


Cardiac tumors may be primary (benign or malignant) or metastatic (malignant). Myxoma, a benign tumor, is the most common type of primary cardiac tumor. Cardiac tumors may occur in any cardiac tissue. They can cause valvular or inflow-outflow tract obstruction, thromboembolism, arrhythmias, or pericardial disorders. Diagnosis is by echocardiography and frequently cardiac MRI. Treatment of benign tumors is usually surgical resection; tumors may recur. Treatment of metastatic cancer depends on tumor type and origin; prognosis is generally poor.
Primary cardiac tumors are found in < 1/2000 people at autopsy. Metastatic tumors are 30 to 40 times more common. Usually, primary cardiac tumors originate in the myocardium or endocardium; they may also originate in valve tissue, cardiac connective tissue, or the pericardium. Metastatic cardiac tumors typically originate from the lung. Other common sources of cardiac metastases include breast and kidney carcinoma, melanoma, and lymphoma.
Classification of Cardiac Tumors
Some of the more common primary and secondary cardiac tumors are listed (see Types of Cardiac Tumors). Primary cardiac tumors may be
Benign (nearly 80% of cases)
Malignant (the remaining 20%)
Benign primary cardiac tumors
Examples are myxomas, papillary fibroelastomas, rhabdomyomas, fibromas, hemangiomas, teratomas, lipomas, paragangliomas, and pericardial cysts.
Myxoma is most common, accounting for 50% of all primary cardiac tumors. Incidence in women is 2 to 4 times that in men. In uncommon familial forms (Carney complex), men are affected more often. About 75% of myxomas occur in the left atrium, and the rest occur in the other chambers as a solitary tumor or, less commonly, at several sites. Myxomas may be up to 15 cm in diameter. About 75% are pedunculated and may prolapse through the mitral valve and obstruct ventricular filling during diastole. The remainder of the tumors are broad-based and sessile. Myxomas may be myxoid and gelatinous; smooth, firm, and lobular; or friable and irregular. Friable, irregular myxomas increase risk of systemic embolism.
Carney complex is a familial, autosomal dominant syndrome of recurrent cardiac myxomas with some combination of cutaneous myxomas, myxoid mammary fibroadenomas, pigmented skin lesions (lentigines, ephelides, blue nevi), multiple endocrine neoplasia (primary pigmented nodular adrenocortical disease causing Cushing syndrome, growth hormone and prolactin-producing pituitary adenoma, testicular tumors, thyroid adenoma or carcinoma, and ovarian cysts), psammomatous melanotic schwannoma, breast ductal adenoma, and osteochondromyxoma. Patients are often young at presentation (median age, 20 years), have multiple myxomas (particularly in the ventricles), and have a higher risk of myxoma recurrence.
Papillary fibroelastomas are avascular papillomas that occur on heart valves in > 80% of cases. The papillomas are more likely to occur on the left side of the heart ), predominantly on the aortic and mitral valves. Men and women are affected equally. They have papillary fronds branching from a central core, resembling sea anemones. About 45% are pedunculated. They do not cause valvular dysfunction but increase risk of embolism.
Rhabdomyomas affect mainly infants and children, 80% of whom also have tuberous sclerosis. Rhabdomyomas are usually multiple and located intramurally in the septum or free wall of the left ventricle, where they affect the cardiac conduction system. They are firm, white lobules that typically regress with age. A minority of patients develop tachyarrhythmias and heart failure due to left ventricular outflow tract obstruction.
Fibromas occur mainly in children and are associated with adenoma sebaceum of the skin and kidney tumors. They occur primarily on the left side of the heart, are often located within the ventricular myocardium, and may develop in response to inflammation. They can compress or invade the cardiac conduction system, causing arrhythmias and sudden death. Some fibromas occur as part of a syndrome with generalized body overgrowth, jaw keratocytes, skeletal abnormalities, and various benign and malignant tumors (Gorlin, or basal cell nevus syndrome).
Hemangiomas cause symptoms in a minority of patients. Most often, they are incidentally detected during examinations done for other reasons.
Teratomas of the pericardium affect mainly infants and children. They are often attached to the base of the great vessels. About 90% are located in the anterior mediastinum; the rest, mainly in the posterior mediastinum.
Lipomas can develop at a wide range of ages. They originate in the endocardium or epicardium and have a large pedunculated base. Many are asymptomatic, but some obstruct flow or cause arrhythmias.
Paragangliomas, including pheochromocytomas, rarely occur in the heart; when they do, they are usually localized to the base of the heart near vagus nerve endings. They may manifest with symptoms due to catecholamine secretion (eg, increased heart rate and blood pressure, excessive sweating, tremor). Paragangliomas may be benign or malignant.
Pericardial cysts may resemble a cardiac tumor or pericardial effusion on chest x-ray. They are usually asymptomatic, although some cause compressive symptoms (eg, chest pain, dyspnea, cough).
Malignant primary cardiac tumors
Malignant primary tumors include sarcomas, pericardial mesothelioma, and primary lymphomas.
Sarcoma is the most common malignant cardiac tumor. Sarcomas affect mainly middle-aged adults (mean, 44 years). Almost 40% are angiosarcomas, most of which originate in the right atrium and involve the pericardium, causing right ventricular inflow tract obstruction, pericardial tamponade, and lung metastasis. Other types include undifferentiated sarcoma, malignant fibrous histiocytoma, leiomyosarcoma, fibrosarcoma, rhabdomyosarcoma, liposarcoma, and osteosarcoma; these types are more likely to originate in the left atrium, causing mitral valve obstruction and heart failure.
Pericardial mesothelioma is rare. It affects all ages, males more than females. It causes cardiac tamponade and constriction, and can metastasize to the spine, adjacent soft tissues, and brain.
Primary lymphoma is extremely rare. It usually occurs in patients with HIV/AIDS or other people with immunodeficiency. These tumors grow rapidly and cause heart failure, arrhythmias, cardiac tamponade, and superior vena cava (SVC) syndrome.
Metastatic tumors
Melanoma is a tumor with a high propensity for cardiac involvement. Lung and breast carcinoma, soft-tissue sarcoma, and renal cancer are also common sources of metastases to the heart (1). Leukemia and lymphoma often metastasize to the heart, but cardiac involvement is often clinically silent and detected incidentally. When Kaposi sarcoma spreads systemically in immunodeficient (usually AIDS) patients, it may spread to the heart, but clinical cardiac complications are uncommon.
Classification reference
1. Klatt EC, Heitz DR: Cardiac metastases. Cancer 65:1456‒1459, 1990.
Symptoms and Signs of Cardiac Tumors
Cardiac tumors cause symptoms and signs typical of much more common disorders (eg, heart failure, stroke, coronary artery disease). Symptoms and signs of benign primary cardiac tumors depend on tumor type, location, size, and friability.
Types of symptoms and signs
Symptoms can be classified as
Extracardiac
Intramyocardial
Intracavitary
Extracardiac symptoms and signs may be constitutional or mechanical. Constitutional symptoms of fever, chills, lethargy, arthralgias, and weight loss are caused exclusively by myxomas, perhaps as a result of cytokine (eg, interleukin-6) release. Petechiae may also occur. These and other findings may erroneously suggest bacterial endocarditis, connective tissue disorders, or occult cancer. With some tumors (especially gelatinous myxomas), thrombi or tumor fragments may embolize into the systemic circulation (eg, brain, coronary arteries, kidneys, spleen, extremities) or the lungs and cause manifestations specific to those organs. Mechanical symptoms (eg, dyspnea, chest discomfort) result from compression of cardiac chambers or coronary arteries or from pericardial irritation or tamponade caused by growth or hemorrhage within the pericardium. Pericardial tumors may cause pericardial friction rubs.
Intramyocardial symptoms and signs are caused by arrhythmias, usually atrioventricular or intraventricular block or paroxysmal supraventricular or ventricular tachycardias due to compression or encroachment on the conduction system (notably rhabdomyomas and fibromas).
Intracavitary symptoms and signs are due to tumors that obstruct valvular function, blood flow, or both (causing valvular stenosis, valvular insufficiency, or heart failure). Intracavitary symptoms and signs may vary with body position, which can alter hemodynamics and physical forces associated with the tumor.
Symptoms and signs by tumor type
Myxomas may manifest with the triad of heart failure, embolic disease, and constitutional symptoms. Myxomas may cause a diastolic murmur that mimics the murmur of mitral stenosis but whose loudness and location vary from beat to beat with body position. About 15% of pedunculated left atrial myxomas produce an audible “tumor plop” as they drop into the mitral orifice during diastole. Myxomas may also cause arrhythmias. Raynaud syndrome and finger clubbing are less typical but may occur.
Fibroelastomas, often discovered incidentally at autopsy, are usually asymptomatic; however, they may be a source of systemic emboli.
Rhabdomyomas are usually asymptomatic.
Fibromas cause arrhythmias, possibly causing sudden death, and obstructive symptoms.
Hemangiomas are usually asymptomatic but may cause any of the extracardiac, intramyocardial, or intracavitary symptoms.
Teratomas cause respiratory distress and cyanosis due to compression of the aortic and pulmonary artery, or SVC syndrome due to compression of the superior vena cava.
Symptoms and signs of malignant cardiac tumors are more acute in onset and progress more rapidly than those of benign tumors. Cardiac sarcomas most commonly cause symptoms of ventricular inflow tract obstruction and pericardial tamponade. Mesothelioma causes symptoms of pericarditis or tamponade. Primary lymphoma causes refractory progressive heart failure, tamponade, arrhythmias, and SVC syndrome. Metastatic cardiac tumors may manifest as sudden cardiac enlargement, tamponade (due to rapid accumulation of hemorrhagic pericardial effusion), heart block, other arrhythmias, or sudden unexplained heart failure. Fever, malaise, weight loss, night sweats, and loss of appetite may also be present.
Diagnosis of Cardiac Tumors
Echocardiography
Cardiac MRI
Cardiac CT
Diagnosis, which is often delayed because symptoms and signs mimic those of much more common disorders, is confirmed by echocardiography. Transesophageal echocardiography is better for visualizing atrial tumors, and transthoracic echocardiography is better for ventricular tumors.

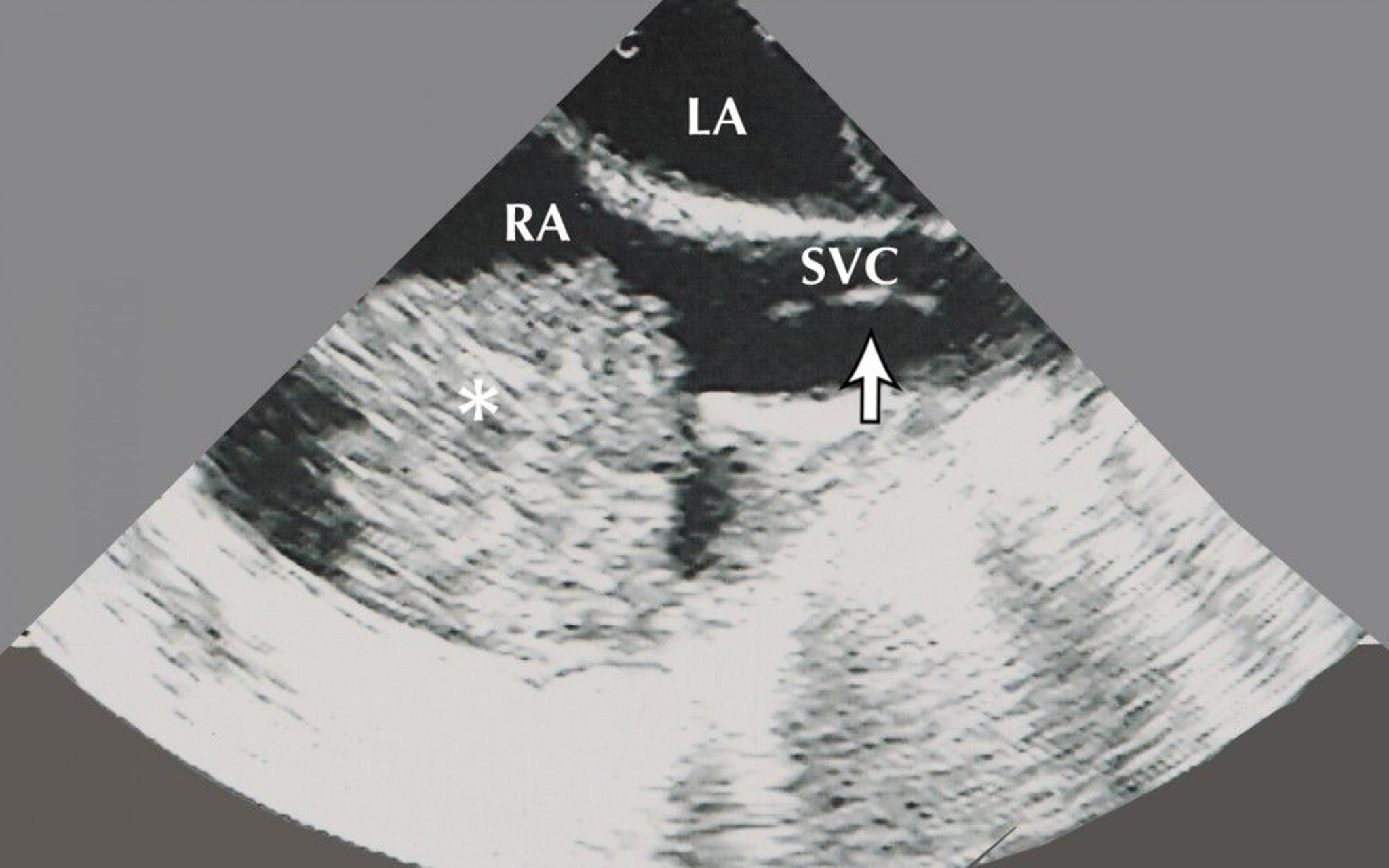
© Springer Science+Business Media
Cardiac MRI is frequently used to identify tumor tissue characteristics and provide clues to tumor type. If results are equivocal, gated radionuclide imaging and CT may be helpful.

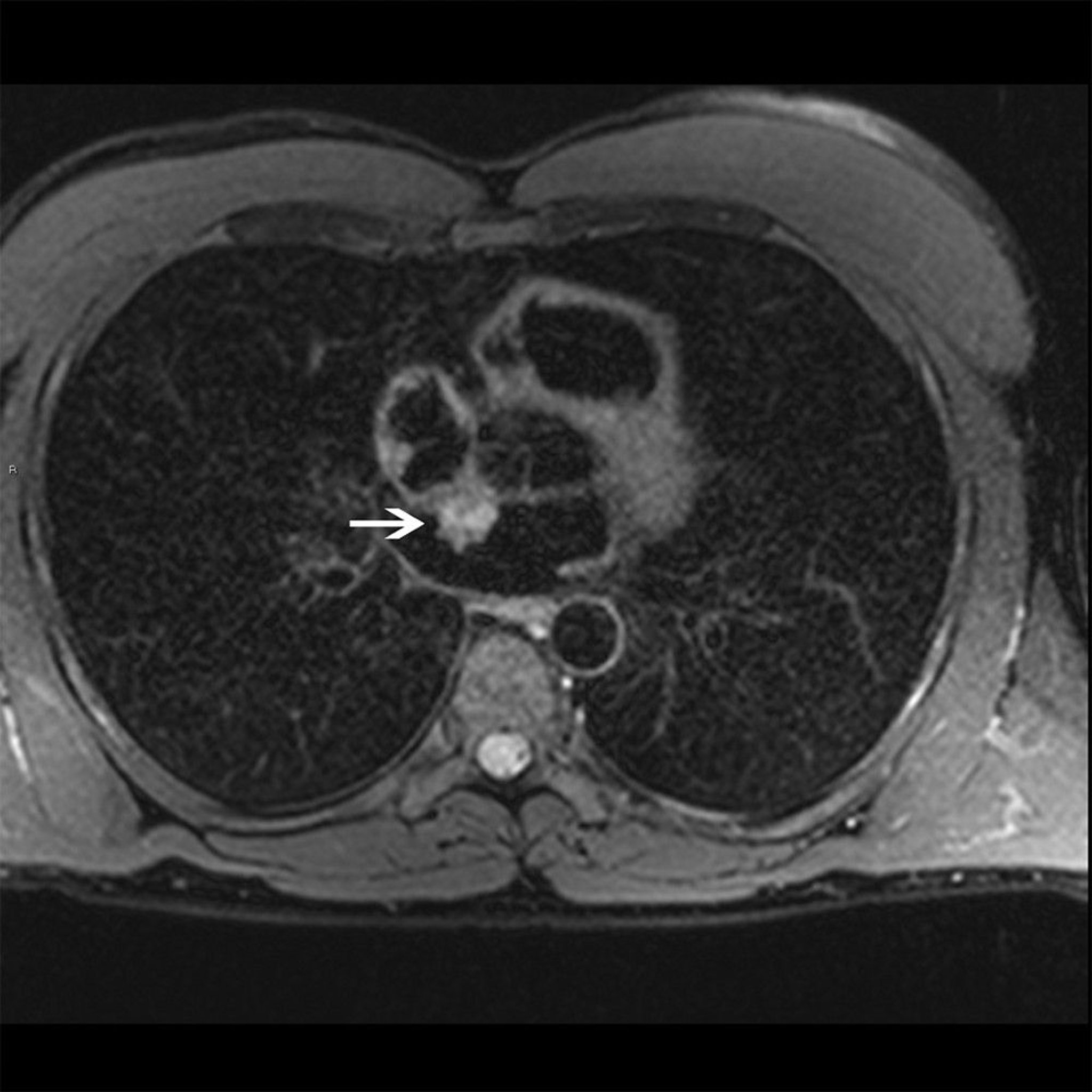
© 2017 Elliot K. Fishman, MD.
Contrast-enhanced cardiac CT can provide detailed information with superior spatial resolution compared to other techniques.
Biopsy is not usually done because imaging studies can often distinguish benign from malignant tumors, and biopsy may inadvertently spread cancerous cells in patients with a malignant primary tumor.
Extensive testing often precedes echocardiography in patients with myxomas because their symptoms are nonspecific. Anemia; thrombocytopenia; and elevation of white blood cell count, erythrocyte sedimentation rate, C-reactive protein, and gamma-globulins are common. ECG may show left atrial enlargement. Routine chest x-ray may show calcium deposits in right atrial myxomas or in teratomas seen as anterior mediastinal masses. Myxomas are sometimes diagnosed when tumor cells are found in a surgically removed embolus.
Arrhythmias and heart failure in patients with features of tuberous sclerosis suggest rhabdomyomas or fibromas. New cardiac symptoms and signs in a patient with a known extracardiac cancer suggest cardiac metastases. Chest x-ray may show bizarre changes in the cardiac silhouette.
Treatment of Cardiac Tumors
Benign primary: Excision
Malignant primary: Palliation
Metastatic: Depends on tumor origin
Treatment of benign primary tumors is surgical excision followed by serial echocardiography over 5 to 6 years to monitor for recurrence. Tumors are excised unless another disorder (eg, dementia) contraindicates surgery. Surgery is usually curative (95% survival at 3 years). Exceptions are rhabdomyomas, most of which regress spontaneously and do not require treatment, and pericardial teratoma, which may require urgent pericardiocentesis. Patients with fibroelastoma may also require valvular repair or replacement. When rhabdomyomas or fibromas are multifocal, surgical excision is usually ineffective, and prognosis is poor after the first year of life; survival at 5 years may be as low as 15%.
Treatment of malignant primary tumors is usually palliative (eg, radiation therapy, chemotherapy, management of complications) because prognosis is poor.
Treatment of metastatic cardiac tumors depends on tumor origin. It may include systemic chemotherapy or palliation.
Key Points
Most cardiac tumors are metastatic, most commonly from lung and breast carcinoma, melanoma, soft-tissue sarcoma, and renal carcinoma.
Primary cardiac tumors are much less common; most originate in the myocardium or endocardium but they can develop in any cardiac tissue and be benign or malignant.
Manifestations depend on the location and type of tumor but include constitutional symptoms, valvular or inflow-outflow tract obstruction, thromboembolism, and arrhythmias.
Diagnosis is by echocardiography, and frequently cardiac MRI.
For benign tumors, treatment is excision; for malignant primary and most metastatic tumors, treatment is palliative.




