARY


Image provided by Thomas Habif, MD.


CLINICA CLAROS/SCIENCE PHOTO LIBRARY


DR P. MARAZZI/SCIENCE PHOTO LIBRARY

© Springer Science+Business Media

DR P. MARAZZI/SCIENCE PHOTO LIBRARY

DR. P. MARAZZI/SCIENCE PHOTO LIBRARY


Image courtesy of K. Mae Lennon and Clement Benjamin via the Public Health Image Library of the Centers for Disease Control and Prevention.
Chronic irritation can cause a persistent lump or raised area on the gingiva. Benign growths due to irritation are relatively common and, if necessary, can be removed by surgery. In 10 to 40% of people, benign growths on the gingiva reappear because the irritant remains. Occasionally such irritation, particularly if it persists over a long period of time, can lead to premalignant or malignant changes.
Warts may occur in the mouth (oral squamous papillomas). Ordinary warts (verrucae vulgaris) can infect the mouth if a person sucks or chews one that is growing on a finger. Genital warts, caused by human papillomavirus infection (HPV), may also occur in the oral cavity when transmitted through oral sex. Oral warts may regress spontaneously but slowly (over months or years). Typical treatment is complete surgical excision when possible.
Oral candidiasis (thrush) often appears as white, cheesy plaques that stick tightly to the mucous membranes and leave red erosions when wiped off. Thrush is most common among patients with diabetes or immunocompromise and among those who are taking antibiotics.
Cysts of many kinds cause jaw pain and swelling. Often they are associated with an impacted wisdom tooth and can destroy considerable areas of the mandible as they expand. Certain types of cysts are more likely to recur after surgical removal. Various types of cysts may develop in the floor of the mouth. Often, these cysts are surgically removed because they make swallowing uncomfortable or because they are unattractive.
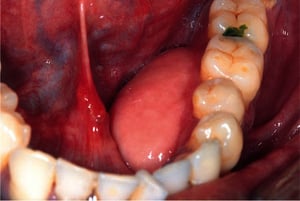
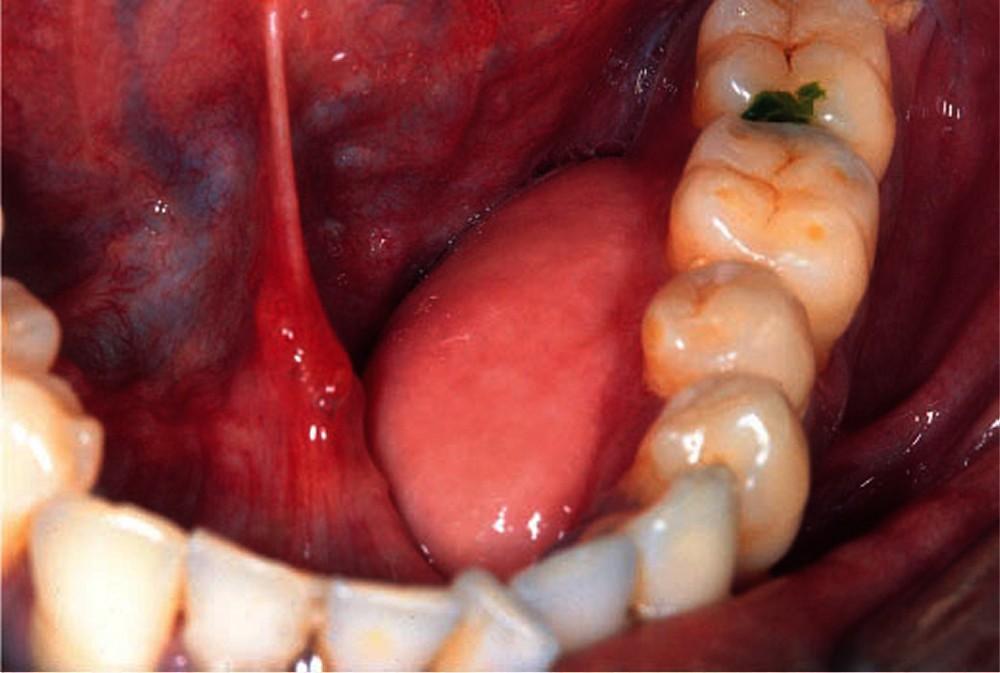
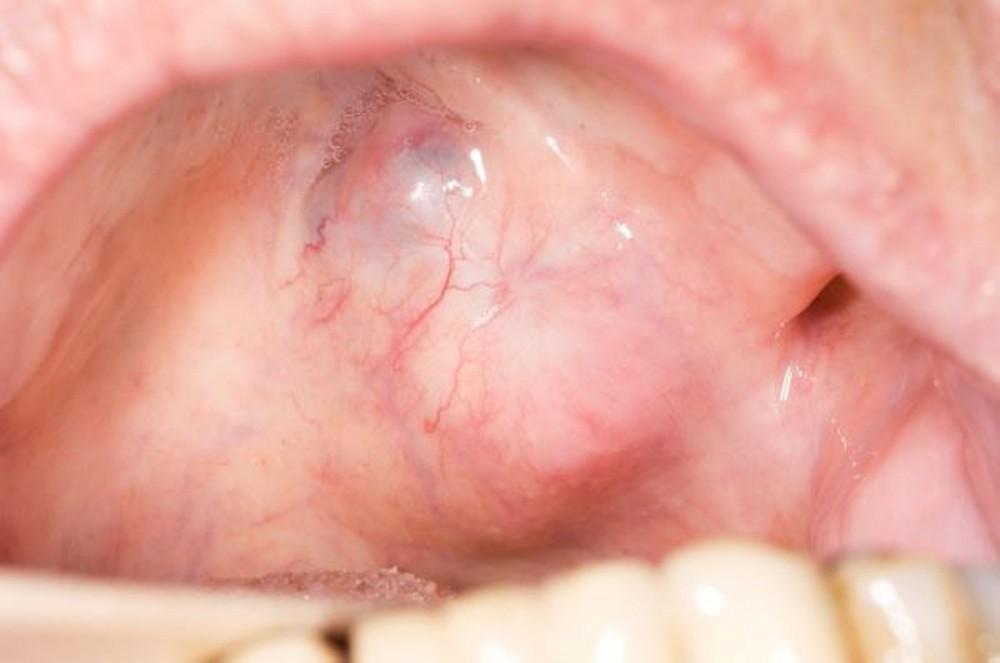
Mucoceles (mucus retention cysts and ranulas) are painless, benign, intraoral swellings due to cystic or pseudocystic accumulations of salivary gland mucus. They are often traumatic in origin. By far the most common lesion, mucoceles most often occur inside the lateral lower lip and often have a bluish translucent color due to presence of spilled mucin under the mucosa. They are usually the result of accidentally biting the (lower) lip and occur when salivary flow from a minor salivary gland is obstructed. Most mucoceles disappear in a week or two. Ranulas are large, usually bluish mucoceles on the floor of the mouth. Treatment is surgical excision.
A torus is a rounded projection of bone that forms in the midline of the hard palate (torus palatinus) or on the inner aspect of the mandible (torus mandibularis). This hard growth is both common and harmless. Even a large growth can be left alone unless it gets traumatized during eating or the person needs a denture that covers the area.
Gardner syndrome is a type of familial adenomatous polyposis, a hereditary disorder of the gastrointestinal tract that involves multiple colorectal polyps. Patients who have Gardner syndrome often present with multiple oral osteomas that may clinically resemble multiple torus lesions, particularly in the body and angle of the lower jaw.
Keratoacanthomas are growths that form on the lips and other sun-exposed areas, such as the face, forearms, and hands. A keratoacanthoma usually reaches its full size of about 1 to 3 cm or more in diameter within 1 or 2 months, then begins to shrink after another few months and may eventually disappear without treatment. Once, all keratoacanthomas were considered to be noncancerous, but some experts now consider those that do not diminish in size to be low-grade cancerous lesions, and biopsy or excision is currently recommended for such lesions. Some pathologists consider keratoacanthoma an incipient variant of squamous cell carcinoma (1).
Odontomas are overgrowths of tooth-forming cells that look like small, misshapen extra teeth. In children, they may get in the way of normal tooth eruption. In adults, they may push teeth out of alignment. Large odontomas may also cause enlargement of the maxilla or mandible. They are usually removed surgically.
Salivary gland tumors are mostly benign, slow-growing, and painless. They usually occur as a single, soft, movable lump beneath normal-appearing skin or under the oral mucosa. Occasionally, when hollow and fluid-filled, they are firm. The most common type is a pleomorphic adenoma (mixed tumor) and it occurs mainly in women > age 40. Pleomorphic adenomas can become malignant and are removed surgically. Unless completely removed, this type of tumor is likely to recur. Other types of benign tumors are also removed surgically but are much less likely to become malignant or recur.
Premalignant (dysplastic) changes
White, red, or mixed white-red areas that are not easily wiped away, persist for > 2 weeks, and are not definable as some other condition may be dysplastic. The same risk factors are involved in dysplastic changes as in malignant growths, and dysplastic changes may become malignant if not removed.


Leukoplakia is a flat white spot that may develop when the oral mucosa is irritated for a long period. The term leukoplakia is used when a white lesion on the oral mucosa cannot be characterized as any other definable lesion. The irritated spot appears white because it has a thickened layer of keratin, which normally is less abundant in the oral mucosa. Factors often associated with the development of idiopathic oral leukoplakia include tobacco use; alcohol consumption; deficiencies of vitamins C, B12, B6, B3; and endocrine disturbances.

Erythroplakia is a red and flat or worn-away area that results when the oral mucosa thins. The area appears red because the underlying capillaries are more visible. Erythroplakia is a much more ominous predictor of oral cancer than leukoplakia.


Mixed lesions show intermixed areas of leukoplakia and erythroplakia and also may be precursors of cancer.
Oral cancer
People who use tobacco, alcohol, or both are at much greater risk of oral cancer. For people who use chewing tobacco and snuff, the insides of the cheeks and lips are common sites. In other people, the most common sites for cancer include the lateral borders of the tongue, the floor of the mouth, and the oropharynx. Human papillomavirus (HPV) infection , especially type 16, is a risk factor for oral cancer, primarily in the tonsils and at the base of the tongue; at these sites, HPV16 has surpassed tobacco as the primary cause. Rarely, cancers found in the oral region have metastasized from the lungs, breast, or prostate.
Oral cancer can have many different appearances but typically resembles dysplastic lesions (eg, white, red, or mixed white-red areas that are not easily wiped away).
Reference
1. Kwiek B, Schwartz RA: Keratoacanthoma (KA): An update and review. J Am Acad Dermatol 74(6):1220-1233, 2016. doi: 10.1016/j.jaad.2015.11.033
Evaluation of Oral Growths
History
History of present illness includes questions about how long the growth has been present, whether it is painful, and whether there has been any injury to the area (eg, biting a cheek, scraping by a sharp tooth edge or dental restoration). Patients are asked about symptoms of systemic illness, particularly weight loss and malaise.
Past medical history should seek risk factors for candidiasis, including recent antibiotic use, diabetes, and HIV infection (or risk factors for HIV). The amount and duration of use of alcohol and tobacco are noted.
Physical examination
The physical examination focuses on the mouth and neck, inspecting and palpating all areas of the mouth and throat, including under the tongue. The neck is palpated for lymphadenopathy, which suggests possible cancer or chronic infection.
Red flags
The following findings are of particular concern:
Weight loss
Neck mass
Persistent sore throat
Difficulty swallowing
Interpretation of findings
The main concern is to not mistake an oral cancer or dysplastic lesion for a benign disorder. Clinicians should maintain a high degree of suspicion and refer the patient for biopsy if the lesion does not resolve in a few weeks.
Testing
Suspected candidiasis can be confirmed by finding yeast and pseudohyphae in 10% potassium hydroxide wet mounts of scrapings from a lesion. Other acute lesions, particularly those that appear related to local trauma or irritation, may be observed. However, most lesions that have been present for more than a few weeks, and those of unknown duration, should be biopsied because cancer is difficult to exclude clinically.
Treatment of Oral Growths
Treatment depends on the cause, aesthetic and functional impairments, pain, and malignant potential of the diagnosed growth.
Key Points
Most oral growths are benign.
Warts, candidal infections, and repeated trauma are common causes of benign growths.
Use of alcohol and tobacco and oral HPV infection are risk factors for cancer.
Because cancer is difficult to diagnose by inspection, biopsy is often necessary.






