A number of procedures are used to gain vascular access.
Peripheral Vein Catheterization
Most patients’ needs for IV fluid and drugs can be met with a percutaneous peripheral venous catheter. If blind percutaneous placement is difficult, ultrasonographic guidance usually results in successful placement. Venous cutdown can be used on the rare occasions when percutaneous catheter insertion is not feasible. Typical cutdown sites are the cephalic vein in the arm and the saphenous vein at the ankle. However, venous cutdown is rarely needed because of the popularity of peripherally inserted central catheter (PICC) lines and intraosseous lines in both adults and children.
For a step-by-step description of how to do peripheral vein catheterization, see How To Do Peripheral Vein Cannulation and How To Do Peripheral Vein Cannulation, Ultrasound-Guided.
Common complications (eg, local infection, venous thrombosis, thrombophlebitis, interstitial fluid extravasation) can be reduced by using a meticulous sterile technique during insertion and by replacing or removing the catheters within 72 hours.
Central Venous Catheterization
Patients needing secure or long-term vascular access (eg, to receive antibiotics, chemotherapy, or total parenteral nutrition) and those with poor peripheral venous access require a central venous catheter (CVC). CVCs allow infusion of solutions that are too concentrated or irritating for peripheral veins and allow monitoring of central venous pressure (CVP).
CVCs can be inserted through the jugular, subclavian, or femoral veins or via the upper arm peripheral veins (PICC line). Although the type of catheter and site chosen are often determined by individual clinical and patient characteristics, a jugular CVC or PICC line is usually preferred to a subclavian CVC (associated with a higher risk of bleeding and pneumothorax) or femoral CVC (associated with a higher risk of infection). During cardiac arrest, fluid and drugs given through a femoral vein CVC often fail to circulate above the diaphragm because of the increased intrathoracic pressure generated by cardiopulmonary resuscitation (CPR). In this case, a subclavian or internal jugular approach may be preferred.
Ultrasound guidance for placement of internal jugular lines and PICC lines is now standard care and reduces the risk of complications. Coagulopathy should be corrected whenever feasible prior to CVC insertion, and the subclavian approach should not be used in patients with uncorrected coagulopathy because the venipuncture site cannot be monitored or compressed.

© 2017 Elliot K. Fishman, MD.
For a step-by-step description of how to do central venous catheterization, see the following:
How To Do Infraclavicular Subclavian Vein Cannulation, Ultrasound-Guided
How To Do Internal Jugular Vein Cannulation, Ultrasound-Guided

Video created by Hospital Procedures Consultants at www.hospitalprocedures.org.
Video created by Hospital Procedures Consultants at www.hospitalprocedures.org.

Video created by Hospital Procedures Consultants at www.hospitalprocedures.org.

Video created by Hospital Procedures Consultants at www.hospitalprocedures.org.

Video created by Hospital Procedures Consultants at www.hospitalprocedures.org.

Video created by Hospital Procedures Consultants at www.hospitalprocedures.org.


Video created by Hospital Procedures Consultants at www.hospitalprocedures.org.
Video created by Hospital Procedures Consultants at www.hospitalprocedures.org.

Video created by Hospital Procedures Consultants at www.hospitalprocedures.org.

Video created by Hospital Procedures Consultants at www.hospitalprocedures.org.

Video created by Hospital Procedures Consultants at www.hospitalprocedures.org.

Video created by Hospital Procedures Consultants at www.hospitalprocedures.org.
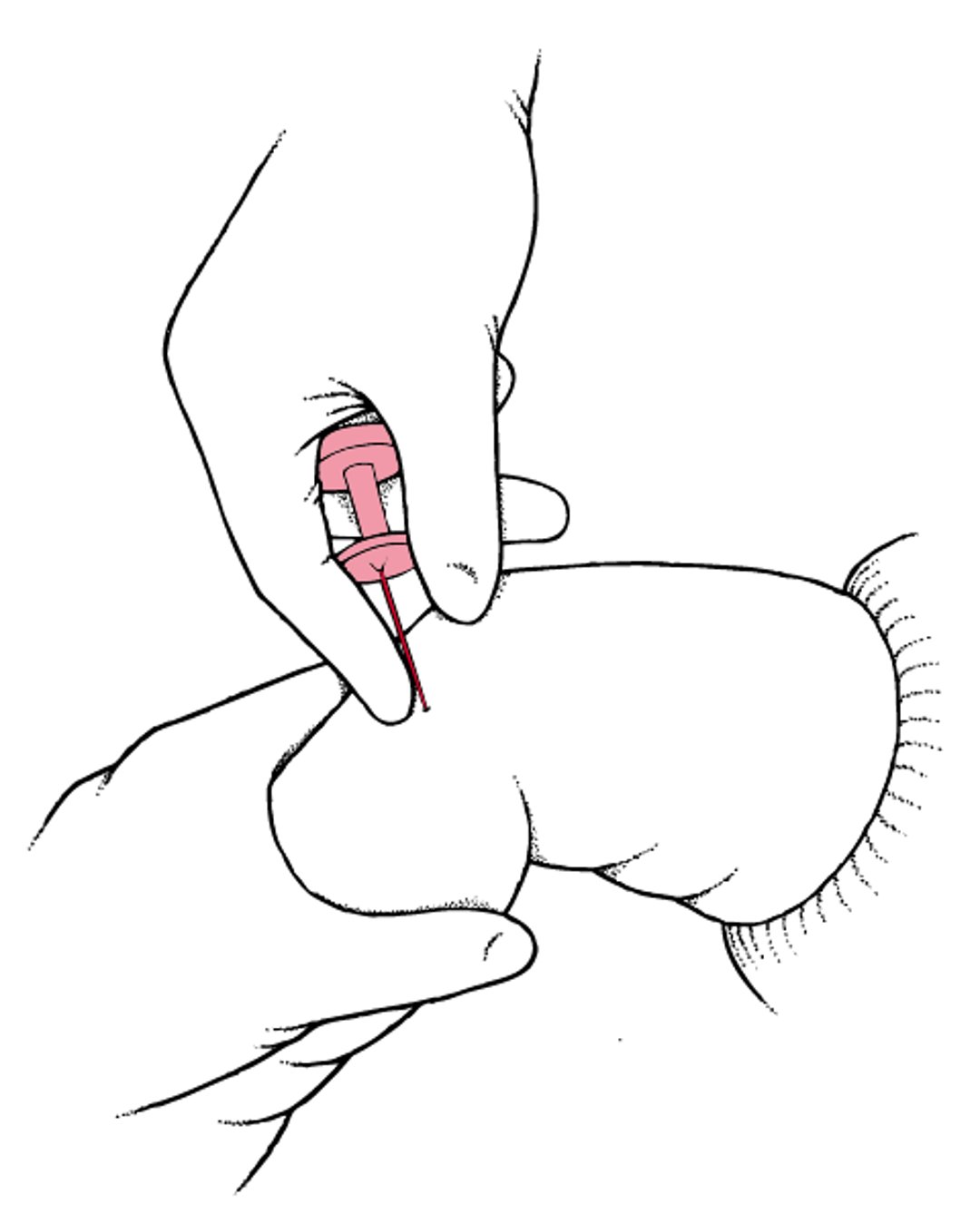
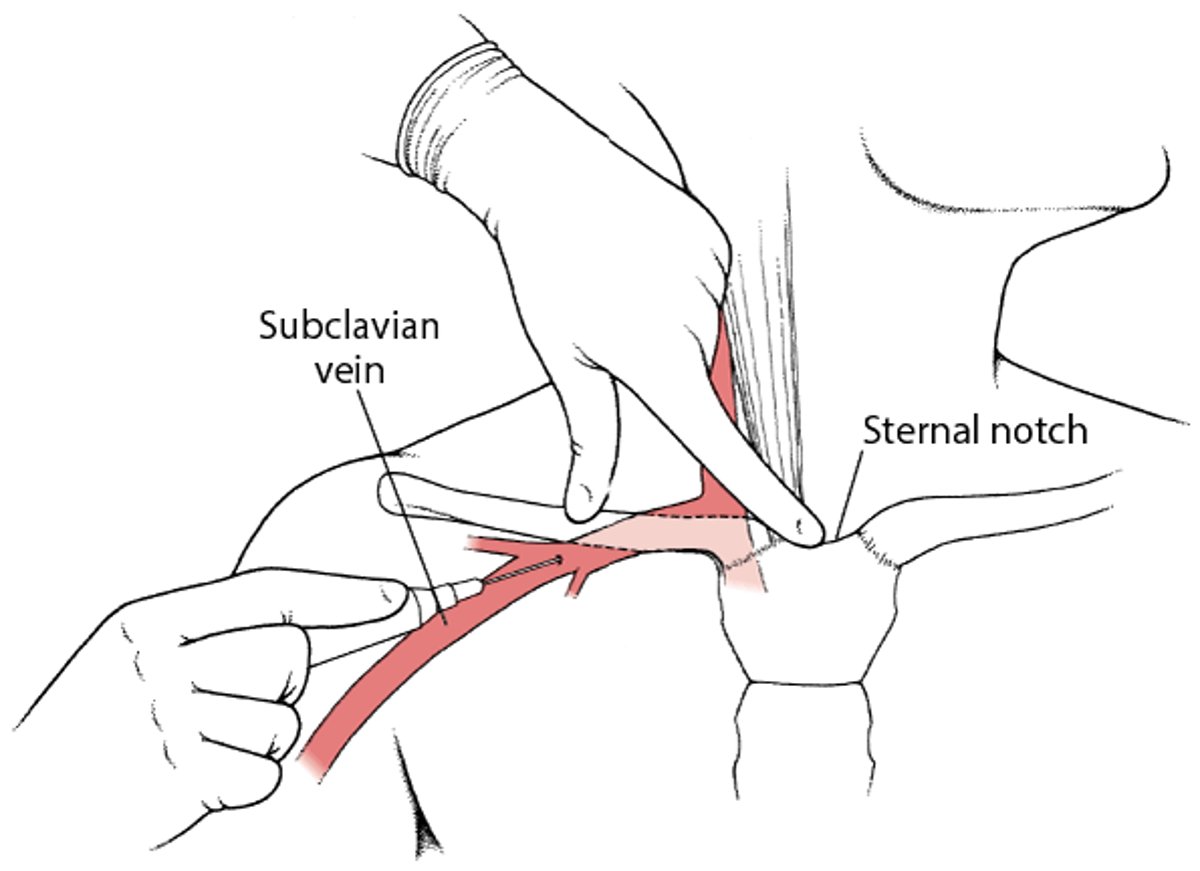
Subclavian venipuncture
This figure shows hand position during subclavian venipuncture (infraclavicular approach). |

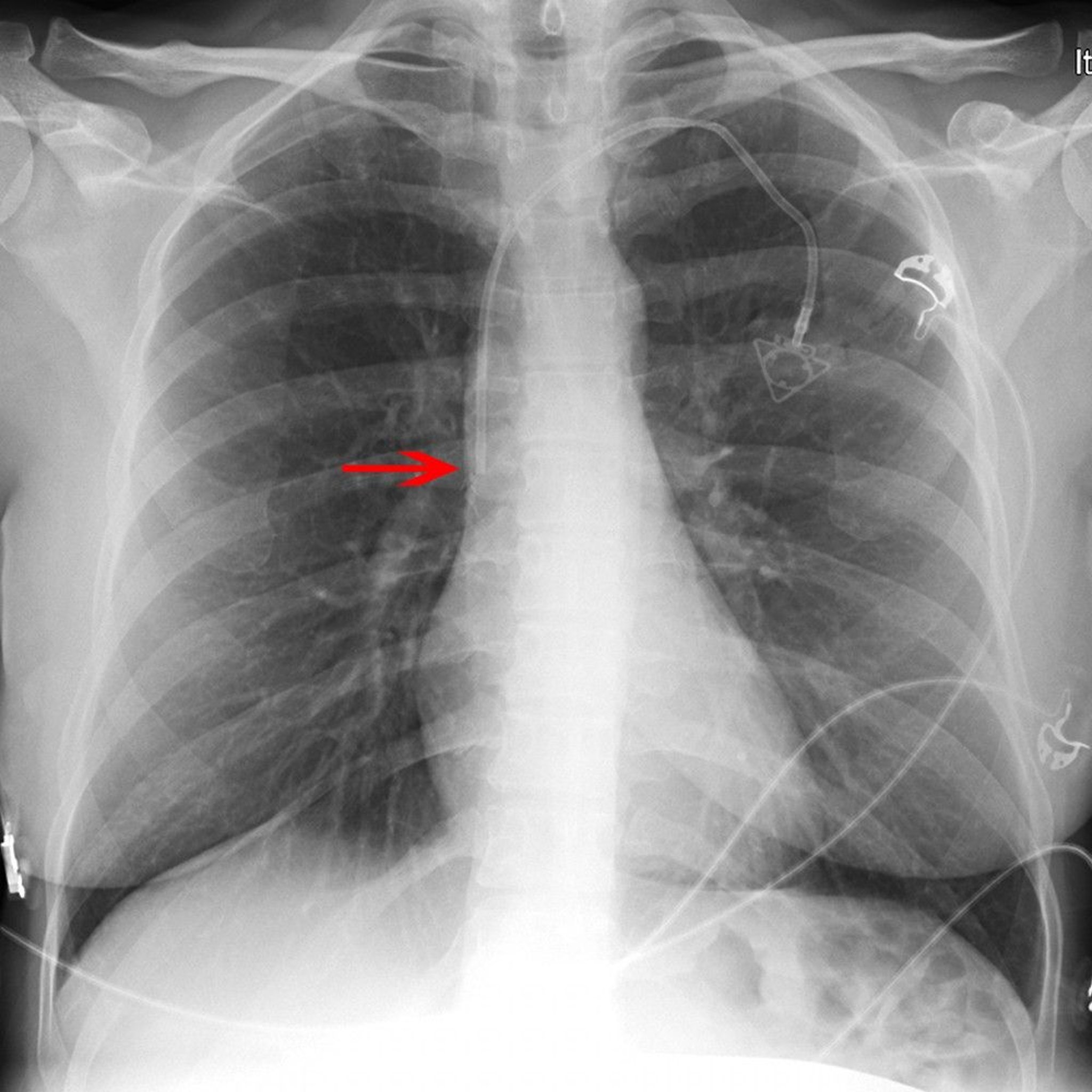
Complications of central venous catheterization
CVCs can cause many complications (see table Complications Associated With Central Venous Catheters). Pneumothorax occurs in 1% of patients after CVC insertion. Atrial or ventricular arrhythmias frequently occur during catheter insertion but are generally self-limited and subside when the guide wire or catheter is withdrawn from within the heart. The incidence of catheter bacterial colonization without systemic infection may be as high as 35%, whereas that of true sepsis is 2 to 8%. Catheter-related venous thrombosis is an increasingly recognized complication, particularly in the upper extremities. Rarely, accidental arterial catheterization requires surgical repair of the artery. Hydrothorax and hydromediastinum may occur when catheters are positioned extravascularly. Catheter damage to the tricuspid valve, bacterial endocarditis, and air and catheter embolism occur rarely.
To reduce the risk of venous thrombosis and catheter sepsis, clinicians should remove CVCs as soon as possible. The skin entry site must be cleansed and inspected daily for local infection; the catheter must be replaced if local or systemic infection occurs. Some clinicians feel it is beneficial to change CVC catheters at regular intervals (eg, every 5 to 7 days) in patients with sepsis who remain febrile; this approach may reduce the risk of bacterial colonization of the catheter.
(See also Guidelines for Prevention of Intravascular Catheter-Related Infections at the CDC web site.)
Midline Peripheral Catheterization
Midline catheters (MC) are 8 to 20 cm in length, have a single or double lumen, and are placed peripherally in the nondominant arm 1.5 cm above or below the antecubital fossa, into the basilic, cephalic, or brachial vein. Although placement of a MC requires use of the modified Seldinger technique and ultrasonographic guidance, MCs are not considered central venous catheters because the tip is located at or below the axillary vein. Thus, x-ray confirmation of correct placement of the MC tip is not necessary.
Criteria for using MCs:
Patients anticipated to require intermediate to long-term intravenous therapy
Patients who have poor venous access requiring multiple needlestick attempts or blood draws
Patients likely to require frequent blood draws to monitor their condition
MCs have been found to have lower phlebitis rates than peripheral catheters and lower infection rates than central venous catheters (1).
Arterial Catheterization
The use of automated noninvasive blood pressure devices has diminished the use of arterial catheters simply for pressure monitoring. However, these catheters are beneficial in unstable patients who require minute-to-minute pressure measurement and in those requiring frequent arterial blood gas sampling. Indications include refractory shock and respiratory failure. Blood pressure is frequently somewhat higher when measured by an arterial catheter than by sphygmomanometry. Initial upstroke, maximum systolic pressure, and pulse pressure increase the more distal the point of measurement, whereas the diastolic and mean arterial pressures decline. Vessel calcification, atherosclerosis, proximal occlusion, and extremity position can all affect the value of arterial catheter measurements.
For a step-by-step description of how to do arterial catheterization, see How To Do Radial Artery Cannulation and How To Do Radial Artery Cannulation, Ultrasound-Guided.

Video created by Hospital Procedures Consultants at www.hospitalprocedures.org.

Video created by Hospital Procedures Consultants at www.hospitalprocedures.org.

Video created by Hospital Procedures Consultants at www.hospitalprocedures.org.

Video created by Hospital Procedures Consultants at www.hospitalprocedures.org.

Video created by Hospital Procedures Consultants at www.hospitalprocedures.org.

Video created by Hospital Procedures Consultants at www.hospitalprocedures.org.
Complications of arterial catheterization
At all sites, complications include bleeding, infection, thrombosis, intimal dissection, and distal embolism. Catheters should be removed if signs of local or systemic infection are present.
Radial arterial complications include ischemia of the hand and forearm due to thrombosis or embolism, intimal dissection, or spasm at the site of catheterization. The risk of arterial thrombosis is higher in small arteries (explaining the greater incidence in women) and with increased duration of catheterization. Occluded arteries nearly always recanalize after catheter removal.
Femoral arterial complications include atheroembolism during guide wire insertion. The incidence of thrombosis and distal ischemia is much lower than that for radial arterial catheterization.
Axillary arterial complications include hematomas, which are infrequent but may require urgent care because brachial plexus compression can result in permanent peripheral neuropathy. Flushing the axillary arterial catheter may introduce air or a clot. To avoid neurologic sequelae of these emboli, clinicians should select the left axillary artery for catheterization (the left axillary artery branches further distal to the carotid vessels than does the right).
Catheterization reference
Alexandrou E, Ramjan L, Spencer T, et al: The use of midline catheters in the adult acute care setting – clinical implications and recommendations for practice. JAVA 16:35–41, 2011.
Intraosseous Infusion
Any fluid or substance routinely given IV (including blood products) may be given via a sturdy needle inserted in the medullary cavity of select long bones. Fluids reach the central circulation as quickly as with venous infusion. This technique is used more commonly in infants and young children, whose bony cortices are thin and easily penetrated and in whom peripheral and central venous access can be quite difficult, particularly in shock or cardiac arrest. However, this technique can be used in older patients at various sites (eg, sternum, proximal tibia, humerus) via special devices (eg, pressure-loaded puncture device, drilling device) that are now more readily available. Thus, intraosseous infusion is becoming more common in adults.
For a step-by-step description of how to do intraosseous cannulation, see How To Do Intraosseous Cannulation, Manually and With a Power Drill.
Procedure demonstrated by Eric Sanders, MD, EM-2. Walter A. Schrading, MD, FACEP, faculty supervisor. WellSpan York Hospital Emergency Medicine Residency Program York, PA. Cadaver specimens provided by Maryland State Anatomy Board, DHMH. Filmed on location at School of Medicine, Anatomical Services Division, Univ. of Maryland.
© Elsevier Inc. All Rights Reserved.
This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.
Procedure demonstrated by Eric Sanders, MD, EM-2. Walter A. Schrading, MD, FACEP, faculty supervisor. WellSpan York Hospital Emergency Medicine Residency Program York, PA. Cadaver specimens provided by Maryland State Anatomy Board, DHMH. Filmed on location at School of Medicine, Anatomical Services Division, Univ. of Maryland.

© Elsevier Inc. All Rights Reserved.
This video is for personal informational use. Users are prohibited from copying, reproducing, licensing, subscribing, selling, leasing or distributing this video.
Intraosseous (IO) needle insertion
The physician’s fingers and thumb are wrapped around the proximal tibia to stabilize it; the hand should not be placed directly behind the insertion site (to avoid self-puncture). Instead, a towel may be placed behind the knee to support it. The physician holds the needle firmly in the palm of the other hand, directing the point slightly away from the joint space and growth plate. The needle is inserted with moderate pressure and a rotary motion; it is stopped as soon as a pop indicates penetration of the cortex. Some needles have a plastic sleeve, which can be adjusted to prevent them from being pushed too deeply into or through the bone. |