




Pelvic organ prolapse involves relaxation or weakening of the ligaments, connective tissue, and muscles of the pelvis, causing the bladder, urethra, small intestine, rectum, or uterus to bulge into the vagina.
Women may feel pressure that feels as if something is bulging out of their vagina or they are sitting on a ball, or they may have a sense of fullness in their pelvis or problems with urination or bowel movements.
A pelvic examination is done while a woman bears down to make abnormalities more obvious.
Pelvic muscle exercises and pessaries may help, but surgery may be needed.
Pelvic organ prolapse occurs only in women and become more common as women age. During their lifetime, about 1 of 11 women has surgery for pelvic organ prolapse.
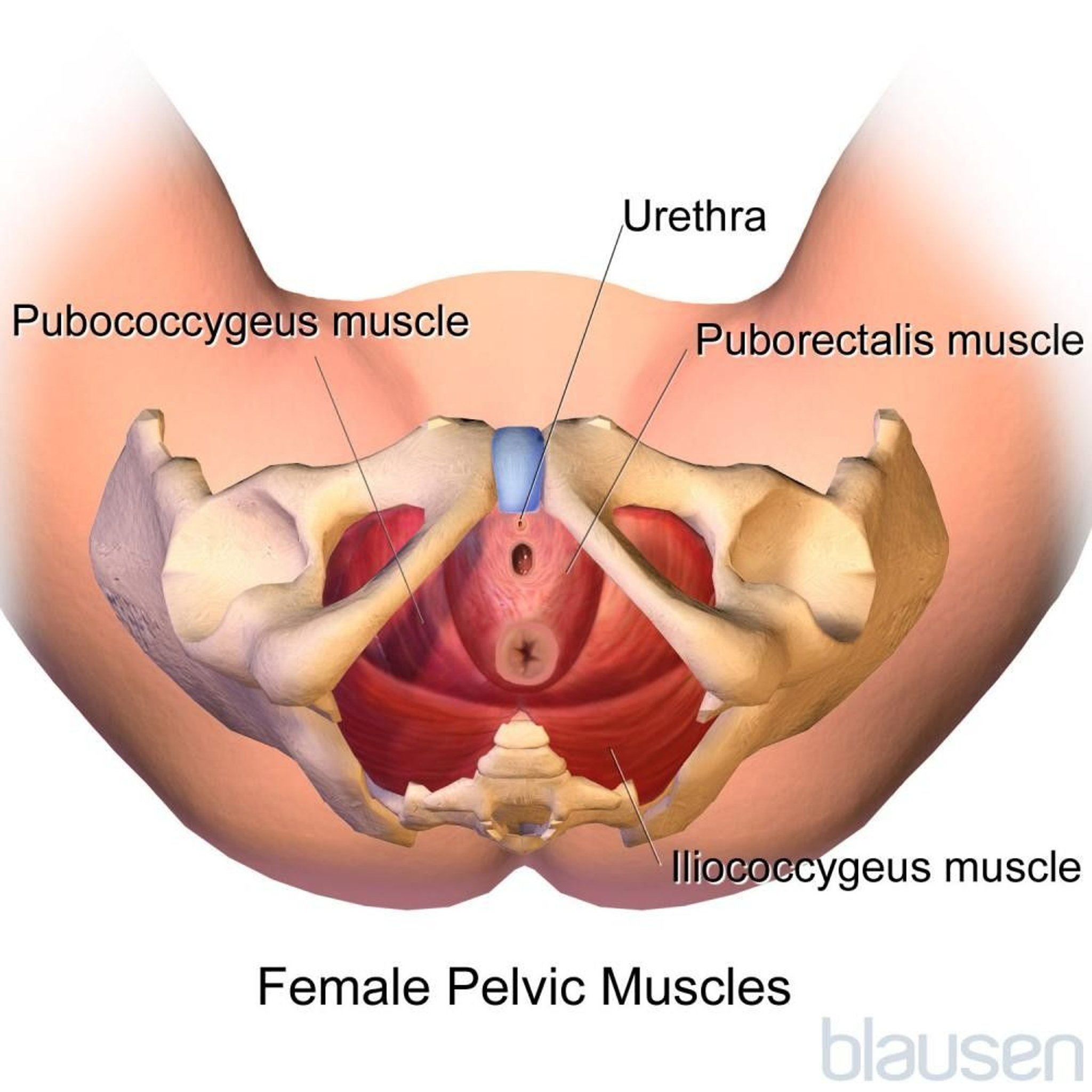
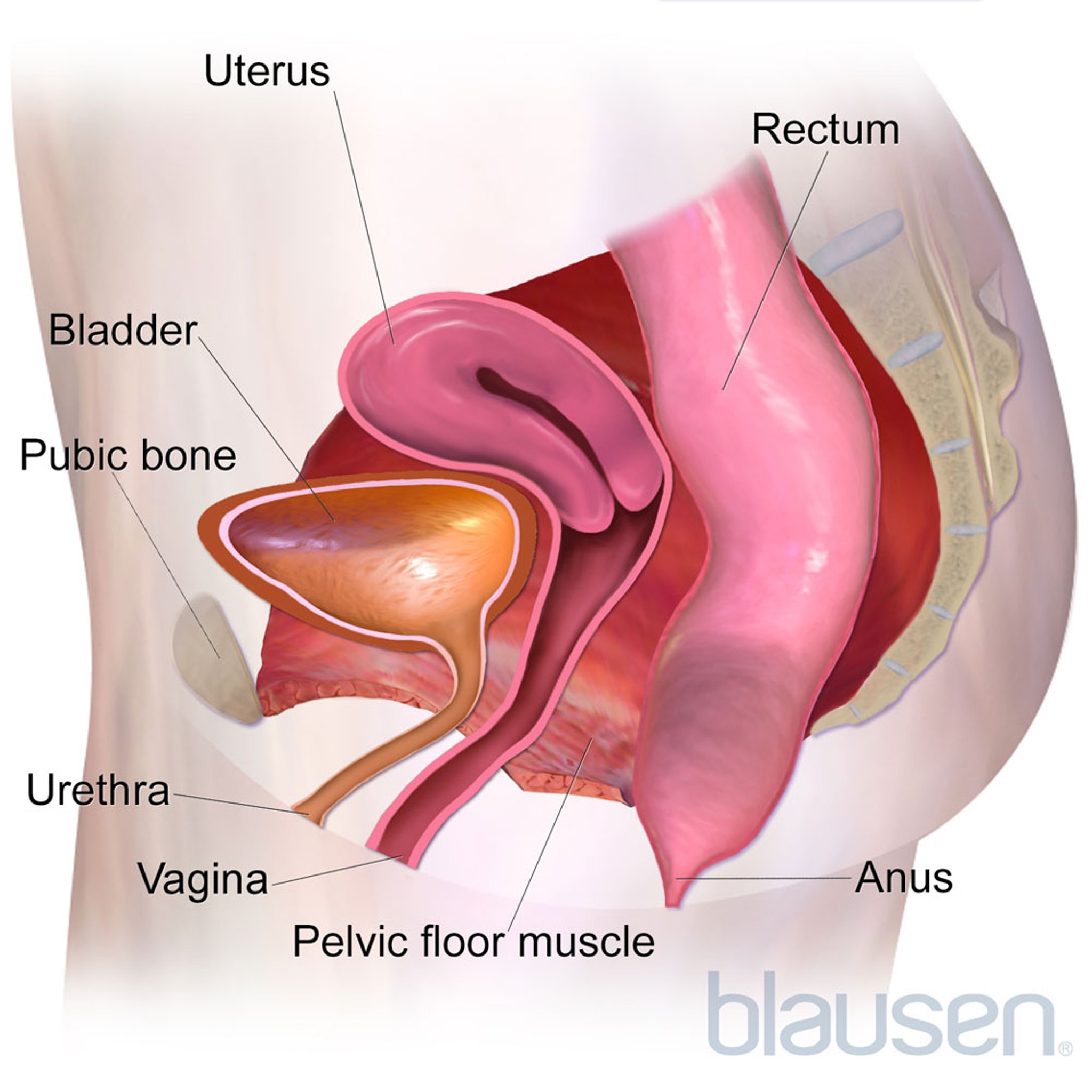
The pelvic floor is a network of muscles, ligaments, and tissues that act like a hammock to support the organs of the pelvis: the uterus, vagina, bladder, urethra, and rectum. If the muscles become weak or the ligaments or tissues are stretched or damaged, the pelvic organs or small intestine may drop down and protrude (prolapse) into the vagina. If the disorder is severe, the organs may protrude all the way through the opening of the vagina and outside the body.

Pelvic organ prolapse usually results from a combination of factors.
The following factors commonly contribute to development of pelvic organ prolapse:
Having a baby, particularly if the baby is delivered vaginally
Having obesity
Having an injury, as may occur during hysterectomy (removal of the uterus) or another surgical procedure
Aging
Frequently doing things that increase pressure in the abdomen, such as straining during bowel movements or lifting heavy objects
Being pregnant and having a vaginal delivery may weaken or stretch some of the supporting structures in the pelvis. Pelvic organ prolapse is more common among women who have had several vaginal deliveries, and the risk increases with each delivery. The pregnancy or the delivery may damage nerves, leading to muscle weakness. The risk of developing pelvic organ prolapse may be less with a cesarean delivery than with a vaginal delivery.
As women age, the supporting structures in the pelvis may weaken, even if a woman has never been pregnant. As a result, pelvic organ prolapse is more likely to develop.
Having a hysterectomy may also weaken the structures in the pelvis, increasing the risk of pelvic organ prolapse.
Increased pressure on the pelvic floor for a long time, usually many years, may also contribute to pelvic organ prolapse. Frequently straining the pelvic area (for example, because of constipation), having a chronic cough, or frequently lifting heavy object can increase this pressure.
Less common factors that may contribute to pelvic organ prolapse include disorders that increase pressure in the abdomen and thus on pelvic organs, such as accumulation of fluid within the abdomen (ascites) and tumors in the abdomen. Disorders of nerves to the pelvic floor and disorders of connective tissue may also contribute. (Connective tissue is the tough, often fibrous tissue that is present in almost every organ, including muscles, and that provides support and elasticity.) Rarely, women have birth defects that affect this area or are born with weak pelvic tissues.
Types and Symptoms
Pelvic organ prolapse is essentially a hernia (an opening or weak area in tissue), through which organs protrude abnormally because supporting tissue is weakened.
The different types of pelvic organ prolapse are named according to the organ affected.
The back wall of the vagina: Prolapse of the rectum (rectocele) or small intestine (enterocele)
The front wall of the vagina: Prolapse of the bladder (cystocele) or urethra (urethrocele)
The top of the vagina: Vaginal (apical) prolapse
The uterus: Prolapse of the uterus (uterine prolapse)
Often, a woman has more than one type. In all types, the most common symptom is a feeling of heaviness, fullness, or pressure in the area of the vagina. A woman may feel as if she is sitting on a ball or that the uterus, bladder, or rectum is bulging or dropping out of her vagina.
When the Bottom Falls Out: Prolapse in the Pelvis

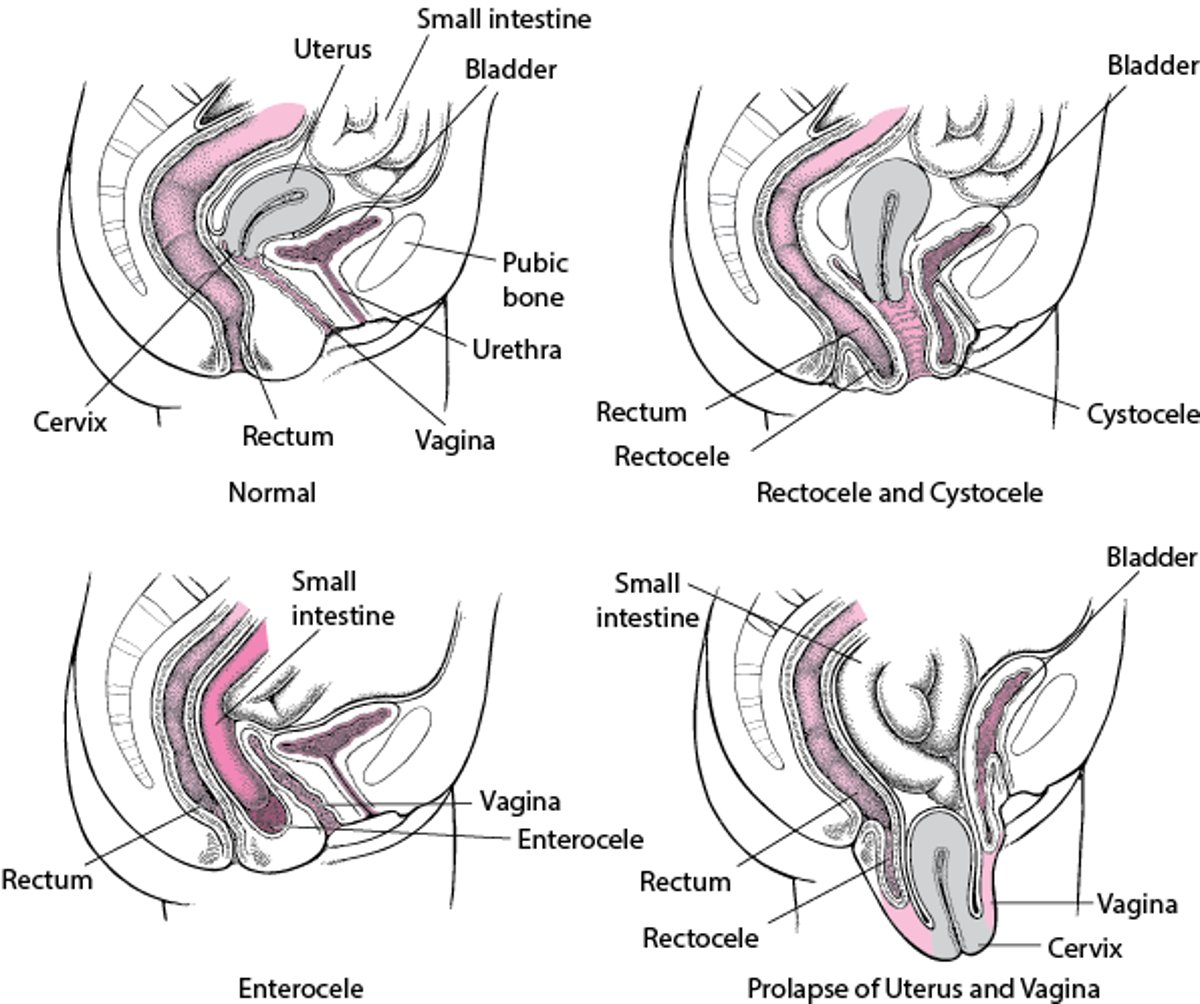
Symptoms tend to occur when women are standing or sitting upright, straining, or coughing and to disappear when they are lying down and relaxing. For some women, sexual intercourse is painful.
Mild cases may not cause symptoms until the woman becomes older.
Prolapse of the rectum (rectocele), small intestine (enterocele), bladder (cystocele), and urethra (urethrocele) are particularly likely to occur together. A urethrocele and cystocele almost always occur together.
Damage to the pelvic floor may affect the urinary tract. As a result, women who have pelvic organ prolapse may have problems controlling urination, resulting in urine leaking out involuntarily (urinary incontinence) or problems completely emptying the bladder (urinary retention).
Cystocele and cystourethrocele
A cystocele develops when the bladder drops down and protrudes into the front wall of the vagina. It results from weakening of the connective tissue and supporting structures around the bladder. When a urethrocele and cystocele occur together, they are called a cystourethrocele.
Women with either of these disorders may have urinary incontinence.
Rectocele
A rectocele develops when the rectum drops down and protrudes into the back wall of the vagina. It results from weakening of the muscular wall of the rectum and the connective tissue around the rectum.
A rectocele can make having a bowel movement difficult and may cause constipation. Women may be unable to empty their bowels completely. Some women need to place a finger in their vagina and press against the rectum to have a bowel movement.
Enterocele
An enterocele develops when the small intestine and the lining of the abdominal cavity (peritoneum) bulge downward between the vagina and the rectum. It occurs most often after the uterus has been surgically removed (hysterectomy). An enterocele results from weakening of the connective tissue and ligaments supporting the uterus or vagina.
An enterocele often causes no symptoms. But some women feel a sense of fullness or pressure or pain in the pelvis. Pain may also be felt in the lower back.
Prolapse of the uterus
In prolapse of the uterus, the uterus drops down into the vagina. It usually results from weakening of the connective tissue and ligaments supporting the uterus. The uterus may bulge in the following ways:
Only into the upper part of the vagina
Down to the opening of the vagina
Partly through the opening
All the way through the opening, resulting in total uterine prolapse (procidentia)
How far down the uterus drops down determines how severe symptoms are.
At first, prolapse of the uterus may cause mild or no symptoms. When prolapses worsens, the first symptom most women report is feeling a bulge at the opening of the vagina. They may also have pain in the lower back or over the tailbone, difficulty having a bowel movement, and pain during sexual intercourse, as well as a feeling of heaviness or pressure—a feeling that pelvic organs are dropping out.
Total uterine prolapse can cause pain during walking. Sores may develop on the protruding cervix (the lower part of the uterus) and cause bleeding, a discharge, and infection.
Women may have problems controlling urination, resulting in urine leaking out involuntarily (urinary incontinence). Or women may not be able to empty their bladder completely or to urinate (urinary retention).
Constipation can occur.
Prolapse of the vagina
In prolapse of the vagina, the upper part of the vagina drops down into the lower part, so that the vagina turns inside out. The upper part may drop part way through the vagina or all the way through, protruding outside the body and causing total vaginal prolapse. Usually, a cystocele or rectocele is also present.
Total vaginal prolapse may cause pain while sitting or walking. Sores may develop on the protruding vagina and cause bleeding and a discharge. Like prolapse of the uterus, prolapse of the vagina can cause problems with urination. Having a bowel movement may also be difficult.
Diagnosis of Pelvic Organ Prolapse
A pelvic examination
Doctors can usually diagnose pelvic organ prolapse by doing a pelvic examination with a speculum (an instrument that spreads the walls of the vagina apart). A doctor may insert one finger in the vagina and one finger in the rectum at the same time to determine how severe a rectocele or enterocele is.
A woman may be asked to bear down (as when having a bowel movement) or to cough. She may be examined while standing with one foot on a stool. The resulting pressure in the pelvis from bearing down, coughing, and/or standing may make a pelvic organ prolapse more obvious.
Procedures to determine how well the bladder and rectum are functioning may be done. For example, doctors often measure the amount of urine that the bladder can hold without leaking, the amount of urine left in the bladder after urination, and the rate of urine flow. If a woman has a problem with the passage of urine or urinary incontinence, doctors may use a flexible viewing tube to view the inside of the bladder (a procedure called cystoscopy) or the urethra (a procedure called urethroscopy). These procedures help doctors determine whether drugs or surgery is the best treatment. If the bladder is not functioning well, women are more likely to need surgery.
Rarely, if there are sores in the vagina or on the cervix, doctors may need to take a sample and examine it to help them determine what treatment is needed and whether cancer is present.
Treatment of Pelvic Organ Prolapse
Observation
Pelvic floor exercises
A pessary
Surgery
Treatment of pelvic organ prolapse is based on the woman's symptoms. Treatment aims to improve quality of life.
Doctors start by closely monitoring the woman and her symptoms.
If symptoms are bothersome, treatment may include pelvic floor exercises, a pessary, and, if symptoms are severe, surgery. If women do not have symptoms or symptoms are mild, no treatment is needed. However, follow-up visits are needed to monitor the progression of the prolapse.
Doctors also treat problems with completely emptying the bladder (urinary retention) or urinary incontinence.
Exercises
Pelvic floor exercises, such as Kegel exercises, can lessen bothersome symptoms, including stress incontinence, but do not affect prolapse itself. They tend to be most helpful if prolapse is mild.
These exercises help by strengthening the pelvic floor muscles. Kegel exercises target the muscles around the vagina, urethra, and rectum—the muscles used to stop a stream of urine. These muscles are tightly squeezed, held tight for about 1 or 2 seconds, then relaxed for about 10 seconds. Gradually, contractions are lengthened to about 10 seconds each. The exercise is repeated about 10 times in a row. Doing the exercises several times a day is recommended. Women can do Kegel exercises when sitting, standing, or lying down.
Some women have difficulty contracting the correct muscles. To determine whether they are contracting the correct muscles, women can contract pelvic floor muscles two or three times while urinating. If they contract the correct muscles, the flow of urine stops in midstream. If women need additional help, pelvic floor physical therapy may be recommended.
Pelvic floor therapy includes techniques that make learning the exercises easier, such as the following:
Cone-shaped inserts placed in the vagina, which help women focus on contracting the correct muscle
Biofeedback devices, which may use special sensors that show pelvic floor muscle contractions on a computer screen
Electrical stimulation (a health care practitioner inserts a probe, which transmits an electrical current to make the correct muscle contract)
Pessaries
If prolapse is causing symptoms, a device called a pessary may be inserted into the vagina to support the pelvic organs. Pessaries are especially useful for women who are waiting for surgery or who do not want or cannot have surgery. The pessary can lessen symptoms but is not a cure.
A pessary is usually made of silicone. They may be shaped like a diaphragm, cube, or doughnut. Some can be inflated. A doctor fits the pessary to the woman by inserting and removing different sizes until the right size is found. In some countries, pessaries may be available over the counter.
A pessary must be periodically removed and cleaned with soap and water. Women are taught how to insert and remove the pessary for cleaning. If they prefer or if they are unable to clean and replace the pessary themselves, they may go to the doctor's office periodically to have the pessary cleaned. Some pessaries should be removed during intercourse. Also, women may choose to remove them during intercourse. Women should also leave the pessary out overnight at regular intervals as recommended by their doctor.
Pessaries sometimes irritate the vaginal tissues and cause a foul-smelling discharge. The discharge can sometimes be controlled by regularly cleaning the pessary, changing the type of pessary, or using a vaginal jelly. Some doctors recommend using an estrogen cream to control the discharge.
Women who use a pessary should see their doctor periodically as their doctor recommends.
Surgery
Surgery is done if symptoms persist after women have tried pelvic floor exercises and a pessary. Surgery is also an option for women who do not wish to use a pessary. Surgery is usually done only after a woman has decided not to have any more children.
One of the following types of surgery is used:
Vaginal surgery: Surgery is done through the vagina rather than the abdomen. In such cases, no external incision is needed.
Abdominal surgery: One or more incisions are made in the abdomen.
Abdominal surgery includes the following:
Laparotomy: An incision that is several inches long is made in the abdomen.
Laparoscopic surgery: A viewing tube (laparoscope) and surgical instruments are inserted through several tiny incisions in the lower part of the abdomen.
The weakened area is located, and the tissues around it are built up to prevent the organ from dropping through the weakened area.
For rectoceles, enteroceles, cystoceles, and cystourethroceles, procedures may include the following:
Repair of the tissues that normally support the vagina (colporrhaphy).
Repair of the tissues between the opening of the vagina and the anus (perineorrhaphy).
For these two procedures, surgery is done through the vagina. These procedures do not require an incision in the abdomen.
For severe prolapse of the uterus or vagina, treatment may include
Removal of the uterus, if still present (hysterectomy)
Repair of the tissues that support the uterus and vagina (colporrhaphy)
Repair the tissues between the opening of the vagina and the anus (perineorrhaphy)
Attachment of the upper part of the vagina (with stitches) to a nearby stable structure, such as a bone or strong ligament in the pelvis (sacrospinous ligament fixation)
Closure of the vagina (colpocleisis) after removal of the uterus or with the uterus in place (called the Le Fort procedure)
Surgery is delayed until any sores on the protruding vagina have healed.
Closure of the vagina (colpocleisis) is an option for women who have severe vaginal prolapse and who do not plan to be sexually active. For this procedure, part of the vagina's lining is removed, and the vagina is stitched shut. Because this procedure can be done quickly and causes few complications, it may be a good choice for women who have conditions that make surgery risky (such as a heart disorder). Also, after closure, prolapse is unlikely to recur. However, vaginal intercourse is no longer possible.
After surgery to correct a pelvic organ prolapse, a catheter may be inserted in the bladder until the bladder starts functioning normally. Ideally, the catheter is removed within 24 hours.
Recovery time depends on the type of surgery. Most women can gradually resume their normal physical activity over a period of a few weeks, depending on the surgery. Lifting heavy objects (more than 10 pounds) may interfere with healing and should be avoided for at least 6 weeks after surgery to correct pelvic organ prolapse.




