




Vulvar cancer usually develops in the labia, the tissue that surrounds the opening of the vagina.
The cancer may appear to be a lump, an itchy area, or a sore that does not heal.
A sample of the abnormal tissue is removed and examined (biopsied).
All or part of the vulva and any other affected areas are removed surgically.
Reconstructive surgery can help improve appearance and function.
(See also Overview of Female Reproductive System Cancers.)
In the United States, cancer of the vulva (vulvar carcinoma) is the fourth most common gynecologic cancer, accounting for 5% of these cancers. Vulvar cancer usually occurs after menopause. The average age at diagnosis is 70 years. As more women live longer, this cancer is likely to become more common. Recent evidence suggests that vulvar cancer is becoming more common among younger women.
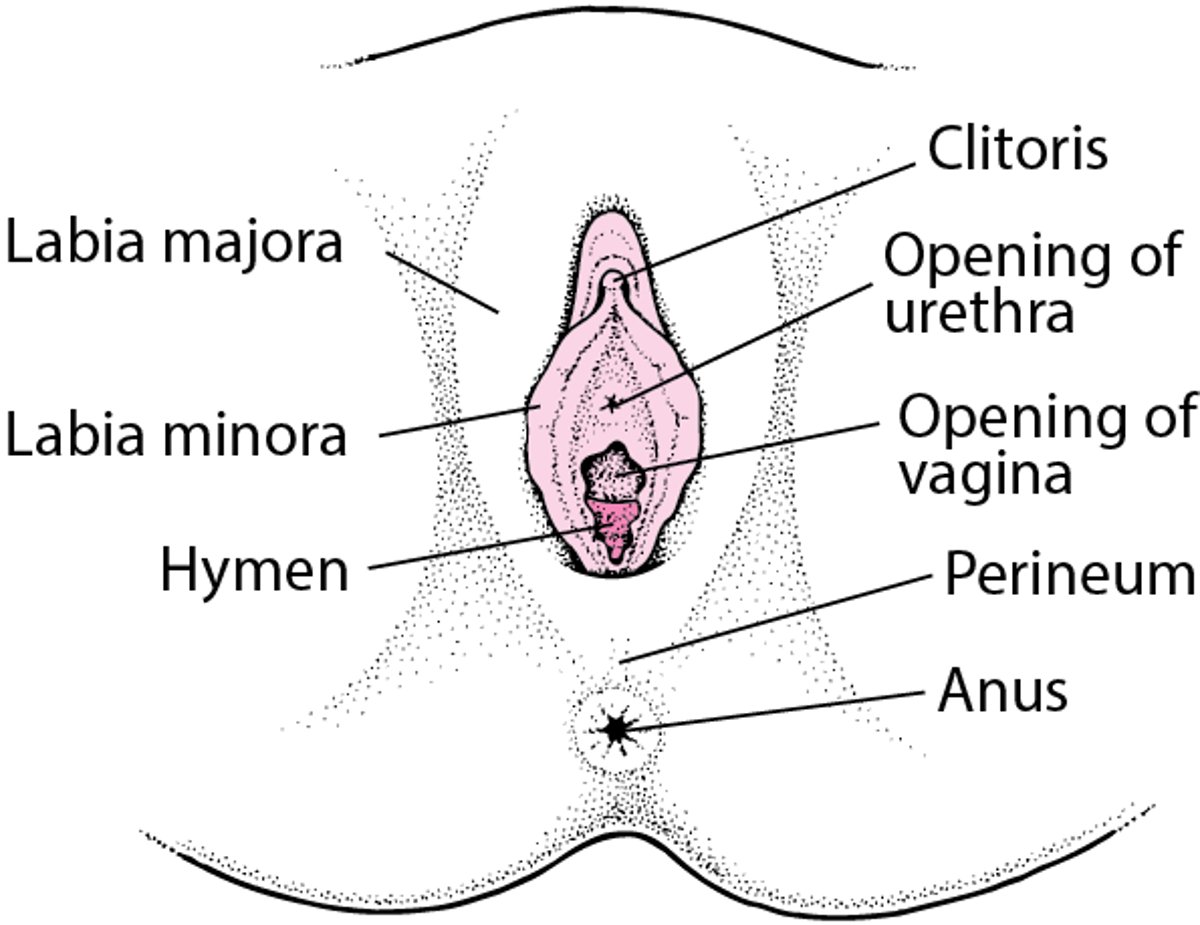
The vulva refers to the area around the opening of the vagina. It contains the external female reproductive organs.
Locating the Vulva

Vulvar cancer usually develops slowly over a number of years.
Most vulvar cancers are cancers of the skin that covers the labia, which surround the opening of the vagina. Approximately 90% of vulvar cancers are squamous cell carcinomas, which develop in the flat cells that form the outermost layer of skin, and 5% are melanomas, which develop in the pigment-producing cells of the skin (melanocytes). The remaining 5% include adenocarcinomas (which develop from gland cells), basal cell carcinomas (which rarely spread), and rare cancers such as Bartholin gland cancer. (Bartholin glands are very small, round glands located deep in the vulva on either side of the opening to the vagina.)
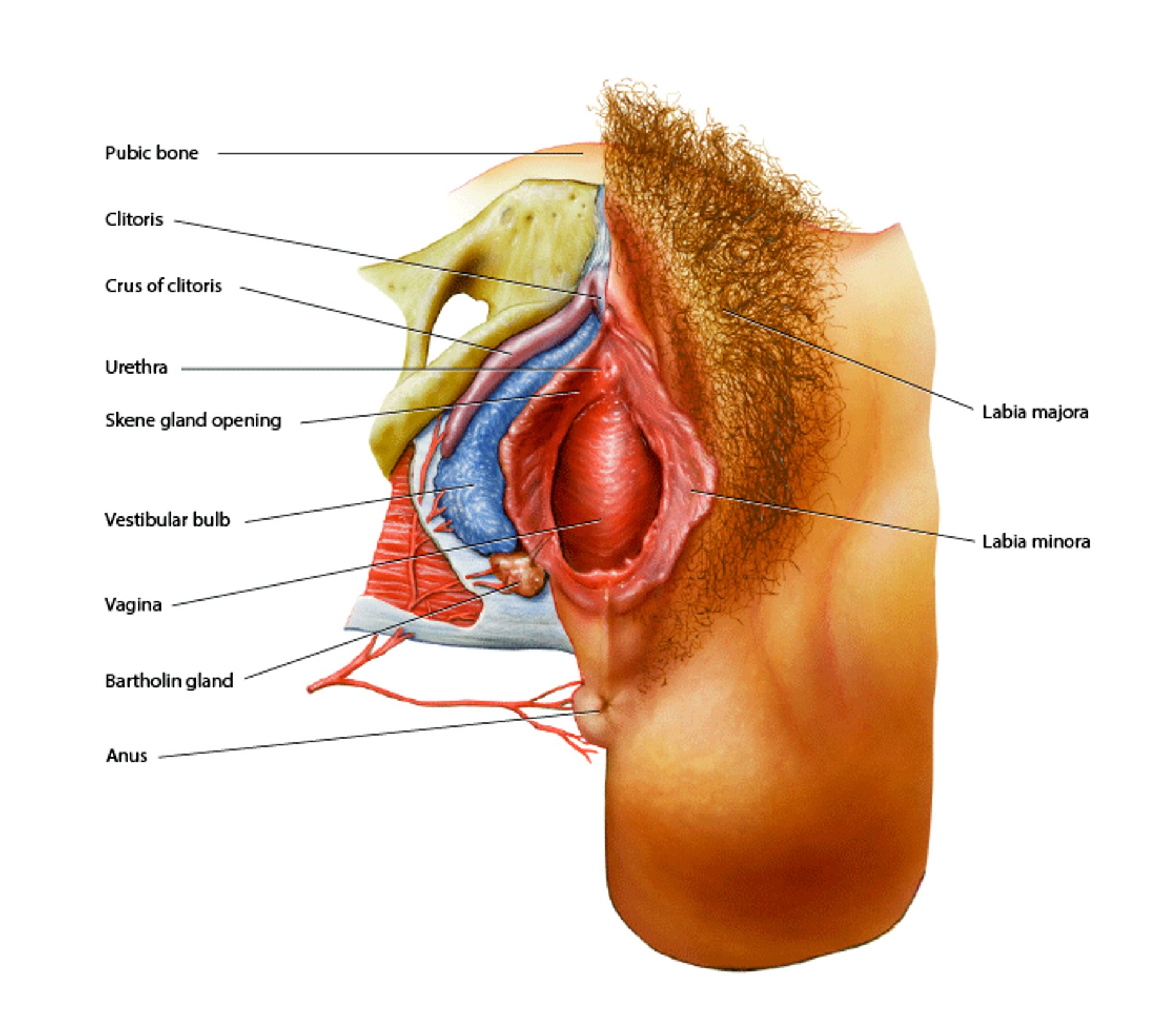
External Female Genital Anatomy
At the center of this image is the vagina, a canal composed of smooth muscle. The small opening directly above it is the urethra, which is the opening from the bladder. Below the vagina is the anus. Above the urethra is the clitoris, a body of erectile tissue that is homologous to the penis. The vagina is surrounded by the labia minora, which are surrounded by the labia majora. The pubic bone is at top. The purple tissue is a continuation of the clitoris, the crus of clitoris. The bulb of the vestibule (blue) also consists of erectile tissue. Below the bulb is a Bartholin gland, which secretes mucus to lubricate the vagina. BO VEISLAND/SCIENCE PHOTO LIBRARY |

Vulvar cancer begins on the surface of the vulva. Most of these cancers grow slowly, remaining on the surface for years. However, some (for example, melanomas) grow quickly. Untreated, vulvar cancer can eventually invade the vagina, the urethra, or the anus and spread into lymph nodes in the pelvis and abdomen and into the bloodstream.
Risk Factors for Vulvar Cancer
The risk of developing vulvar cancer is increased by the following:
Precancerous changes (vulvar intraepithelial neoplasia or dysplasia) in vulvar tissues
Cigarette smoking
Lichen sclerosus, which causes persistent itching and scarring of the vulva
A weakened immune system (due to a disorder such as cancer or AIDS or to medications such as chemotherapy drugs or corticosteroids)
Chronic granulomatous disease (a hereditary disease that impairs the immune system)
Most vulvar cancers are caused by persistent human papillomavirus (HPV) infection.
Symptoms of Vulvar Cancer
Redness or a change in skin color of the vulva may be precancerous (indicating that cancer is likely to eventually develop).
Vulvar cancer usually causes unusual lumps or flat, smooth or rough, red, or flesh-colored sores that can be seen and felt and that do not heal. Sometimes the flat sores become scaly, discolored, or both. The surrounding tissue may contract and pucker. The sores may bleed. Melanomas may be bluish black or brown and raised. Some sores look like warts.
Many women have had itching in the vulvar area for a long time.
Typically, vulvar cancer causes little discomfort, but itching is common. Eventually, the lump or sore may bleed or produce a watery discharge (weep). These symptoms should be evaluated promptly by a doctor.
Diagnosis of Vulvar Cancer
Biopsy
Doctors diagnose vulvar cancer by taking a sample of the abnormal skin and examining it (biopsy). The biopsy enables doctors to determine whether the abnormal skin is cancerous or just infected or irritated. The type of cancer, if present, can also be identified, helping doctors develop a treatment plan. If the skin abnormalities are not well-defined, doctors apply stains to the abnormal area to help determine where to take a sample of tissue for a biopsy. Alternatively, they may use an instrument with a binocular magnifying lens (colposcope) to examine the surface of the vulva—a procedure called colposcopy.
Staging of vulvar cancer
Doctors stage vulvar cancer based on how large it is, where it is, and whether it has spread to nearby lymph nodes, which is determined during surgery to remove the cancer. Stages range from I (the earliest) to IV (advanced).
Stage I: The cancer is confined to the vulva.
Stage II: The cancer has spread to nearby tissues (the lower part of the urethra and/or vagina or to the anus) but not to nearby lymph nodes.
Stage III: The cancer has spread to the upper part of nearby structures or the lymph nodes.
Stage IV: The cancer has spread to distant sites (for example, outside the pelvis) or lymph nodes in the groin, forming sores or becoming stuck together or attached to bone.
Treatment of Vulvar Cancer
Removal of all or part of the vulva
Usually removal of nearby lymph nodes
For more advanced cancers, surgery and radiation therapy, often with chemotherapy
All or part of the vulva is surgically removed (a procedure called vulvectomy). Nearby lymph nodes are usually also removed. But sometimes doctors can instead do a sentinel lymph node dissection (removal of the first lymph node that would be affected by the cancer). Because basal cell carcinoma of the vulva does not tend to spread (metastasize) to distant sites, surgery usually involves removing only the cancer. The whole vulva is removed only if basal cell carcinoma is extensive.
To identify sentinel lymph nodes, doctors inject a blue or green dye and/or a radioactive substance into the vulva around the tumor. These substances map the pathway from the vulva to the first lymph node (or nodes) in the pelvis. During surgery, doctors then check for lymph nodes that look blue or green or that give off a radioactive signal (detected by a handheld device). Doctors remove this lymph node and send it to a laboratory to be checked for cancer. If it is cancer-free, no other lymph nodes need to be removed (unless they look abnormal). For early-stage cancers, such treatment is usually all that is needed. Doctors may remove sentinel lymph nodes on one or both sides of the vulva, depending on the size of the tumor.
If areas of cancer that measure less than 2 millimeters in size (called micrometastases) are detected in the sentinel lymph nodes, they are treated with radiation therapy. If the areas are larger (macrometastases), the lymph nodes in the groin are removed (lymphadenectomy).
For more advanced vulvar cancers, radiation therapy, often with chemotherapy, are usually used before vulvectomy. Such treatment can shrink very large cancers, making them easier to remove. Sometimes the clitoris and other organs in the pelvis must be removed.
For very advanced vulvar cancers, treatment may include surgery to remove all pelvic organs (called pelvic exenteration), radiation therapy, and/or chemotherapy. These organs include the reproductive organs (vagina, uterus, fallopian tubes, and ovaries), bladder, urethra, rectum, and anus. Which organs are removed and whether all are removed depend on many factors, such as the cancer's location, the woman's anatomy, and her goals after surgery. Permanent openings—for urine (urostomy) and for stool (colostomy)—are made in the abdomen so that these waste products can leave the body and be collected in bags.
After the cancer is removed, surgery to reconstruct the vulva and other affected areas (such as the vagina) may be done. Such surgery can improve function and appearance.
Doctors work closely with the woman to develop a treatment plan that is best suited to her and takes into account her age, sexual lifestyle, and any other medical problems. Sexual intercourse is usually possible after vulvectomy.
Prognosis for Vulvar Cancer
If vulvar cancer is detected and treated early, approximately 3 of 4 women have no sign of cancer 5 years after diagnosis. The percentage of women who are alive 5 years after diagnosis and treatment (5-year survival rate) depends on whether and how far the cancer has spread. Overall, the 5-year survival rate is approximately 70%.
Melanomas are more likely to spread than squamous cell carcinomas.
More Information
The following English-language resource may be useful. Please note that THE MANUAL is not responsible for the content of this resource.
National Cancer Institute: Vulvar Cancer: This web site provides links to general information about vulvar cancer, as well as links to information about causes, statistics, prevention, screening, treatment, and research and about coping with cancer.






